
Abstract
Purpose:
Single-incision laparoscopic appendectomy (SILA) for the treatment of appendicitis has been documented. Typically, SILA requires the use of specialized ports, instruments, and materials. The SILA technique at our institution utilizes the same instrumentation as the conventional laparoscopic approach (CLA), thus obviating the need for these specialized products. This study aims to further demonstrate the noninferiority of our SILA technique for the treatment of uncomplicated appendicitis.
Materials and Methods:
This is a single-institution retrospective review of patients who underwent SILA from 2011 to 2020 to treat uncomplicated appendicitis. Outcomes including demographics, operative time, length of stay (LOS), and common postsurgical complications were evaluated. These SILA cases were matched with up to 3 CLA controls based on age, gender, and weight utilizing the Greedy match method. Patients with an operative diagnosis of perforated appendicitis were excluded.
Results:
A total of 137 patients underwent SILA at a single institution. A total of 128 patients were in the final cohort after excluding perforated appendicitis. Mean age was 11.9 years. Case–control matching was conducted with 349 controls included. Between cases and controls, SILA had shorter operative time (27.2 minutes versus 43.7 minutes, P < .001) with no difference in mean LOS (42.4 hours versus 42.4 hours, P = .88). There was no difference in complication rate (5.4% versus 8.5%, P = .06). There was no difference in readmission rate (0.8% versus 3.4%, P = .108).
Conclusion:
These data suggest that for appropriately selected patients, our SILA technique is noninferior to CLA with shortened operative time.
Introduction
Single-incision laparoscopic appendectomies (SILAs) are performed in children and adults with appendicitis as an alternative to the conventional laparoscopic appendectomy three-port technique (CLA) or the open technique. The CLA approach involves multiple incisions through the abdominal wall to access the appendix, resulting in numerous scars and the potential for increased postoperative complications at the additional suture sites. SILA minimizes abdominal wall trauma and reduces scarring by completing the operation through a single incision in the umbilicus.
Multiple randomized controlled trials and meta-analyses demonstrate that SILA allows improved cosmetics over the CLA approach with comparable complication rates and pain scores.1–3 Traditional SILA techniques have shown high rates of conversion to CLA and longer operative times than CLA.1–5 The length of hospital stays and time to recover normal activity in SILA are shown to be significantly shorter than those in CLA in certain meta-analyses2,4,6 and insignificant in other meta-analyses.1,3,5,7 At our institution, SILAs are performed selectively in patients with appendicitis where surgeons determine the feasibility of cecal exteriorization and whether the appendix is confirmed to be nonperforated while utilizing laparoscopic vision.
To start, we use two regular 5 mm ports inserted through separate fascia openings but within the same infraumbilical incision (Figs 1 and 2). The cecum is then mobilized bluntly from lateral to medial. The two fascial incisions are bridged together to make a single centimeter size incision. The appendix is then exteriorized and the mesoappendix is ligated with ties and divided. Ligasure was also used at times. The appendix is divided at the base by either stapling or with an Endoloop, at surgeon's discretion.

The 5 mm trocar with laparoscope inserted.

Two standard 5 mm trocars placed in adjacent fascial incisions.
There are variations in reported SILA techniques that include those that utilize a telescope incorporated with a working channel, 8 a multichannel port, 9 or a glove port. 10 The outcomes of our specific technique applied in pediatric population are not known.
The specific aim of this study was to assess and compare the intraoperative complication rates, operative time, postoperative length of stay (LOS), and postoperative complications including wound infection, bleeding, herniation, and readmission among pediatric patients who underwent SILA and those who underwent CLA. We hypothesize that our SILA technique is noninferior to the CLA approach in both complication rate and length of hospital stay. If so, the SILA approach can be demonstrated as an advantageous alternative to the CLA approach by producing superior cosmetic outcomes without any increased risk of adverse events. Furthermore, our SILA technique remains a cost-effective approach, as it does not require any special single-incision equipment.
Materials and Methods
This is a retrospective single-pediatric center matched case–control study to evaluate the safety of the SILA technique. All pediatric patients who underwent SILAs or CLA in the past 10 years (January 1, 2011–December 31, 2020) were queried from our institutional database. Patients who had perforated appendicitis were excluded. For those who met the mentioned inclusion and exclusion criteria, individual patient charts were reviewed and queried for (1) demographics (age, gender, weight, and comorbidities), (2) intraoperative adverse events, (3) operative time, (4) postoperative LOS, and (5) postoperative adverse events.
Adverse events were any complications that occurred within the first 30 days after surgery. SILA patients were matched with CLA controls based on age, gender, and weight using the Greedy match method. The Greedy match method matches cases to controls based on their propensity to receive the intervention. It matches the case to the control with the minimal difference in propensity score within a predefined limit or as predetermined differences in specific variables.
