
Abstract
Background:
Swallowable balloons are innovative devices for the treatment of obesity. Endoscopy or anesthesia for implantation is not required. They are generally well tolerated and experience reports satisfactory results in relation to weight loss. The objective of this study was to analyze the first experience with the implementation of a swallowable balloon in Argentina.
Methods:
It is a descriptive retrospective observational study on the treatment of obesity in patients who underwent swallowable balloons in Argentina, admitted to one center, in a period time of 12 months with a follow-up of 6 months.
Results:
A total of n = 153 patients were recruited between June 2021 and May 2022, 78% were women and 22% men. The average age was 39 years. Average body mass index was 29.5 kg/m2. Balloon implantation was performed with complete swallowing by the patients in 19.4% of the cases, swallowing with operator assistance in 55.5%, and swallowing with stylet assistance in 25%. The adverse effects reported were abdominal pain (80%), nausea (60%), vomiting (38%), headache (36%), gastroesophageal reflux (29%), constipation (11%), and diarrhea (7%). No deaths were reported. A mean 4-month weight loss of 12% was reported.
Conclusion:
Swallowable balloon for the treatment of obesity is effective, safe, and well tolerated. Adverse effects are not severe.
Introduction
Morbid obesity and overweight are a multifactorial disease.1,2 Treatment requires a multidisciplinary team that includes surgery. The advent of laparoscopic procedures has favored bariatric surgery. It allows good access to the abdominal cavity, produces less bleeding and pain, and favors postoperative recovery.3,4 But despite these advantages, many obese patients do not want to undergo a surgical procedure. For this reason, alternative techniques have been developed. One of them is the use of an intragastric balloon, indicated starting with a body mass index (BMI) of 27 kg/m2 or patients who are not candidates for bariatric surgery for weight loss.
In recent years, several kinds of balloons have been used.5,6 Endoscopy is required for both implantation and removal, which could be associated with some complications. But the evolution of technology applied to medicine has made it possible to develop swallowable balloons. These new balloons do not require endoscopy and anesthesia for handling, since they are controlled under fluoroscopy. 7
In this article we present an initial experience in the use of swallowable balloons.
Objectives
The objective of this study was to analyze the first experience with the implementation of a swallowable balloon for the treatment of obesity in Argentina.
Materials and Methods
This is the first descriptive retrospective observational study on the treatment of obesity in patients who underwent swallowable balloon in Argentina. The data collected were from patients admitted to one center (Diagnomed, Buenos Aires, Argentina), who were treated by the same medical-surgical team. The time period analyzed was 12 months (from January 2021 to January 2022). The following selection criteria were considered: (1) inclusion criteria: age between 18 and 64 years, BMI between 27 and 45 kg/m2, residence close to the institution and (2) exclusion criteria: organ failure (heart, liver, kidney), anticoagulation/antiaggregation, cancer, hiatal hernia, and pregnancy/lactation. The follow-up period was 6 months.
Swallowable intragastric balloon
The swallowable balloon (Elipse™ System; Allurion Technologies, Natick, MA, USA) is made of a flexible material that allows it to be swallowed without inconvenience or great discomfort (Fig. 1). The balloon is connected to a catheter 75 cm long and 1.3 mm in diameter. This catheter features radiopaque markings to improve fluoroscopic control during balloon swallowing. Once inside the stomach, it is filled with a special solution of distilled water and potassium. Its volume is 550 cm3. After placement, the nutritional monitoring app is activated on the smart scale and the smart watch health tracker (Fig. 1). The balloon has a valve that, after 16 weeks, dissolves automatically, allowing the liquid to escape and emptying the balloon. It is eliminated naturally.
