
Abstract
Introduction:
Massive splenomegaly in children can complicate minimally invasive splenectomy. Splenic artery embolization (SAE) before splenectomy has been shown to decrease splenic volume, reduce intraoperative blood loss, and decrease conversion rates in laparoscopic surgery. Our objective was to review our recent experience with immediate preoperative SAE in massive splenomegaly for pediatric patients using both laparoscopic and robotic techniques.
Materials and Methods:
We retrospectively reviewed preoperative SAE outcomes in pediatric patients with massive splenomegaly undergoing minimally invasive splenectomy between January 2018 and July 2021.
Results:
Four patients, 3 female, ages 5–18 years, had SAE immediately before minimally invasive splenectomy. Two cases were completed robotically, one laparoscopically, and one laparoscopic case required conversion to open. SAE time ranged from 69 to 92 minutes. Time between embolization and surgical start ranged from 26 to 56 minutes, with operative times from 153 to 317 minutes. Estimated blood loss ranged from <10 to 150 mL. Mean length of stay was 3.5 days (range 2–6). Postoperative complications included one patient with ileus and another with concurrent gastritis and urinary tract infection. Splenic size comparisons were difficult to perform due to morselization of the spleen; however, excised spleen weights, measurements, and surgeon's impression suggested decreased size of the spleen after SAE. There were no transfusions, postembolization complications, or deaths.
Conclusion:
SAE subjectively appears to decrease splenic distension, which should allow for easier manipulation and possibly better visualization of splenic hilar vessels during minimally invasive surgery. Immediate preoperative SAE is safe and feasible and should be considered in pediatric patients with massive splenomegaly.
Introduction
Splenomegaly has an overall prevalence of 2% in the United States. 1 In children, splenomegaly is usually secondary to hemolytic anemias, malignancy, infection, hereditary storage disorders, or benign masses. 2 Symptoms include early satiety, abdominal pain, dyspnea, referred pain to the left shoulder, and an associated abdominal mass. Patients with splenomegaly are at an increased risk of serious complications such as symptomatic cytopenias, intestinal obstruction, and catastrophic splenic rupture. 1 Indications for splenectomy in children not due to trauma include refractory cytopenias, splenic sequestration crisis, malignancy, symptomatic splenomegaly, and massive splenomegaly.3,4
In adults, massive splenomegaly is defined as >20 cm or a splenic weight >1000 g. 5 In pediatric patients, spleen size varies with growth, and there remains debate around the ideal criteria. 6 The European Association for Endoscopic Surgery (EAES) definition of pediatric massive splenomegaly is a spleen larger than four times normal for the age, whereas some studies have used four times the ideal size based on weight, and others have used a splenic weight >500 g.5,7 Massive splenomegaly is important to identify because splenectomies in these patients are associated with higher rates of intraoperative bleeding, longer operative times, and increased conversion rates to open with minimally invasive surgery. 8 The 2008 EAES guidelines even recommend a preference for hand-assisted laparoscopic or open approaches in massive splenomegaly, although this has since come into question.5,9–13
Preoperative splenic artery embolization (SAE) has been shown to reduce intraoperative blood loss, conversion rates, operative time, serious perioperative complications, and splenic volume in patients with massive splenomegaly.10,14 SAE is not without risks, with complications including postembolization pain syndrome, coil migration, iatrogenic pancreatitis, and splenic artery rupture. Prolonging the time between embolization and splenectomy, even by just several hours, has an increased risk of postembolization syndrome.14,15 We elected to perform SAE immediately before splenectomy under the same anesthesia for this reason. There is some concern that performing the surgery immediately after SAE may limit the amount of volume reduction, but some volume reduction has still been shown to occur for most patients.10,14
Our objective was to review our early single-center experience in children with massive splenomegaly who underwent robotic or laparoscopic splenectomy immediately preceded by SAE. We hypothesized that this approach would result in smaller splenic size at surgery, decreased blood loss, and increase the feasibility of minimally invasive techniques without an increase in SAE associated complications.