We did a variable one to three match with equal gender. A 6-month difference was allowed for age matching and a 2 kg difference was allowed for weight matching. Mean procedure, mean LOS, return to emergency room (ER), unplanned readmissions, surgical site infection rate, postoperative bowel obstructions, and incisional hernias in SILA group were evaluated and compared against those of CLA control group.
Patient characteristics were compared between the cases and controls with chi-square and independent samples t-tests. Patient outcomes were compared between the groups with chi-square and t-tests. Simple linear and logistic regressions were performed on LOS, procedure, and operative time and development of any complications to obtain estimates of effect.
The rate of adverse intraoperative events, operative time, rate of postoperative adverse events, and LOS were calculated. The analysis of data for significant associations was performed using t-test for continuous variables and chi-squared or Fisher's exact test for categorical variables. Analysis of variance was used for comparisons of multiple groups. All analyses were performed using IBM SPSS version 28.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics are presented as frequencies and proportions for categorical variables. P < .05 was considered statistically significant.
Results
A total of 137 patients underwent SILA at a single institution. A total of 128 patients were in the final cohort after excluding perforated appendicitis and some chart duplications in the electronic medical record (Fig. 3
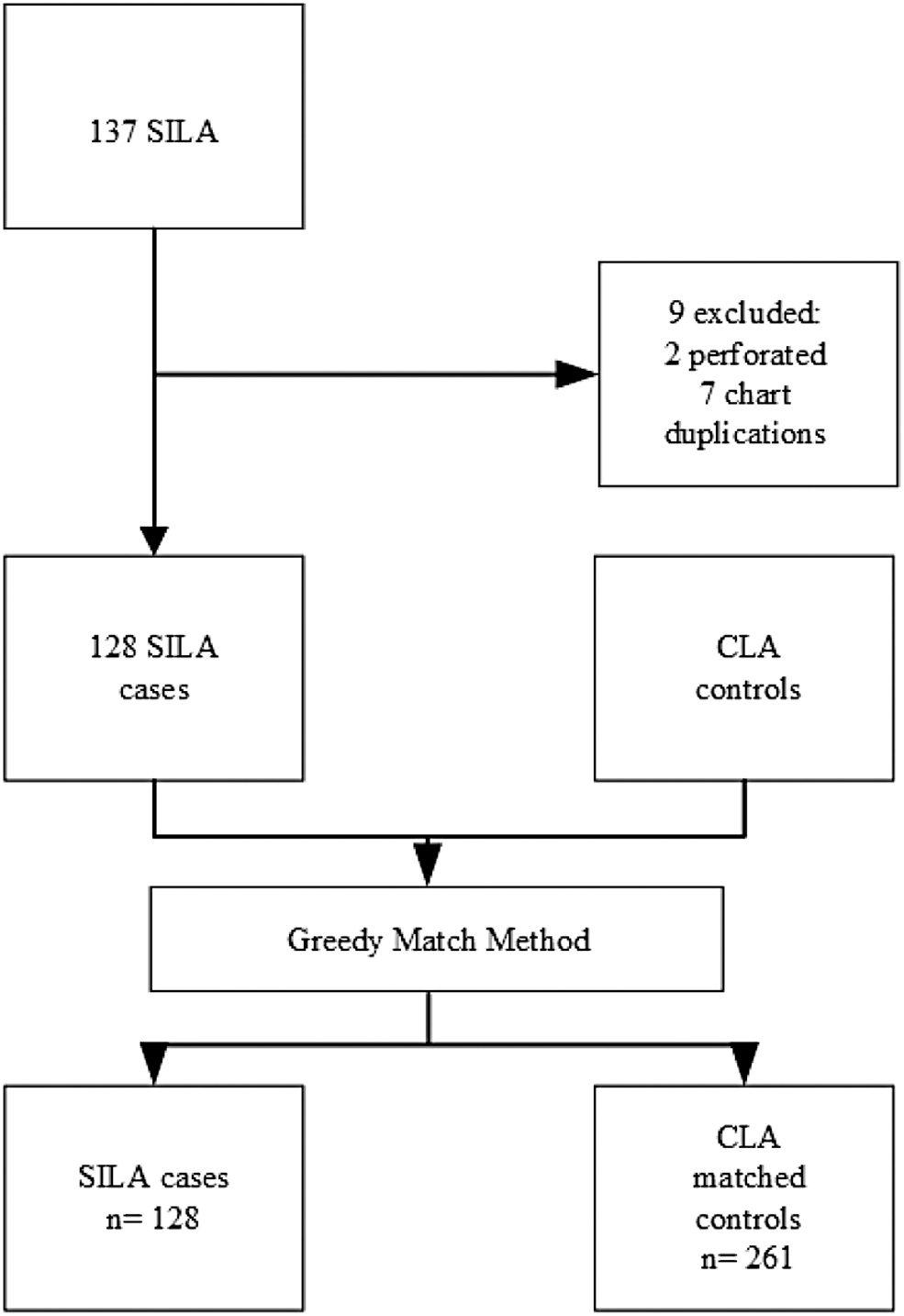
Greedy method case–control matching. CLA, conventional laparoscopic appendectomy; SILA, single-incision laparoscopic appendectomy.
