
Abstract
Introduction:
Congenital partial duodenal obstruction (CPDO) is a rare type of intestinal obstruction, including webs and stenoses. Treatment has usually been operative by laparoscopy or laparotomy. Some have proposed endoscopic treatment due to a higher surgical risk in patients with CPDO. However, restenosis seems to be frequent after simple balloon dilatation.
Material and Methods:
We report on a patient with CPDO and complex esophageal atresia in whom we used a gastrojejunal tube to keep the lumen open after endoscopic balloon dilatation over a guidewire.
Results:
Follow-up endoscopy showed no evidence of restenosis. During the third endoscopy, the opening could be dilated to 15 mm without any complications and the gastrojejunal tube was removed. Since then, there were no clinical signs of obstruction, and no further endoscopic intervention was necessary.
Discussion and Conclusion:
Using a gastrojejunal tube after endoscopic balloon dilatation of a duodenal web may lower the risk of restenosis. This technique should be considered in patients with comorbidities and considerable surgical risk that have a gastrostomy in place.
Introduction
Congenital partial duodenal obstruction (CPDO) is a rare type of intestinal obstruction with an incidence of 1 in 10,000–40,000 live births. 1 The obstructing diaphragm is mostly found in the second part of the duodenum and can be of varying sizes. Therefore, symptoms can present postnatally or later in childhood. Treatment traditionally involves laparoscopic or open surgery.
However, CPDO is associated with a high rate of other anomalies and comorbidities. Especially for these patients, surgical intervention may lead to a higher risk of complications. It is also sometimes difficult to localize the obstructing web from outside the lumen. In rare cases, there may even be multiple webs in a row. 2 Therefore, endoscopic treatment of these patients makes sense and has been increasingly described in literature.1–5
We were faced with a patient with CPDO who was transferred to our service for further care of complex esophageal atresia and recurrent tracheoesophageal fistula. A gastrostomy had already been placed. However, nutrition through gastrostomy had not been possible due to recurrent nonbilious vomiting. Thus, intravenous nutrition had been established and had already led to highly elevated transaminases and beginning liver failure.
Materials and Methods
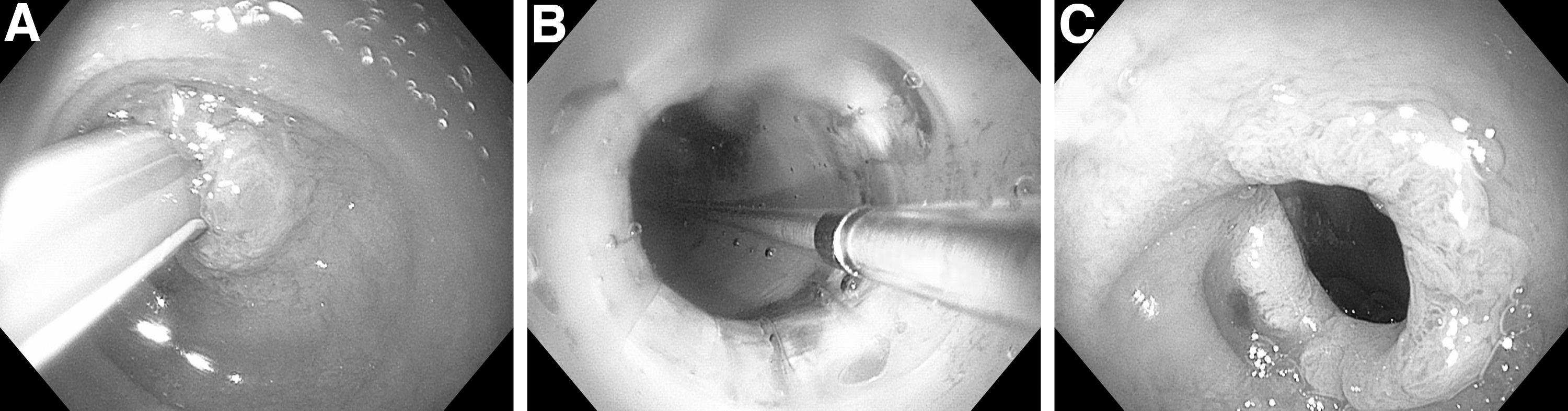
A 5-month-old male child with complex esophageal atresia was transferred to our service. Upon upper gastrointestinal endoscopy and bronchoscopy, a recurrent tracheoesophageal fistula was confirmed. In addition, duodenal obstruction was also found in the second part of the duodenum (Fig. 1A). The obstruction appeared as a diaphragm with a pinhole opening of ∼1–2 mm. The ampulla of Vater was not identified, indicating a prepapillary lesion.