Materials and Methods
Institutional Review Board approval was obtained for a retrospective review of four cases between January 2018 and July 2021. Patient consent was not required owing to the retrospective nature of the study. Patients included were 18 years of age or younger at the time of surgery, with massive splenomegaly of any cause, and who underwent preoperative SAE followed by minimally invasive splenectomy. Patient demographics collected included age, sex, weight, body mass index (BMI), prior surgeries, comorbidities, preoperative symptoms, laboratories, splenic size, and reason for splenomegaly. Operative variables included splenic embolization technique, SAE time, time to surgery, operative technique, operative time, estimated blood loss, splenic size, and weight. Postoperative complications and laboratories were evaluated for the duration of the hospital stay, at any recurrent visit related to the primary hospitalization and at planned follow-up visits.
Before SAE, patients were intubated and sedated under general anesthesia. SAE was then performed by a board-certified pediatric interventional radiologist. All patients underwent initial particle embolization of the main splenic artery branches with subsequent coil embolization of the distal main splenic artery as previously described by Van Der Veken et al. 10 Individual particle type and coil selection were based on anatomic constraints. Two patients underwent additional coil embolization to branches of the main splenic artery. Care was taken to preserve flow to the pancreatic and gastric arterial branches originating from the splenic artery, which was confirmed by angiogram (Fig. 1). Patients were then transported directly to the operating room. For the cases completed laparoscopically or robotically, spleens were morselized before removal from the abdomen. In the case converted to open, the spleen was removed en bloc, and the intact volume was measured by pathology.

Angiogram (Case 3) after splenic artery embolization demonstrating near complete blockage of blood flow to spleen with coils noted in the distal main splenic artery.
Ideal splenic volume in milliliter for the pediatric patient was calculated based on body weight from the formula (0.7 + [4.6 × Body Weight]). 16 Preoperative splenic measurements were determined by either ultrasound or computed tomography (Fig. 2). Estimated splenic volume was then calculated using the formula for the volume of an ellipse (0.523 [length × width × height]). 17 Estimated splenic weight was additionally calculated, based on the formula (0.43 [length × width × height]). 18 Postoperative splenic weight was reported by pathology. Descriptive statistical analysis was performed using GraphPad Prism version 9.3.0 for Windows, GraphPad Software, San Diego, CA, USA, www.graphpad.com. Categorical variables are reported as frequencies (%). Continuous variables are reported using mean (range).
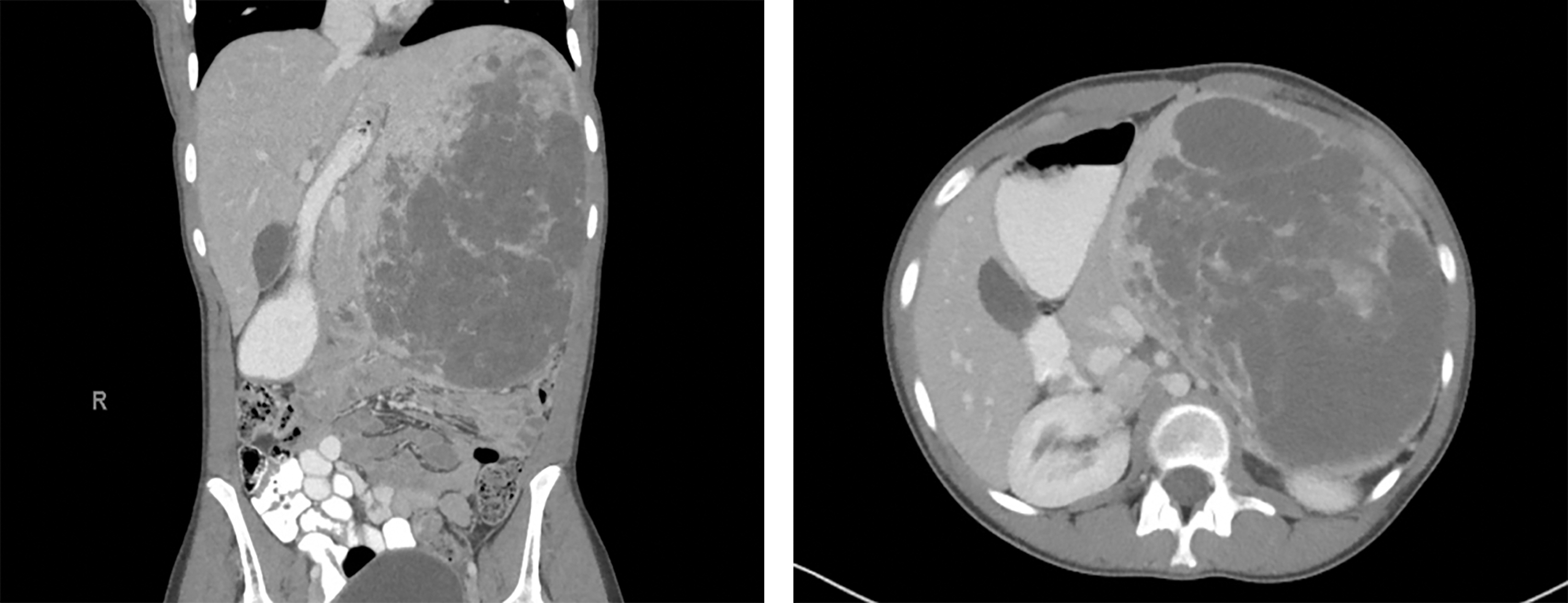
Preoperative computed tomography (Case 1) demonstrating massive splenomegaly in a coronal view (left) and axial view (right).