Demographics and Clinical Characteristics
CLA, conventional laparoscopic appendectomy; IR, interventional radiology; NA, not available; SILA, single-incision laparoscopic appendectomy.
In addition, 2.9% unplanned readmissions occurred and 0% had reoperation. Case–control matching was conducted with 261 controls included. Between cases and controls, SILA had shorter operative time (27.2 minutes versus 43.7 minutes, P < .001) with no difference in mean LOS (42.4 hours versus 42.4 hours, P = .88). There was no difference in complication rate (5.5% versus 11.5%, P = .06). There was no difference in readmission rate (0.8% versus 3.4%, P = .108; Table 2
Outcome Metrics
CI, confidence interval; CLA, conventional laparoscopic appendectomy; ER, emergency room; LOS, length of stay; NA, not available; OR, operating room; odds ratio; SILA, single-incision laparoscopic appendectomy; SSI, surgical site infection.
Discussion
The results of this study are twofold. On the one hand, the objective results suggest that when patients are appropriately selected, our SILA technique is noninferior to CLA and results in shorter operative time. On the other hand, the actualization of this study implies that the technique employed at this institution is safe and feasible, not requiring the additional cost or separate purchase of SILA-specific instruments to achieve the same minimalized cosmetic outcomes afforded in other more traditional SILA operations.
Although our institution's technique may not be entirely novel where previous studies have reported success with multiple laparoscopic incisions being placed within the umbilicus,11–13 it is one of the first studies to be demonstrated on this scale and comparing outcomes against the CLA approach within the pediatric population. Other comparable studies have mainly involved one of the three previously reported SILA techniques.8–10 One study compared the single-incision technique utilizing a glove port wound protector (SILA-WP), the transumbilical approach of utilizing an 11 mm telescope with a 5 mm working channel (TULA) and CLA. 10
In patients with simple appendicitis, operation time of SILA was shorter than CLA but longer than TULA (62.8 ± 22.5 minutes versus 82.2 ± 24.3 minutes and 51.6 ± 22.3 minutes, P < .01). SILA-WP had shorter hospital stay than CLA, and similar to TULA (56.1 ± 20.4 hours versus 71.5 ± 37.8 hours and 56.9 ± 19.0 hours, P < .01). In patients with complicated appendicitis, SILA had shorter operation time than CLA, but a similar time to TULA (80.9 ± 22.4 minutes versus 105.7 ± 28.8 minutes and 82.5 ± 31.2 minutes, P < .01). These data reinforce what we found in our study. It also adds that SILA for complicated appendicitis is feasible and should be the next aim for applying this technique.
This study adds to the growing body of literature that supports the utilization of some sort of SILA technique as a safe alternative to CLA. This study demonstrates a shorter operative time is possible even without the more formal SILA instrumentation seen in other studies.
The obvious limitations of this study include those inherent to any retrospective study. More specific limitations to this study include our very selective inclusion criteria. Selected patients were those who had a thin body habitus such that cecal exteriorization could be performed with relative ease and those who were confirmed to be nonperforated on preoperative imaging. By implication, we included the easiest possible cases to undergo this technique.
Considering the controls, we did not account for the number of days this cohort had abdominal pain before their operation so although they may not have been perforated, some may have been clinically sicker with a more inflamed appendix, thus affecting operative metrics. This study also did not account for differences in pain score or perceived patient satisfaction with cosmesis as additional comparative factors between the two techniques. Future studies of this technique should account for complicated appendicitis as well as subjective scoring for pain and cosmesis.
Conclusions
This study is a unique contribution to the expansion of SILA. First, our data step outside the current standard approaches for SILA and show that an even simpler approach using traditional three-port instruments is noninferior to CLA for appropriately selected patients. Second, this study demonstrates that this SILA technique has shorter operative times without sacrificing other surgical outcome metrics. It remains that prospective randomized studies are required to further delineate the effectiveness of SILA over CLA, including in cases of complicated and perforated appendicitis.
Footnotes
Acknowledgment
The authors thank The Advanced HEAlth Data (AHEAD) Research Institute at Saint Louis University for its contributions in chart abstraction and statistical analysis.
Authors' Contributions
S.M. contributed to conceptualization, methodology, and supervision. J.R. was involved in data curation and writing—original draft preparation. M.V. and D.F. carried out data curation. J.G. took charge of conceptualization and methodology. A.E., C.S., M.K., C.B., and R.H. contributed to writing—review and editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.