Under direct visualization, a guidewire and balloon catheter was placed across the pinhole. The opening was dilated using the balloon dilator with an outside diameter of 10 mm (Fig. 1B). The balloon was expanded with normal saline under direct visualization and held for 3 minutes. Thereafter, visualization of the distal part of the duodenum was possible through the dilated opening, thus confirming a patent distal duodenum. After dilatation, the balloon was removed and a gastrojejunal feeding tube was advanced distally toward the jejunum (Fig. 1C).
Results
The gastrojejunal tube allowed intestinal nutrition and proximal gastric decompression. A Replogle tube was placed into the proximal esophagus to aspirate the secretions and allow the fistula to heal spontaneously. After 2 weeks, repeat endoscopy was performed, showing the gastrojejunal tube in place in a patent duodenum without restenosis. Also, the tracheoesophageal fistula had healed.
After another 4 weeks, a second endoscopic intervention was performed and showed adequate position of the tube (Fig. 2A) as well as no signs of restenosis. Nevertheless, a further dilatation of the opening to 15 mm was performed (Fig. 2B), after which the gastrojejunal tube was removed (Fig. 2C). Since then, nutrition was provided both orally and through a gastrostomy, gradually weaning the latter. So far, over a follow-up of 6 months, there were no clinical signs of restenosis and no further endoscopic intervention was necessary.
Discussion
Endoscopic treatment of CPDO has been successfully performed and reported in infants as a useful alternative in patients with comorbidities who may not tolerate operative interventions.1–5
Incision of the web by laser or electrocauterization, however, carries the risk of intestinal perforation and damaging the ampulla of Vater. 2 Therefore, we opted for balloon dilatation of the CPDO in our case, since it has not been associated with such complications so far.1,2 The reported major disadvantage of this type of endoscopic treatment is the necessity for multiple sessions of dilatation to reach complete resolution of the obstruction without restenosis. On average, two to four sessions have typically been described as necessary in the literature. 4 In our case, we believe that the gastrojejunal feeding tube left in situ prevented restenosis as documented in our case.
This case confirms that endoscopic balloon dilatation is a simple and effective method of treating partial duodenal obstruction. There were no complications during the procedure. The primary innovation of our approach is the postprocedural placement of a gastrojejunal tube that allows distal enteral feeding in between the sessions. Hereby, complications such as liver toxic effects of parenteral nutrition and the risk of restenosis in between the sessions may be avoided, and affording all the benefits of enteral feeding.6,7
Conclusions
Using a gastrojejunal tube after endoscopic balloon dilatation of a duodenal web to keep the lumen open after dilatation provides a mean of enteral feeding while dilatations are performed. It also may lower the risk of restenosis. This technique should be considered in patients with comorbidities and considerable surgical risk that have a gastrostomy in place. Further studies on the potential benefits of this technique are warranted, realizing that the constellation of CPDO and presence of a gastrostomy is rare.
Footnotes
Authors' Contributions
Performing the operation, writing of the article, and editing of figures by J.K. Performing the operation, supervision, reviewing, and editing of the article by O.M.
Ethics Approval
A formal ethics approval is not required for anonymous case reports at our institution. Written consent for the publication of the case and the pictures was provided by the parents.
Disclosure Statement
No competing financial interests exist. All authors completed the standardized ICMJE Disclosure form.
Funding Information
No funding was received for this article. Intramural funding only.