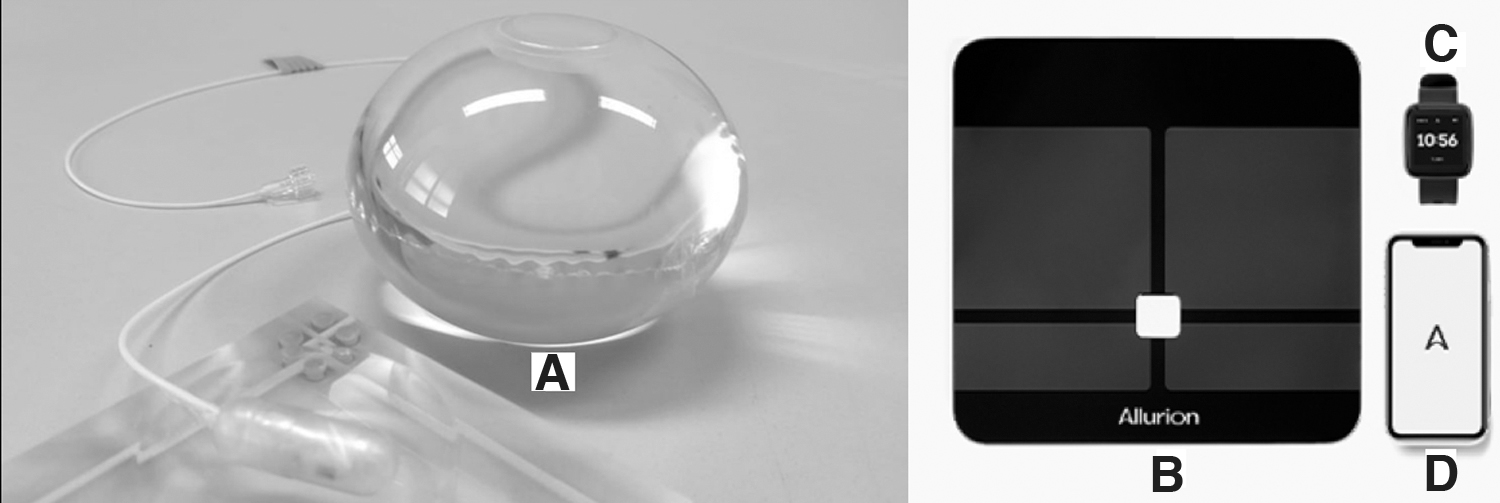
Elipse™ System swallowable gastric balloon. It is composed of the gastric balloon
Technical aspects
All balloons were placed in a room specially prepared for these procedures. The patients were explained of the intervention who then signed the informed consent.
Swallowable balloons connected to a catheter were placed deflated in the mouth. The patients swallowed it with the help of water and/or sparkling water. The position of the balloon in the stomach was verified with the help of the catheter marking. The correct situation was corroborated with fluoroscopy (Fig. 2A). The balloon was then connected to the pumping system and inflated with the corresponding solution (Fig. 3). Once the insufflation was completed, a new fluoroscopy was performed to verify the correct inflation of the balloon (Fig. 2B). Finally, the introduced catheter was removed and the nutritional monitoring app was connected. Patients were discharged the same day with indication of taking antiemetics and antispasmodics for 3 days, and gastric protector (proton pump inhibitor [PPI]) for 4 months as medication.

Fluoroscopy control after swallowing gastric balloon placement.

Pumping system for balloon insufflation.
Follow-up was carried out at 7 days to assess tolerance to the procedure, then every 15 days by the nutrition assistant team.
Statistical analysis
Statistical data were analyzed using computer programs (IBM SPSS Statistics 25.0). Results are expressed in percentage, range, and standard deviation. A 95% confidence interval was applied, and a value of P < .05 was established as statistically significant.
Bioethical aspects
All participants signed an informed consent.
Results
A total of n = 153 patients were recruited. Demographic data were analyzed (Table 1). In total, 119 (78%) were women and 34 (22%) were men (±0.41). The mean age was 39 years (range 21–72, ±20.01). The average BMI was 29.5 kg/m2 (range 27–43, ±3.17). The associated morbidities were high blood pressure 68%, dyslipidemia 56%, and diabetes or insulin resistance 54%.
