
Abstract
Background:
Laparoscopic isolated caudate lobectomy is still a challenging procedure for hepatobiliary surgeons because of its deep location and narrow operating space. Hilar exposure and adequate operation space play an important role during laparoscopic caudate lobectomy. Very few references are available on this technique, and in this study, we present a new suspension technique to assist laparoscopic caudate lobectomy.
Materials and Methods:
The data of patients with caudate hepatic tumors who underwent laparoscopic isolated caudate lobectomy with or without the double suspension technique at the Eastern Hepatobiliary Surgery Hospital were retrospectively analyzed.
Results:
A total of 25 patients underwent laparoscopic isolated caudate lobectomy at Eastern Hepatobiliary Surgery Hospital between June 2016 and March 2022. Eight patients had perioperative complications, and no patient died within 30 days after surgery. There were no significant differences between the two groups in terms of conversion rate (8.3% versus 7.7%; P = .954), complication rate (25.0% versus 38.5%; P = .480), length of stay (8.0 [6.0–11.0] days versus 9.0 [6.0–19.0] days; P = .098), and postoperative liver function changes. Patients who underwent resection in the suspension group had shorter operation time (154.9 ± 44.3 minutes versus 224 ± 86.3 minutes; P = .018), inferior vena cava dissection time (30.1 ± 5.4 minutes versus 44.8 ± 7.4 minutes; P < .001), and less bleeding (125.0 [20–800.0] mL versus 350 [80–850.0] mL, P = .011).
Conclusions:
This double suspension technique is a safe and feasible method to assist laparoscopic caudate lobectomy. It provides clear exposure and adequate surgical space, thereby shortening the operation time and reducing intraoperative blood loss.
Introduction
In the past decade, improvements in minimal techniques have had a significant impact on the surgical procedure. With the accumulation of surgical experience and the development of laparoscopic instruments, laparoscopic liver resection has been widely used for hepatectomy.1,2 Laparoscopy is not only performed for such sites as the anterior liver lobe but also gradually for the caudate lobe and other complex liver segments. 3 Even so, laparoscopic caudate lobectomy remains a huge challenge for most surgeons, even experienced hepatobiliary surgeons.4,5 At present, there is much literature on laparoscopic caudate lobectomy, but few references on technique that instructs surgeons on how to perform it.6–9
Isolated laparoscopic resection is surgically difficult because of its deep location and adjacency to the hepatic hilar region, the hepatic vein, and the inferior vena cava (IVC). 9 Many of these cases were often performed in combination with right or left hepatectomy for better exposure. 10 For hepatic malignancies, most of these patients have hepatitis or cirrhosis. Therefore, isolated lobectomy is necessary to provide the possibility of radical resection while preserving functional liver parenchyma. 5 But isolated caudate lobectomy is technically very difficult compared with combined resection for its limitation of surgical view and operation space. Therefore, obtaining a clear view and sufficient surgical space plays an important role in the success of isolated caudate lobectomy.
Liver suspension is widely used in laparoscopic gastric and bariatric surgery because it provides adequate surgical field and a proper view.11–14 In terms of technique, there are some references focusing on the approach for laparoscopic caudate lobectomy,15–17 but there is little literature on liver suspension for laparoscopic lobectomy.18–20 In our study, we propose a new suspension technique to help obtain a better view field and a wider surgical area in laparoscopic hepatic caudate lobectomy. The aim of this study was to introduce the technical details and compare the intraoperative and postoperative parameters of laparoscopic hepatic caudate lobectomy with or without the new suspension technique and to evaluate its safety and feasibility.
Materials and Methods
Patients
We retrospectively analyzed 25 patients who underwent laparoscopic isolated hepatic caudate lobectomy from June 2016 to March 2022. Data were collected from a prospective database. All patients were divided into two groups according to whether the suspension technique was performed. Twelve patients (48%) underwent laparoscopic resection with this new suspension technique and 13 (52%) without this technique. Among the 25 cases, 22 (88.00%) were diagnosed with malignant tumor (20 hepatocellular carcinoma and 2 metastatic carcinoma), and 3 (12.00%) were focal nodular hyperplasia. The preoperative liver function of 22 patients was classified as Child–Pugh A class, and 3 was classified as Child–Pugh B7. Routine preoperative investigations included imaging and serology. Three-dimensional imaging was performed according to the doctor's discretion. The study protocol was approved by Eastern Hepatobiliary Surgery Hospital of Shanghai. Each patient signed the informed consent.