Results
Four patients, 3 females, underwent splenectomy with preoperative SAE between January 2018 and July 2021. Mean age was 13.3 years (5–18) with a mean preoperative BMI of 22.26 kg/m2 (15.75–34.21; Table 1). Only 1 patient had undergone prior abdominal surgery, a robotic cholecystectomy. The most common preoperative complaint was abdominal pain, and all patients suffered from anemia. Causes of splenomegaly included thalassemia, sickle cell disease, hereditary spherocytosis, and hemorrhagic pseudocysts. Spleens were on average 5.9 (3.1–10.3) times larger by volume than expected based on body weight and had an estimated weight of 1104.8 g (373–1988; Table 2).
Patient Variables
BMI, body mass index.
Splenic Measurements
Estimated/ideal splenic volume = (0.523 [length × width × height])/(0.7 + [4.6 × Body weight]).
Estimated pre-op splenic weight (g) = 0.43 (length × width × height).
All patients were successfully embolized without complication with a mean embolization time of 83.5 (69–92) minutes (Table 3). Mean time from completion of SAE to surgical incision was 41.3 (26–56) minutes. Average operative length was 200.3 (122–317) minutes, with the longest procedure additionally including a cholecystectomy and cholangiogram. Two cases were completed robotically, one laparoscopically, and one laparoscopic case was converted to open to obtain improved visualization of the hilar vessels. The open case had 125 mL estimated blood loss, with the other cases having minimal blood loss. Due to morselization, splenic size comparisons were difficult to extract; however, excised spleen weights and surgeon's impression suggested decreased size of the spleen after SAE (Table 2).
Operative Variables
PVA, polyvinyl alcohol; SAE, splenic artery embolization; UTI, urinary tract infection.
Mean postoperative length of stay was 3.5 (2–6) days with the patient (Case 4) kept for 6 days due to prolonged postoperative ileus. Interestingly, this is the same patient who required concomitant cholecystectomy with cholangiogram due to recent biliary pancreatitis. One additional patient returned to the hospital for concurrent urinary tract infection and gastritis, which resolved with IV fluids, Famotidine, and antibiotic. No patients required transfusions, and all patients were doing well with normal laboratories at 30-day follow-up. There were no cases of postembolic pain syndrome, pancreatitis, or remnant accessory spleens noted.
