
Abstract
Introduction:
Cerebral and renal regional oxygen saturation (C-rSO2 and R-rSO2, respectively) were monitored using near-infrared spectroscopy in pediatric patients (range: 0.3–14.3 years) during minimally invasive surgery (MIS) taking at least 3 hours performed by laparoscopy (Lap), thoracoscopy (Tho), or retroperitoneoscopy (Ret) from January 2019 to December 2021.
Materials and Methods:
Criteria compared were operative time, preoperative/intraoperative hemoglobin, blood loss, mean arterial pressure, arterial partial pressure of carbon dioxide (PaCO2), peripheral oxygen saturation (SpO2), C-rSO2, and R-rSO2. Pathological desaturation (PD) was defined as >20% decrease from baseline, and statistical significance as P < .05.
Results:
Subjects (n = 79) were similar for gender, age, and body mass index. MIS procedures were: Lap = 45, Tho = 20, Ret = 14; one Lap case required conversion for severe adhesions, not PD. Intraoperative PaCO2 (mmHg) was significantly higher in Tho (maximum: 59.5 ± 17.0, minimum: 39.9 ± 7.5) versus Lap (maximum: 39.9 ± 5.1, minimum: 34.6 ± 3.9) and Ret (maximum: 37.8 ± 4.2, minimum: 35.0 ± 3.3); P < .0001 (maximum), P = .0013 (minimum). Minimum intraoperative SpO2 was significantly lower in Tho (P < .0001). Mean operative times were significantly shorter in Tho (259 ± 114 minutes) versus Lap (433 ± 154 minutes) and Ret (342 ± 100 minutes); P < .0001, respectively. PD was absent during Ret (C-rSO2: 0/14 = 0% and R-rSO2: 0/14 = 0%). Differences in PD for Lap (C-rSO2: 7/45 = 15.6% and R-rSO2: 10/45 = 22.2%) and Tho (C-rSO2: 9/20 = 45.0%, and R-rSO2: 7/20 = 35.0%) were significant; P = .0028 for C-rSO2 and P = .0497 for R-rSO2. Hemoglobin and blood loss were similar.
Conclusions:
PD was absent during Ret, despite longer operative times. If Ret is indicated for a procedure, neurodevelopmental sequelae of MIS could be minimized.
Introduction
With technological advancements, the repertoire of procedures that can be performed using minimally invasive surgery (MIS) has grown and successful reports of surgery in patients that may not be ideal for conventional open intervention, such as the super elderly and preterm/premature neonates are increasing. With patients at the extremes of the human lifespan, physiology is less robust and utmost care is required to maintain cardiovascular function and tissue oxygenation.
While MIS is known to be associated with quicker recovery and less requirement for analgesia, 1 the impact of insufflation is unavoidable.2–4 Several articles report increased intra-abdominal pressure and reduced renal perfusion secondary to pneumoperitoneum during laparoscopy (Lap),5,6 an association between thoracoscopy (Tho) and risks for hypercapnia and acidosis during pneumothorax that can be severe, particularly in children, as well as hemodynamic derangement that can induce cerebral oxygen desaturation.3,4
Reports about complications and technical aspects of MIS abound in the literature, but few focus on tissue oxygenation and sequelae of desaturation during MIS. In an earlier published study, the authors reported evidence of the profound fragility of neonatal vascular perfusion compared with older pediatric patients using intraoperative near-infrared spectroscopy (NIRS). 7 NIRS enables real-time monitoring of tissue oxyhemoglobin and deoxyhemoglobin for measuring tissue oxygen uptake and consumption, 8 providing data for oxygen demand, oxygen extraction, and oxygen reserve 9 used to calculate regional oxygen saturation (rSO2). NIRS is sensitive and monitoring dynamic changes in rSO2 can identify resaturation faster than percutaneous oxygen saturation monitoring. 10
The aim of this study was to determine cerebral and renal rSO2 (C-rSO2 and R-rSO2, respectively) using NIRS during pediatric MIS procedures performed using Lap, Tho, and retroperitoneoscopy (Ret) to determine differences in physiological impact as reflected by the incidence of pathological desaturation (PD) in rSO2.
