
Abstract
Introduction:
Morgagni hernia (MH) is a rare congenital disorder, especially in adults, accounting for 2%–4% of all congenital diaphragmatic hernias.
Materials and Methods:
Retrospective review of all patients who underwent surgical repair of MH at our center from 1991 to 2022. A descriptive analysis was performed.
Results:
Eighteen patients presented with MH, of whom 11 (61.11%) were female, with a median age of 67.60 (IQR 50.25–84.50) years old. Six (33.33%) were asymptomatic and 12 (66.67%) presented with symptoms, being dyspnea (4; 33.33%) the most common. On the group of symptomatic patients, the computed tomography scan (8; 66.67%) was the most frequent diagnostic test. Whereas in the asymptomatic group, 5 patients (83.33%) were diagnosed intraoperatively, during surgery for other reasons. MH was mostly located on the right (16; 88.89%). Hernia contents included omentum and colon (10; 55.56%), omentum (5; 27.78%), and stomach (3; 16.67%). All patients underwent surgical repair, needing in 3 cases (16.67%) emergency surgery. Surgical approaches included 10 laparoscopies (55.56%), 7 laparotomies (38.89%), and 1 thoracotomy (5.55%). Repair was generally performed whether by primary closure in 8 patients (44.4%) or by mesh implantation in 10 (55.56%). The median hospital stay was 6 days (IQR 3–10). Three patients presented complications (17.65%): urinary tract infection (1 patient), intra-abdominal collection (1 patient), and the last 1 presented with renal failure and pneumonia. The median follow-up was 74 months (IQR 4.5–130). No recurrence was described.
Conclusions:
MH is a rare condition in the adult population. In our series most patients presented with symptoms. The gold standard treatment is surgical repair, being the laparoscopic approach the most frequent. The complications rate was relatively low and no recurrence was described in our study.
Morgagni hernia (MH) is a rare congenital disorder, especially in adults, accounting for 2%–4% of all congenital diaphragmatic hernias. 1 MH is defined as the presence of a congenital defect in the anterior aspect of the diaphragm between the costal and sternal portions of this muscle. 2 MH is often identified incidentally on cross-sectional imaging in adulthood, with patients presenting with a variety of nonspecific respiratory and gastrointestinal symptoms. 3 The herniation of abdominal contents possesses risk of strangulation. Thus, surgery is the preferred treatment at time of diagnosis.1–3 To our knowledge, this is the largest Spanish single-center retrospective review on MH. 4
We performed a retrospective review of all patients who underwent surgical repair of MH at our center from 1991 to 2022. Data including age, sex, symptoms, diagnostic method, hernia sac content, surgical technique, hospital stay, complications, and mortality were recorded. Only a descriptive analysis was performed due to the scarce number of cases. Since the retrospective nature of the study no ethical committee approval was needed.
Eighteen patients presented with MH, of whom 11 (61.11%) were female, with a median age of 67.60 (IQR 50.25–84.50) years old. Six (33.33%) patients were asymptomatic and 12 (66.67%) presented with symptoms (Table 1). Most common symptom was dyspnea (33.33%), followed by bowel obstruction (25%) and reflux (16.67%).
Initial Clinical Manifestations (n = 18)
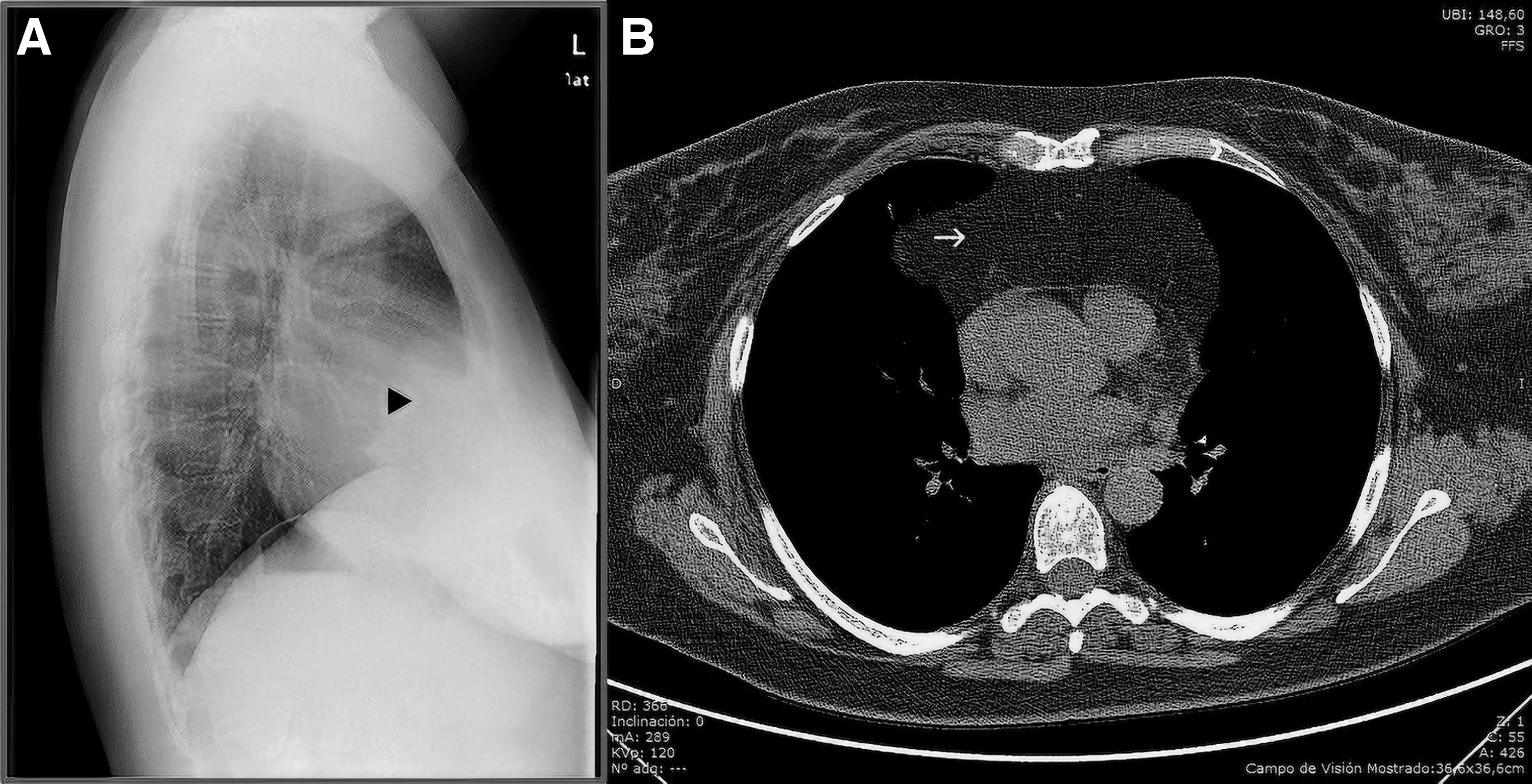
In the group of symptomatic patients, the diagnosis was confirmed by chest X-ray in 4 cases (33.33%) and by computed tomography (CT) scan in 8 (66.67%) (Fig. 1). Whereas in the asymptomatic, 5 (83.33%) were diagnosed intraoperatively, during surgery for other reasons, and 1 (16.67%) on a CT scan performed during the follow-up of a pulmonary nodule. MH was mostly located on the right (16; 88.89%), whereas only in 2 patients it was located on the left (11.11%). Hernia contents included omentum and colon (10; 55.56%), omentum (5; 27.78%), and stomach (3; 16.67%).