Operative technique
Under general anesthesia, the patients were placed in the supine position (inclined 30° to the left). A pneumoperitoneum was created through the subumbilical port with a pressure of 12 mmHg. The positions of the additional four ports are shown in Figure 1 (T1–T5). The trocar and laparoscope were inserted. Pringle's maneuver was routinely used with a clamp/unclamp cycle of 15–20minutes/5 minutes.
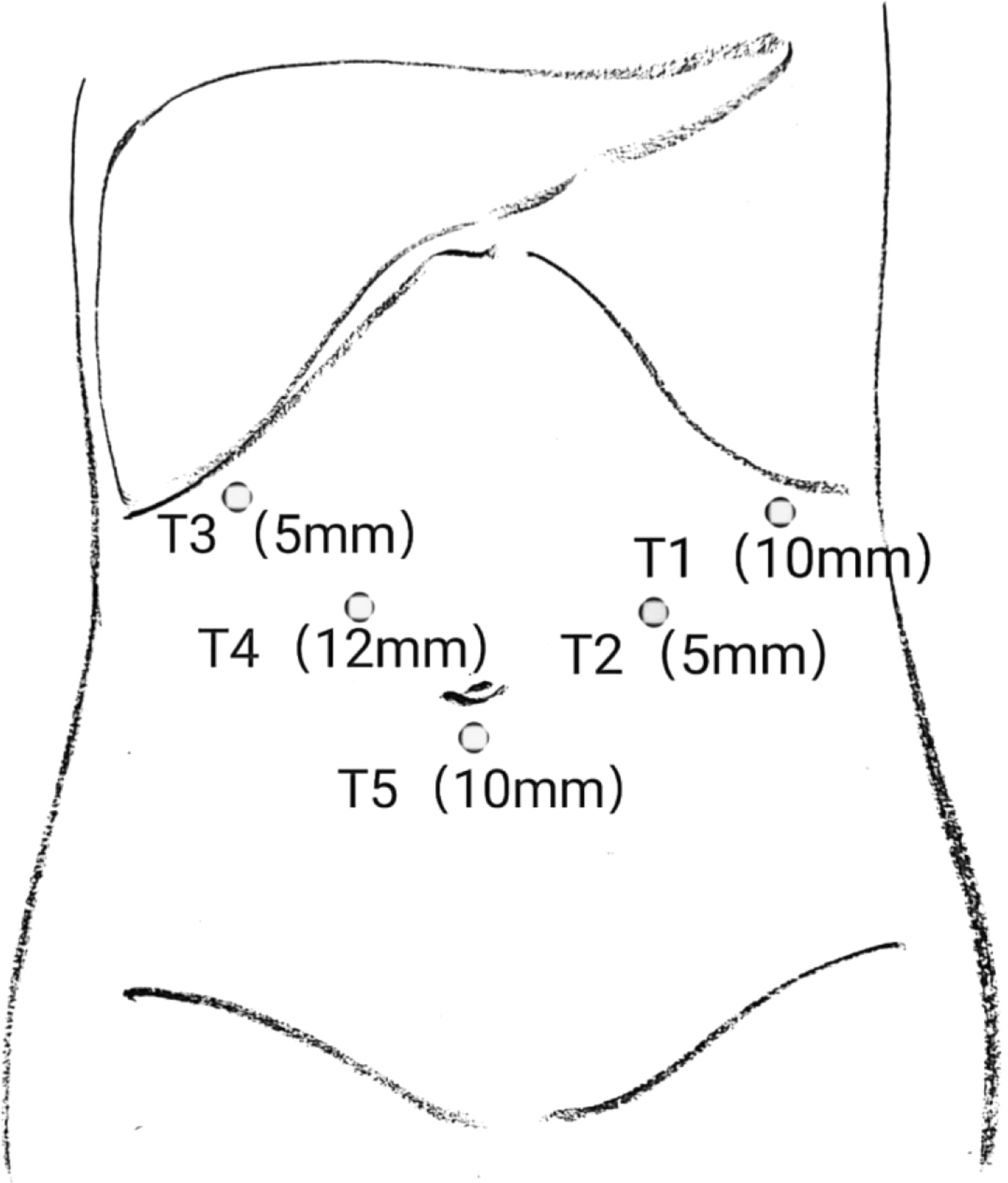
Position of trocar placement.