Materials and Methods
Subjects were Japanese pediatric patients whose caregivers consented to participate in an observational prospective study on the impact of MIS monitored using NIRS. The study was performed at a single institution from January 2019 to December 2021 by a single team of board-certified pediatric surgeons with specialist qualifications in MIS. All procedures had scheduled operative times of at least 3 hours. NIRS (INVOS 5100C; Covidien, Boulder, CO) sensors were applied to the forehead (C-rSO2) and flanks (R-rSO2) of each subject after induction of general anesthesia and removed after extubation or on exiting the operating room if postoperative intubation was required. Recordings were analyzed using the INVOS Monitoring System Analytics Tool software, provided by Covidien.
Criteria compared were: gender ratio, age at the time of surgery, body mass index (BMI), operative time, preoperative hemoglobin, hemoglobin from intraoperative blood gas measurement, blood loss, mean arterial pressure (MAP), MAP ratio (ratio of minimum to maximum MAP), arterial partial pressure of carbon dioxide (PaCO2), peripheral oxygen saturation (SpO2), C-rSO2, and R-rSO2. PD in C-rSO2 and R-rSO2 was defined as >20% decrease from preoperative baseline levels. PD ratio (ratio of minimum rSO2 to baseline rSO2; maximum PD ratio, indicating no change in perfusion related to surgery was 1) was also calculated to reflect intraoperative stability of vascular perfusion for each MIS technique.
Statistical analyses were performed with GraphPad Prism 9 (GraphPad Software, Inc., SanDiego, USA). Categorical data were analyzed using the chi-square test. Continuous data were analyzed using the one-way ANOVA. A P-value of <.05 was considered statistically significant.
This study was approved by the Institutional Review Board at Juntendo University School of Medicine (H20-0227) and complies with the Helsinki Declaration of 1975 (revised 1983).
Results
Subjects were 79 Japanese children from 0.3 to 14.3 years of age. Pediatric MIS procedures performed were: Lap: pull through for Hirschsprung's disease (n = 12), anorectoplasty for anorectal malformation (n = 11), choledochal cyst excision with hepaticojejunostomy anastomosis (n = 10), Nissen fundoplication (n = 4), Kasai portoenterostomy (n = 3), ectopic kidney resection (n = 2), adrenalectomy (n = 1), and tumor resection (n = 2); Tho: lung lobectomy (n = 12), mediastinal tumor resection (n = 6), esophageal anastomosis (n = 1), and diaphragmatic hernia repair (n = 1); and Ret: pyeloplasty (n = 12) and nephrectomy (n = 2).
The three groups had similar gender ratios, mean weights at surgery, mean heights at surgery, and mean BMI at surgery. Specifically, gender ratios (male:female) were: Lap (28:17), Tho (7:13), and Ret (9:5); P = .097, mean ages (years) at surgery were: Lap (3.4 ± 3.5), Tho (5.1 ± 4.8), and Ret (5.6 ± 2.8); P = .093, mean weights (kg) at surgery were: Lap (14.5 ± 9.4), Tho (18.9 ± 14.7), and Ret (20.3 ± 5.6); P = .122, mean heights (cm) at surgery were: Lap (89.8 ± 26.9), Tho (101.4 ± 32.8), and Ret (107.7 ± 16.4); P = .068, and mean BMI (kg/m2) at surgery were: Lap (16.6 ± 1.8), Tho (15.9 ± 2.0), and Ret (17.3 ± 2.2), P = .105 (Table 1).
Subject Demographics (n = 79)
BMI, body mass index.