All patients underwent surgical repair, needing in 3 cases (16.67%) emergency surgery. Surgical approaches included 10 laparoscopies (55.56%), 7 laparotomies (38.89%), and 1 thoracotomy (5.55%). No thoracoscopic repair was described. Repair was generally performed either by primary closure in 8 patients (44.4%) or by mesh implantation in 10 (55.56%). Of the latter, mesh was used as reinforcement of primary suture in 6 patients (60%) and as an interposition graft in 4 (40%). In all cases hernia sac was excised.
The median hospital stay was 6 days (IQR 3–10). Three patients presented complications (17.65%): urinary tract infection (1 patient), intra-abdominal collection (1 patient), and the last 1 presented with renal failure and pneumonia. The median follow-up was 74 months (IQR 4.5–130). No recurrence was described.
MH is a congenital defect in the anterior aspect of the diaphragm between the costal and sternal portions of this muscle. 2 Conditions associated with increased intra-abdominal pressure, such as pregnancy and obesity, may lead to progressive defect enlargement.2,5 In our population most patients were females, with a median age of 67.60 years, consistent with other studies.1,2,6 Most patients presented with symptoms, with a similar distribution between respiratory and gastrointestinal symptoms. These findings corroborate the existing literature.2,6 Nevertheless, the rate of asymptomatic patients in our populations is far wider than that described by Horton et al. 2
CT scan is the preferred diagnostic modality, helping to precisely diagnose the size, location, and possible complications of the hernia. 7 However, chest X-ray can be also useful.3,5 Most MH were located on the right side, probably because the anterior portion of the left hemidiaphragm is protected by the overlying pericardial sac.5,8 In our case the most common herniated organ was omentum and colon, as it was previously described.1,8 Almost a third of the cases had incarcerated hernias, 2 gastric volvulus, and 1 acute bowel obstruction.
Surgical repair is the gold standard for MH, even in asymptomatic patients, due to the risk of incarceration, as it has been proven by the relatively high percentage of emergent surgeries in our study.3,5 Despite this, the surgical approach of choice is not well established, including primary repair or mesh implantation either through laparotomy, laparoscopy, thoracotomy, or thoracoscopy. 8 Recently, robotic approach has been described, with similar results to laparoscopy. 9 We reported a similar distribution between laparoscopy and laparotomy, with only 1 case of thoracotomy. In our study, in the past 12 years the predominance of laparoscopy is noteworthy, even in emergency cases, with no laparotomies. Young et al. described that regardless of surgical approach the recurrence rate was very low (2.3%), with shorter hospital stay on the laparoscopy group. 8
Excision of the hernia sac remains controversial, with authors stating the risk of injuring thoracic structures. Those supporting sac excision affirm that it decreases the risk on recurrence and seroma.2,3 Regarding hernia repair, primary closure, mesh interposition, or a combination of both has been described, to achieve a tension-free closure.1,10 Mesh was used in 52.93% of the patients in our series, especially on the laparoscopic cases, consistent with current literature.1,7,10 Recurrence rates after MH repair are rather low, but it is only based on retrospective case series, with insufficient long-term follow-up. 7
Main limitations of this study are its retrospective nature and the scarce number of patients. But given the low prevalence of this condition, the difficulty of conducting a prospective study is considerable.
Footnotes
Authors' Contributions
All authors contributed to the study conceptualization. Methodology and formal analysis were performed by Á.S.V. and P.P.J. The first draft of the article was written by Á.S.V., and all authors commented on previous versions of the article. All authors read and reviewed the final article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.