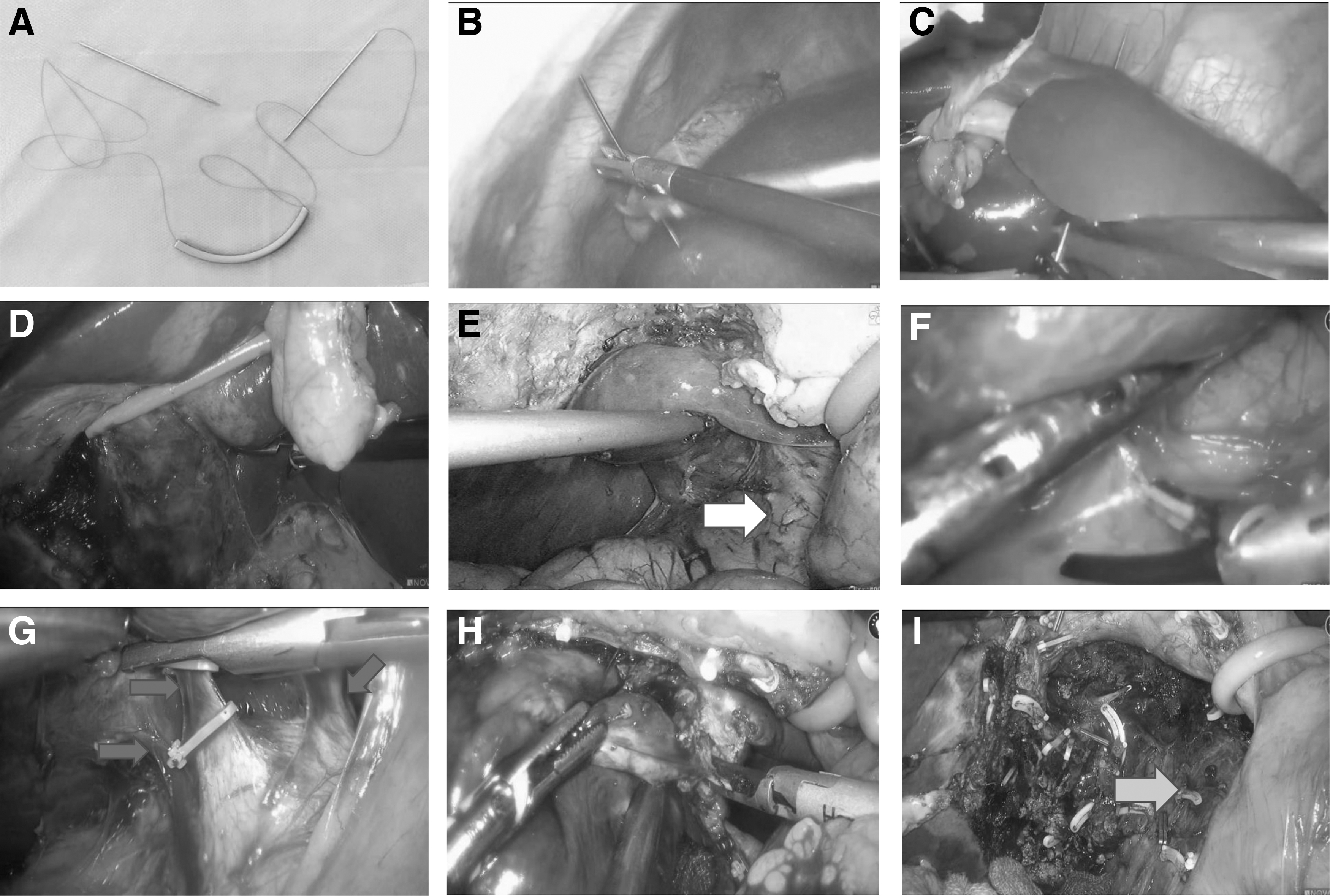
This double suspension technique consisted of two steps: the anterior liver lobes suspension and the hepatoduodenal ligament suspension (Fig. 2A–C). A novel 2-0 modified purse-string suture (W8400 Prolene from Ethicon, Johnson & Johnson Ltd., USA), which is one line with two long straight needles, ran through a rubber hose (Fig. 3A). First, one needle was inserted into the right anterior lobe (segment Ⅴ) and was brought out of the abdominal cavity percutaneously from the subxiphoid area, and the other needle was inserted into left lateral lobe (segment Ⅲ) and was brought out of