Data for MAP, MAP ratios, preoperative hemoglobin, intraoperative blood gas hemoglobin, and blood loss were also similar. Specifically, maximum MAP (mmHg) were: Lap (85.2 ± 14.2), Tho (79.0 ± 11.9), and Ret (89.8 ± 13.9); P = .078, minimum MAP (mmHg) were: Lap (51.5 ± 7.9), Tho (52.0 ± 6.8), and Ret (57.2 ± 10.1); P = .077, MAP ratios were: Lap (0.63 ± 0.12), Tho (0.67 ± 0.10), and Ret (0.64 ± 0.11); P = .24, mean preoperative hemoglobin (g/dL) were: Lap (12.5 ± 1.3), Tho (12.2 ± 2.0), and Ret (13.3 ± 0.9); P = .12, minimum intraoperative blood gas hemoglobin (g/dL) were: Lap (10.4 ± 1.4), Tho (10.7 ± 1.4), and Ret (11.5 ± 1.1); P = .068, and mean Table 2 blood loss (g) was: Lap (9.7 ± 11.0), Tho (5.6 ± 10.4), and Ret (6.2 ± 4.7); P = .25 (Table 2).
Subject Operative Data (n = 79)
MAP, mean arterial pressure.
Mean operative times were significantly shorter in Tho, minimum SpO2 were significantly lower in Tho, and PaCO2 were significantly higher in Tho. Specifically, operative times (minutes) were: Tho (259 ± 114 minutes), Lap (433 ± 154 minutes), and Ret (342 ± 100 minutes); P < .0001, minimum SpO2 (%) were: Tho (89.5 ± 11.4), Lap (97.4 ± 3.0), and Ret (97.9 ± 1.2); P < .0001, PaCO2 (mmHg) were: Tho (maximum: 59.5 ± 17.0, minimum: 39.9 ± 7.5), Lap (maximum: 39.9 ± 5.1, minimum: 34.6 ± 3.9), and Ret (maximum: 37.8 ± 4.2, minimum: 35.0 ± 3.3); P < .0001 for maximum PaCO2 and P = .0013 for minimum PaCO2, respectively (Fig. 1).

Intraoperative gas exchange data according to MIS technique. MIS, minimally invasive surgery; PD, pathological desaturation; PD ratio, minimum/baseline rSO2; Lap, laparoscopy; Ret, retroperitoneoscopy; rSO2, regional oxygen saturation; Tho, thoracoscopy.
PD were absent in Ret (C-rSO2: 0/14 = 0% and R-rSO2: 0/14 = 0%). PD in Lap were (C-rSO2: 7/45 = 15.6% and R-rSO2: 10/45 = 22.2%) and Tho were (C-rSO2: 9/20 = 45.0% and R-rSO2: 7/20 = 35.0%). Differences were significant; P = .0028 for C-rSO2 and P = .0497 for R-rSO2, respectively (Table 3). PD ratios were significantly higher in Ret (C-rSO2: 0.92 ± 0.06 and R-rSO2: 0.96 ± 0.03) compared with Lap (C-rSO2: 0.89 ± 0.07 and R-rSO2: 0.85 ± 0.12) and Tho (C-rSO2: 0.79 ± 0.12 and R-rSO2: 0.85 ± 0.10); P < .0001 for C-rSO2 and P = .0043 for R-rSO2, respectively (Fig. 2).