Discussion
Data suggest that those with massive splenomegaly are at increased risk for complications; thus, preoperative identification of patients with massive splenomegaly is critical. Patel et al determined that adults with massive splenomegaly had a significantly longer median operation time (170 minutes versus 102 minutes, P < .01), higher incidence of postoperative morbidity (55.6% versus 4.9%, P < .01) with common complications of atelectasis (7%) and secondary hemorrhage (6%), and longer median postoperative hospital length of stay (5 days versus 3 days, P < .01). 8 Laparoscopic splenectomy is associated with a conversion rate up to 19.56%, with massive splenomegaly having conversion rates as high as 37.5%.10,19 The limited studies discussing splenectomy in massive splenomegaly in children do not report their comparisons to splenectomy in normal spleens. Despite high conversion rates and longer operating times, minimally invasive splenectomy in massive splenomegaly has been associated with decreased morbidity, mortality, transfusions, postoperative pain, and shorter hospital stays.7,13,20 Early reports suggest decreased need for conversion with robotic surgery, which aligns with our results as both robotic cases were completed successfully without conversion. 21
Using an estimated (calculated) over ideal splenic volume based on body weight is a reliable indicator for massive splenomegaly in pediatric patients with a normal BMI. 10 However, this calculation may be less reliable in obese children as the formula for expected volume based on body weight has not been validated in children with a weight of over 75 kg. 16 We suspect that using body weight in case 2 likely resulted in an overestimation of ideal volume with a ratio of only 3.1 times larger than expected ideal volume, despite the spleen's size nearly meeting the adult definition of massive splenomegaly. Case 2 met additional criteria for massive splenomegaly by being both greater than four times expected for age range and for being >500 g.6,21 We chose to estimate splenic weight based on the formula described by Downey, which has been previously used in related literature, although this is likely a conservative estimation and may underestimate splenic weight.7,22
Given the massive splenomegaly in our patients, we chose to pursue preoperative SAE. This was done in an effort to reduce the splenic blood flow, thereby minimizing intraoperative risk for hemorrhage and to decrease splenic volume to facilitate minimally invasive surgery. Reports of SAE before splenectomy in splenomegaly have been described in limited instances in the pediatric population and have never been described for robotic splenectomy.10,15 In a prospective study evaluating preoperative embolization in 16 pediatric patients, 8 of which had massive splenomegaly, 94% of patients experienced less than 20 mL of blood loss, with only 1 patient suffering a complication of splenic artery perforation and a 250 mL blood loss. 10 This is consistent with our findings in our 2 patients who underwent minimally invasive surgery both having <10 mL of blood loss and an additional patient having 25 mL. In our patient that required conversion to an open procedure, there was a blood loss of 150 mL, but it was still felt that preoperative SAE allowed for significantly decreased blood loss. In the prospective study, all eight cases of massive splenomegaly were completed laparoscopically using SAE, with the largest spleen being eight times larger than expected. In our patient that required conversion, the spleen was 10 times the ideal size, which suggests the challenges of successful completion above a certain size. Mild complications occurred in 2/4 of our patients that were likely unrelated to the minimally invasive mode of removal and/or SAE. One patient returned to the hospital and was found to have a urinary infection with concomitant gastritis. Both conditions resolved with antibiotic and supportive care. An additional patient had a postoperative ileus which resulted in a prolonged hospital stay of 6 days which resolved with supportive care and postoperative narcotic wean. This is consistent with Van Der Veken et al study in pediatric patients where 50% (8/16) of patients had minor complications. 10 The group's reported complications related to SAE included one splenic artery rupture and asymptomatic elevations in amylase. Additional complications included pleural effusions, pneumonia, acute chest syndrome, and a subphrenic abscess. Although no pediatric study has directly compared SAE to laparoscopic splenectomy without SAE, one study in 79 adults found that using SAE reduced operating time, intraoperative blood loss, and postoperative stay. 14 Specifically, it was found that patients that had both preoperative embolization and laparoscopic surgery experienced an estimated blood loss of 47.0 ± 27.6 mL and an average operating time of 166.3 ± 29.3 minutes, compared to patients that had laparoscopic surgery alone, who had an estimated blood loss of 223.8 ± 209.2 mL and an average operating time of 177.6 ± 69.5 minutes. This is consistent with our mean operating time of 161.3 minutes (122–209) when excluding case 4, which had an additional cholecystectomy and cholangiogram.
Debate remains surrounding the optimal timing between preoperative embolization and splenectomy. If the procedures must be scheduled for different days, patients often experience significant postembolic pain until they undergo splenectomy. 14 Takahashi et al reported postembolic pain in 5/5 children who underwent SAE the day before splenectomy; however, they did not report postoperative splenic volume. 15 Wu et al found that waiting an average of 3.8 hours led to a reduction in splenic volume in 16/20 patients, but 6/20 patients complained of significant pain. 14 One way to avoid postembolic pain is by combining the two procedures under the same anesthesia; however, this may limit the benefit in volume reduction. There are limited data regarding changes in splenic volume when SAE is performed immediately before splenectomy, as there is no currently recognized way to compare morselized specimens to preoperative imaging in humans. 23 Despite this, there are subjective reports by surgeons of softer and smaller spleens after SAE, which helped facilitate a successful procedure.10,15 For these reasons, we elected to perform splenectomy under the same anesthesia as SAE with a mean time between procedures of 41.3 (26–56) minutes. We purposely used the more conservative formula to estimate preoperative splenic weight and still noted a decrease in weight. Because the spleen from case 1 was resected intact, we were able to compare the volumes from preoperative imaging to the findings on pathology. Despite only waiting 56 minutes there was a 14% decrease in volume (2417–2089 mL). This suggests that even a short duration can result in decreased splenic volume. It is our belief that cases 2–4 were able to be completed with minimally invasive techniques due to the reduction in splenic volume.