the abdominal cavity percutaneously from the left subcostal area (Fig. 3B, C); the distance between two needles depends on the location of the tumor. The anterior lobes of the liver could be raised by the suspension when both ends of the suture were pulled outward, and the hepatic hilum was completely exposed (Figs. 2B and 3D). Second, we suspended the hepatoduodenal ligament according to the location of tumor by pulling the Pringle maneuver loop.
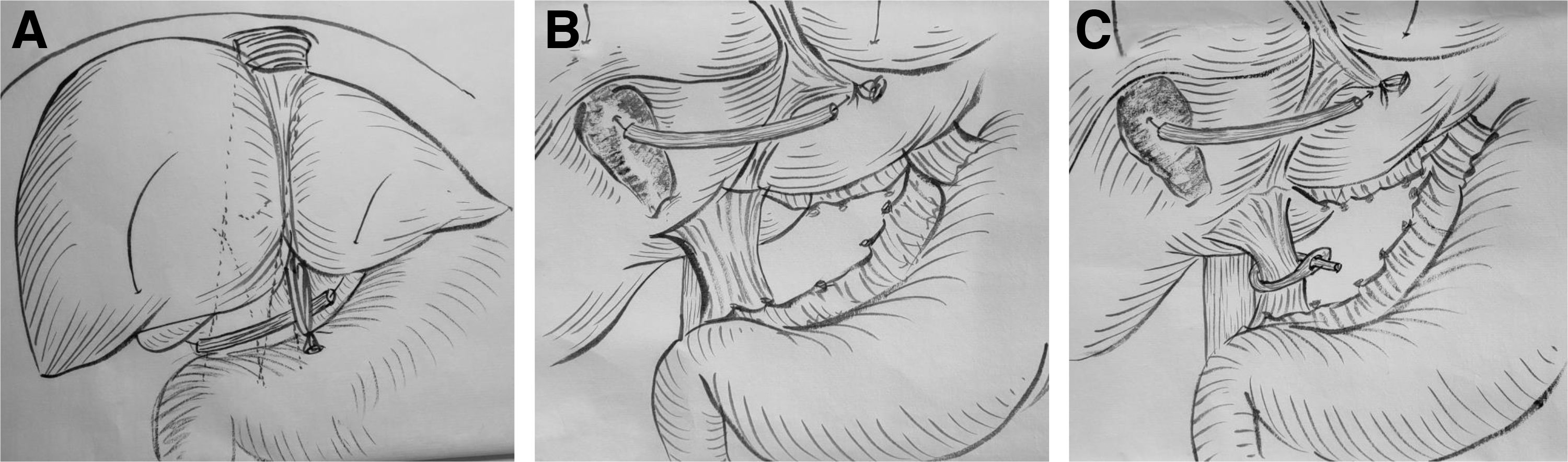
Procedure details of a double suspension technique.
Procedure of a double suspension technique for laparoscopic caudate lobectomy.