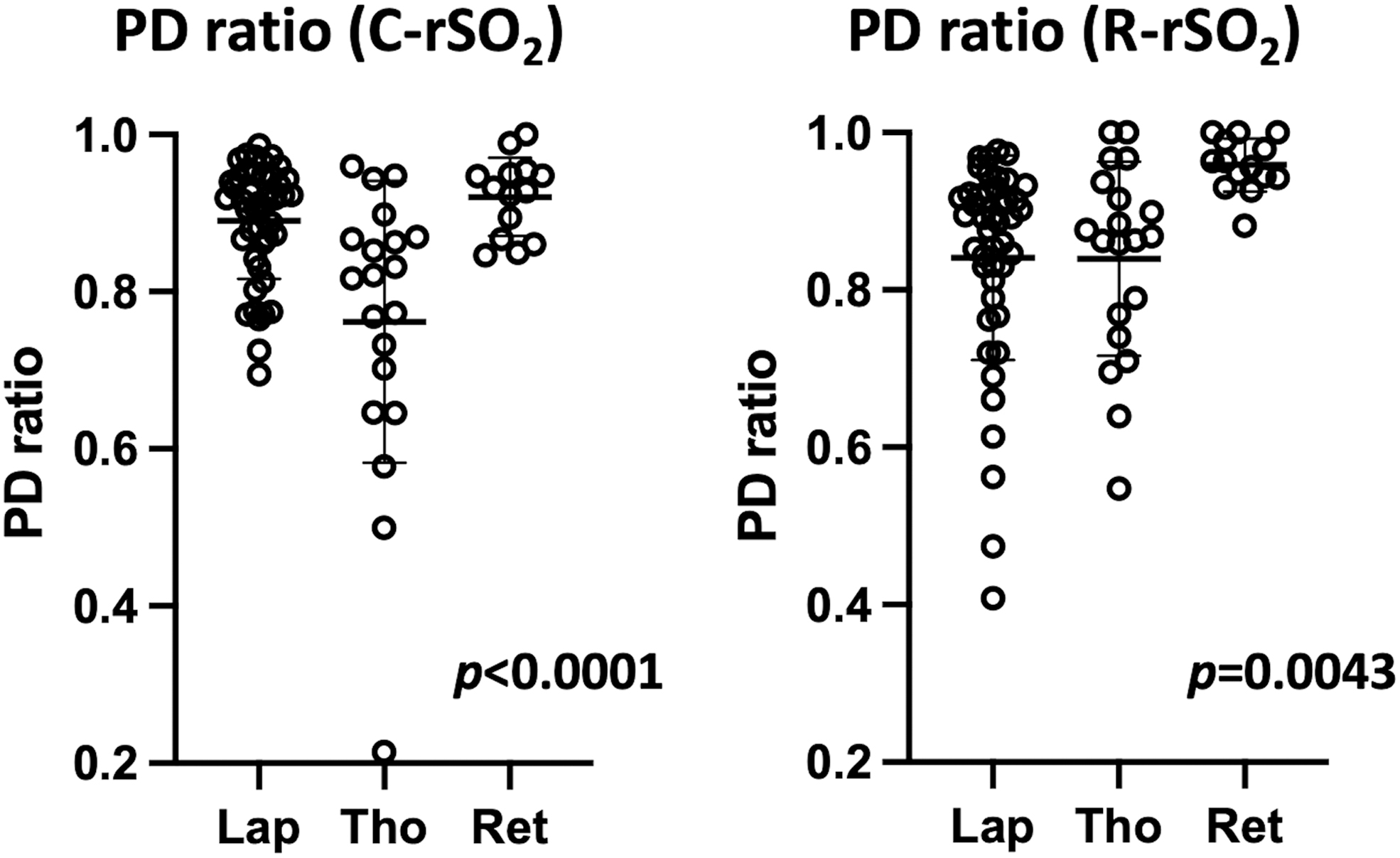
PD ratios according to MIS technique. MIS, minimally invasive surgery; PD, pathological desaturation; PD ratio, minimum/baseline rSO2; Lap, laparoscopy; Ret, retroperitoneoscopy; Tho, thoracoscopy; rSO2, regional oxygen saturation.
Incidence of Pathological Desaturation in rSO2
C-rSO2, cerebral regional oxygen saturation; rSO2, regional oxygen saturation; R-rSO2, renal regional oxygen saturation.
Discussion
From the finding that PD did not occur during Ret for MIS procedures taking at least 3 hours in pediatric cases, Ret would appear to be associated with more stable perfusion than Lap or Tho. While Ret subjects tended to be older and larger, differences were not statistically significant. Compromised ventilation during Tho and manipulation of abdominal organs during Lap could be expected to influence PD but the difference between Ret and Lap/Tho was unexpectedly distinct. This trend is worth considering when planning surgery for procedures that can be performed using alternative techniques.