Interestingly, the embolization technique used may also change the postoperative outcomes. Li et al prospectively found that patients who underwent preoperative splenic embolization using a combination of iodized oil and gelatin sponge experienced decreased blood loss during surgery compared to conventional splenic artery occlusion with laparoscopic splenectomy. 24 In a small study of 5 children who underwent preoperative SAE, 4 had gelatin sponge embolization and 1 had microcoil embolization. 15 There were no embolization complications in our cohort, and of note a single embolization technique was used. We elected to follow the technique suggested by Van Der Veken et al, using particle embolization followed by splenic artery coil placement. 10 This technique has the added benefit of both limiting reflux to collateral circulation and results in complete vascular obstruction with minimal to no bleeding. Our approach resulted in no embolization complications, no transfusions, and no deaths. Of note, the presence of embolization coils within the splenic artery did not preclude adequate hemostasis when using a vascular stapler, which was used for hilar control in laparoscopic and robotic cases. Coils were easily crossed, clamped, and cut, still allowing excellent vessel coaptation and hemostasis without the creation of coil particles within the abdomen. Certainly, further studies are needed to truly compare immediate preoperative SAE to minimally invasive ligation of the splenic artery with some short period of waiting for the splenic size to go down. The difficulty will be known if the spleen is truly without arterial blood supply, as this can be difficult to ascertain and there is significant collateral flow. Furthermore, using this alternative technique might not provide the added benefit of less blood loss during the initial dissection.
Despite the benefits of preoperative embolization, this technique has not been widely accepted thus far. One of the biggest challenges is the difficulty of arranging embolization and surgery together under the same anesthesia. 10 In addition, etiology of the splenomegaly is important to consider when contemplating using preoperative SAE. While using this approach may reduce the operative time and intraoperative blood loss, there is a risk of precipitating tumor lysis syndrome in a subset of patients who experience splenomegaly secondary to a malignancy.25,26
Limitations of this review include the small group of operators, including 1 pediatric interventional radiologist and 2 surgeons performing all embolizations and surgical procedures, respectively, within one hospital. The sample size is small and the experience is still early; thus, further prospective review of additional patients to further support our initial findings is needed. Finally, the need for morselization limits the ability to compare splenic size. Future research could provide a formula for in-vivo splenic weight in humans given known weight after morselization.
Conclusion
Massive splenomegaly is no longer a contraindication to minimally invasive splenectomy. Preoperative SAE immediately before splenectomy is safe, feasible, and potentially beneficial in pediatric patients with massive splenomegaly. Utilization of preoperative SAE resulted in completion of 2 cases robotically and 1 laparoscopically that, although we cannot know for sure, may not have been possible without SAE. Although morselization limits splenic size comparisons, the spleen removed en bloc was found to have a 14% decrease in size, suggesting a clear size reduction after arterial embolization. Thus, early results combining preoperative SAE with immediate laparoscopic or robotic surgery are promising for the ability to decrease conversion rates and merit further study.
Footnotes
Acknowledgment
The authors acknowledge Diane Studzinski for her assistance with this project.
Authors' Contributions
Z.R.: Investigation, Writing-Original Draft, Writing-Review and Editing.
R.R.: Investigation, Writing-Original Draft.
A.A.-H.: Investigation, Writing-Review and Editing.
M.L.: Investigation, Writing-Review and Editing.
N.N.: Investigation, Writing-Review and Editing.
P.B.: Investigation, Writing-Review and Editing.
T.M.: Investigation, Writing-Review and Editing.
B.A.: Investigation, Writing-Review and Editing, Visualization.
A.S.: Investigation, Writing-Review and Editing, Visualization.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.