We would pull the hepatoduodenal ligament up to the right if the tumor was located in the left Spiegel lobe, to the left if in the process portion, and lift it up to if in the paracaval portion. This procedure provided better exposure of the IVC (Figs. 2C and 3E). Retroperitoneum covering the infrahepatic IVC and hepatocaval ligament (Makuuchi's fascia) was incised (Fig. 3F). The short hepatic veins were dissected from caudal to cranial until the confluence of the right hepatic vein and the IVC (Fig. 3G). After complete separation of the caudate lobe from the IVC, we transected the liver parenchyma at the right border of the caudate process (Fig. 3H). The caudate lobe was then removed, and the retrohepatic IVC was fully exposed (Fig. 3I). The resection area would be carefully examined for biliary leakage and bleeding. The specimen was extracted through the infraumbilical port site.
Statistical analysis
The continuous variables did not comply with the normal distribution and are expressed as median (range). The continuous variables comply with normal distribution and are expressed as mean ± standard deviation. Discontinuous and categorical variables are expressed as numbers. Statistical analysis was performed using SPSS version 22.0. Student's t-test or the Mann–Whitney U test was used for comparison of continuous variables, and χ 2 test or Fisher's exact test was used for comparison of categorical variables. P < .05 was considered statistically significant.
Results
A total of 25 patients underwent laparoscopic complete caudate lobectomy at Eastern Hepatobiliary Surgery Hospital between June 2016 and March 2022. Of the 25 patients, 12 (48%) underwent laparoscopic resection with this new suspension technique and 13 (52%) did not. The clinical and pathological characteristics of the patients in both groups are summarized in Table 1. There were no significant differences in the preoperative data between the group with suspension and the group without suspension.
Clinical Characteristics of the Patients
Age, BMI, Hb, ALB, PT, and comply with normal distribution and are expressed as mean ± SD. PLT, ALT, and AST did not comply with the normal distribution and are expressed as median (range).
ALB, albumin; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; Hb, hemoglobin; PLT, platelet count; PT, prothrombin time; SD, standard deviation; TBIL, total bilirubin; WBC, white blood cell count.
Eight patients had perioperative complications, which was including pneumonia, bile leakage, infection of the surgical incision, and no perioperative death. In the present study, 2 patients required open conversion due to intraoperative bleeding. The intraoperative and postoperative parameters are shown in Table 2. There were no significant differences between the two groups in terms of conversion rate (8.3% versus 7.7%; P = .954), complication rate (25.0% versus 38.5%; P = .480), length of stay (8.0 [6.0–11.0] days versus 9.0 [6.0–19.0] days; P = .098), and postoperative liver function changes. Patients who underwent resection in the suspension group had shorter operation time (154.9 ± 44.3 minutes versus 224 ± 86.3 minutes; P = .018), IVC dissection time (30.1 ± 5.4 minutes versus 44.8 ± 7.4 minutes; P < .001), and less blood (125.0 [20–800.0] mL versus 350 [80–850.0] mL; P = .011).
Intraoperative and Postoperative Outcomes of the Patients
Operative time, IVC dissection time, suspension time, TBIL, and ALB are expressed as mean ± SD. Blood loss, length of stay, ALT, and AST are expressed as median (range).
ALB, albumin; ALT, alanine aminotransferase; AST, aspartate aminotransferase; IVC inferior vena cava; SD, standard deviation; TBIL, total bilirubin.
Discussion
During the past decade, laparoscopic caudate lobectomy has been gradually performed due to the improvement of new surgical equipment and increased experience in laparoscopic resection. 21 Even so, it is still considered a technical challenge for most hepatobiliary surgeons. The procedure is difficult because of its location deep in the hepatic parenchyma and adjacency to the portal vein, hepatic vein, and the IVC. 22 Therefore, it is very important for surgeons to perform laparoscopic caudate lobectomy successfully with better hilum exposure and wider surgical space. Transabdominal suspension sutures are wildly used in various laparoscopic abdominal surgeries. This technique provides a better exposure and adequate operation area for the surgeon at different stages of the operation. This procedure avoids the need to add more ports and instruments, which may reduce the interference with the surgeon's movements.10–13,18
Chai et al performed the Arantius ligament suspension technique during laparoscopic isolated caudate lobectomy to obtain a safe and rapid left lateral lobe retraction. 18 However, this suspension technique is only suitable for patients with tumors located in the left Spiegel lobe. According to the Kumon classification, the caudate lobe is anatomically divided into three portions: the Spiegel's lobe, the process portion, and the paracaval portion.15,23 There are four approaches to caudate lobectomy, including left, right, left–right coordinated, and anterior through hepatic parenchymal dissection depending on the location of the tumor, its characteristics, and the type of caudate lobectomy.4,24 This Arantius ligament suspension technique is only suitable for the left side approach. Here, we perform a new suspension technique that simultaneously suspends the anterior liver lobe and hepatoduodenal ligament and is appropriate for laparoscopic isolated caudate lobectomy by various approaches.