Obviously, Tho compromises ventilation; minimum SpO2 was significantly lower and both maximum and minimum PaCO2 were significantly higher in Tho than Lap and Ret in this study. Bishay et al reported that cerebral oxygenation can also be decreased by hypercapnia and acidosis secondary to increased CO2 absorption during pneumothorax. 3 On the other hand, Lap causes compromise related to intra-abdominal pressure with insufflation limiting respiratory movements and perfusion affected by pressure on vessels and manipulation of abdominal organs. Pelizzo et al reported that decreased cerebral oxygen saturation correlated with increased intra-abdominal pressure during pediatric laparoscopic inguinal hernia repair. 11 In an earlier report by the authors, PD in R-rSO2 was observed immediately in all procedures requiring reduction of viscera into the abdominal cavity, and seemed to be related directly to increased intra-abdominal pressure. 7 From these perspectives, lack of PD seen during Ret procedures could be related to PaCO2 and abdominal pressure resulting in stable rSO2.
MIS procedures that can be performed using Ret in children are limited to urology, but some can be performed using Lap with no consensus about which approach is preferable among pediatric surgeons and pediatric urologists.12–14 The reality is that few surgeons choose Ret because the retroperitoneal space is small, the operative field tends to get crowded by instruments, or less trocars are used, and maneuverability suffers.15,16 Robotic surgical systems add extra restraints because trocars must be a certain minimum distance apart. The working space is larger with Lap, enabling more instruments to be used 12 and as a result, some articles have even reported that Lap is thus faster, safer, and technically easier than Ret.12,13,16 These articles focus on technicalities without discussing any issues related to tissue oxygenation. Despite lack of PD during Ret, operator confidence and safety will be more influential when planning how to perform a procedure; few surgeons will opt to choose an approach based purely on oxygen saturation.
Nevertheless, while logistically, Ret is at a disadvantage, pediatric patients have yet to complete full neurological development and any potential cause for PD must be minimized, or prevented. Pediatric patients potentially have many decades of postoperative life after successful surgery, so tissue oxygenation should be an important topic for pediatric surgeons to consider when planning surgery. Thus, Kussman et al reported that intraoperative PD in C-rSO2 is a risk factor for reduced neurodevelopment in infants using the Psychomotor Development Index and brain magnetic resonance imaging, 17 Hoffman, et al reported that perioperative C-rSO2 was correlated with neurodevelopmental performance in preschool-aged children, 18 and Sood et al reported that patients with lower perioperative C-rSO2 had lower receptive communication scores. 19 On the other hand, active monitoring of perioperative C-rSO2 has been reported to be adequate for reducing postoperative neurological complications, such as seizures, cerebral infarct, and speech problems. 20
While this study has limitations because it was an analysis from one center involving a small number of subjects, it identified that Ret has stable tissue oxygenation with no documented PD. Although Ret should be considered actively when indicated, the working space needs to be adequate for success. Thus, Ret is only likely to be used in selected patients to ensure safety although lack of PD is of high priority for normal neurological development. In this study, the correlation between PD and neurodevelopmental outcome was not investigated and a long-term follow-up study on the impact of PD could reveal the optimal threshold for rSO2, and allow it to be incorporated into surgical planning.
Conclusions
PD was not observed in Ret, and PD ratios were highest for Ret suggesting that oxygenation during Ret is more stable than during Lap or Tho. Although customization is the norm in pediatric surgery, preventing deleterious events could contribute as much or more than mastering technical skills and management. Awareness that Ret procedures are not associated with PD is unlikely to be common knowledge and could help improve the acceptance of Ret for pediatric MIS procedures.
Footnotes
Authors' Contributions
Y.M.: conceptualization, methodology, and writing (original draft preparation); K.F.: formal data analysis; K.K., T.O., and S.S.: collation of data, H.K.: study administration; G.J.L.: writing (native English editing and reviewing); K.N.: resource management; M.H.: methodology; A.Y.: supervision.
Acknowledgments
The authors gratefully acknowledge the work of past and present members of their department.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.