Demographic Data
F, female; M, male; BMI, body mass index; DLP, dyslipidemia; DM, diabetes mellitus; HBP, high blood pressure.
The time required for the procedure was 21 minutes (range 14–37 minutes, ±7.02). The introduction of the balloon was performed with complete swallowing by the patients in 19.4% (30 ± 0.40) of the cases, swallowing with the operator's fingers in 55.5% (85 ± 0.50), and swallowing with the assistance of stylet by 25% (38 ± 0.43).
The adverse effects reported were abdominal pain (epigastrium) (122, 80%, ±0.40), nausea (91, 60%, ±0.49), vomiting (58, 38%, ±0.48), headache (55, 36%, ±0.48), gastroesophageal reflux (44, 29%, ±0.45), constipation (16, 11%, ±0.30), and diarrhea (10, 7%, ±0.24) (Table 2). The duration of symptoms was 48 hours on average. In only one case, the balloon had to be removed 20 hours after its placement due to discomfort caused by intolerance. In one case, the balloon had to be removed early due to catheter rupture, which was replaced after 1 week. Balloon repositioning was required due to early balloon deflation (before 3 months) in 3 patients. No deaths were reported.
Details of Implantation of Balloons and Complications
In order of results, mean 4-month weight loss was 12% (6% −25%) and weight loss failure was 10.5%.
Discussion
Bariatric surgery comprises several well-developed surgical techniques with good results. The complication rate is low and variable according to the technique used.8–10 Minimally invasive and image-guided procedures have taken center stage in the treatment of these situations.11–15
The gastric balloon is a good option in those patients who present contraindications for surgery or who fear postoperative complications. Different types have been developed over the years, generally requiring endoscopes and anesthesia/conscious sedation for placement and removal. Although rare, complications have been reported during endoscopic placement and removal of some gastric balloons.16,17 The swallowable balloon makes it possible to avoid such invasive procedures.18,19 Satisfactory results were reported at the end of treatment in relation to weight loss when compared with other balloons. 19
Swallowing the balloon is generally easy and well tolerated by the patient. We consider taking of medication to relieve symptoms (antiemetics, antispasmodics, gastric protectants) to be of fundamental importance. When some inconvenience for placement is presented, the operator can help (fingers) or a stylet can be used. Stylet assistance has been reported in 35.9%. 20 In our team, the placement of the balloon with a stylet was lower, close to 25%. This allows the procedure to be less invasive for the patient and more cost-effective, saving the cost of the stylet.
Once the balloon is inflated in the stomach, it is well tolerated by most patients. The symptoms reported were mild and for no more than 48 hours of evolution. In our series, only 1 patient required early removal of the balloon (at 20 hours) due to digestive intolerance and abdominal discomfort. So far, we have not been informed about serious complications associated with this kind of balloon.
Regarding the results, in a 6-month follow-up, an average weight loss of 12% and a good tolerance to the device were reported, data similar to those published in the literature. 7 Weight loss was notable and marked in the first weeks, after which a slowdown in weight loss was observed, although it remained constant until the last days. No weight regain was observed in this short period of time. The failure rate of the method was 10.5%, considering as such the situation of not exceeding 10% weight loss in a period of 4 months. As an additional objective, the change in lifestyle was well achieved in the majority of patients. The impact on the improvement of comorbidity parameters has not yet been analyzed by this group.
The limitations of this study are the low number of individuals who make up the series and the short follow-up. Randomized clinical trials with long-term follow-up are required to determine the true scope of this novel device, although preliminary results are promising. 21
Conclusion
The implementation of the swallowable balloon for the treatment of obesity has demonstrated its effectiveness, safety, and good tolerance. However, comparative and randomized clinical studies are needed to determine its long-term efficacy.
Informed Consents
All patients signed an informed consent to participate in research and to allow us to use their data for publication.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.