The anterior lobe of the liver, which includes segments III, IV, and V, overlies the hepatic hilum. We suspend the anterior hepatic lobe to achieve good exposure of the Glissonean pedicle. In this way, it is easier to control the inflow of blood supply from the hepatic artery and portal vein into the caudate lobe. After ligation of the portal vein and hepatic artery, transection of the liver parenchyma becomes relatively simple with the caudate ischemia.
The caudate tumors are usually located posterior to the portal vein and anterior to the IVC, where the space is cramped and the surgeon's view is poor. The dissection of the short hepatic veins and separation of IVC are very difficult during the laparoscopic caudate lobectomy, and improper procedure may lead to massive bleeding and gas embolism. Anterior lobe suspension alone does not provide satisfactory exposure of surgical area, mainly because the hepatoduodenal ligament remains in front of the IVC. In this study, we suspended the anterior lobes as well as the hepatoduodenal ligament, and this technique provided better exposure of the IVC and a more adequate operating field. Then, the short hepatic veins were safely dissected and divided under direct vision. After the portal pedicles are dissected and divided, the liver parenchyma division will become easy.
Twenty-five patients underwent laparoscopic caudate lobectomy in this study, and all of them were divided nonrandomly into two groups. The short-term intraoperative and postoperative results of both groups were also compared and analyzed. Our results showed that the surgically suspended group had shorter IVC dissection time, shorter operation time, and less blood loss than the nonsuspended group. There was no significant difference in intraoperative bleeding, postoperative biliary leakage, postoperative liver function impairment, or other complications. We speculate that the shorter dissection time of IVC, shorter operation time, and less blood loss may be related to the exposure of the hepatic hilum and IVC.
On the one hand, this suspension technique provides sufficient operation space, and on the other hand, the ports saved by suspension can be used to place more instruments for hemostasis. The suspension technique did not increase postoperative biliary leakage, liver function damage, or other complications. Therefore, we believe that this new suspension technique may be suitable for laparoscopic caudate lobectomy.
The present study has several limitations. First, the sample size is small and remains insufficient to draw firm conclusion about the surgical choice of laparoscopic caudate lobectomy. Second, this is a nonrandomized retrospective study with its inherent selection bias. Further prospective studies need to be designed and conducted. Finally, this study is a single analysis, and there may be heterogeneity in center experience, surgical procedures, and perioperative management across hospitals. A multicenter cohort analysis is needed.
Conclusions
This new suspension technique is a safe and feasible method to assist in laparoscopic caudate lobectomy. It can provide clear exposure and an adequate surgical space, thereby shortening operation time and reducing intraoperative blood loss.
Footnotes
Authors' Contributions
L.G. contributed to data curation, writing—original draft (equal), formal analysis. X.-Y.Z. contributed to data curation and investigation and writing—review and editing (equal). X.-B.W. contributed to visualization. J.X., J.-X.S., and J.S. contributed to investigation and resources. S.-Q.C. contributed to supervision and conceptualization. W.-X.G. contributed to conceptualization, methodology and supervision, and writing—original draft (supporting) and writing—review and editing (equal).
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Meng Chao Talent Training Program (No: EHBH2019YC112); the Natural Science Foundation of China (No: 82172846); the Shanghai Science and Technology Innovation Action Plan (No: 19411967200). All of them were nonrestricted educational grants.