
Abstract
This review describes the evolution of hiatal hernia repair for the past several decades: From the use of a primary tissue repair only, the subsequent inclusion of synthetic mesh and its complications, to current day indications for mesh use. We will highlight the recent research in biologic and composite meshes as well as the ongoing limitations in studying their efficacy. Finally, we will describe our institutional indications and surgical technique practices in the utilization of biologic mesh.
Introduction
Hiatal hernias were first reported in the literature in 1853 by Bowditch, with the first open repair described by Soresi in 1919. 1 Several repair techniques by Nissen, Belsey, and Collis were developed as surgeons attempted to improve upon primary closure of the hiatus. Despite these and many other advances in approaches to hiatal hernia repair, elevated recurrence rates were still noted, reportedly ranging from 12% to 66%.2–5 As a result, surgeons soon began to explore the use of mesh reinforcement in hiatal hernia repair. Since the introduction of mesh in the late 1990s, surgeons have attempted to optimize or criticize the role of mesh in hiatal hernia repair. In this article, we will review the existing literature and explore the nuances surrounding the use of mesh in cruroplasty.
Success with Synthetic Mesh
Early on, many studies found a decrease in hiatal hernia recurrence rates with the use of synthetic mesh. In 1999, Frantzides et al published a prospective randomized study of 35 patients that showed significantly lower recurrence rates with polytetrafluoroethylene (PTFE) mesh use at 3 years. 6 In 2002, Granderath et al performed a prospective study evaluating outcomes of patients with only primary crural sutures to polypropylene mesh reinforcement and notably found a recurrence rate of 6.1% compared with 0.6% when reinforced with mesh. 7 A randomized double-blinded clinical trial conducted by Analatos et al described 159 patients who were allocated to closure with crural sutures or PTFE mesh. 8 There were no significant differences in recurrence at 12 months and 3-year follow-up; however, there was significantly more dysphagia to solid food in the mesh closure group. These and other researchers found early success with synthetic mesh, which led many other surgeons to incorporate synthetic mesh into their practice.
Complications of Synthetic Mesh
These encouraging results in recurrence rate reduction were soon followed by complications related to synthetic mesh use. Numerous case reports and case series described unacceptable morbidities such as transmural gastric migration, esophageal erosion, esophageal stenosis, and mesh rejection.9–14 These complications, although rare, are serious. Consequently, there has been a move toward the use of biologic absorbable or composite mesh 15 to decrease the morbidity of synthetic mesh and maintain a reduction in recurrence rate.
Biologic Mesh and Emergence of Composite Mesh
With the unacceptable postoperative complications associated with synthetic mesh well described in the literature, surgeons began to explore biologic or absorbable meshes as alternatives. Absorbable meshes that have been developed include Vicryl® (Ethicon, Somerville, NJ) and Bio-A® (Gore Medical, Newark, DE). Biologic meshes include Surgisis® (Cook Medical, Bloomington, IN), Biodesign Hiatal Hernia Graft® (Cook Medical), AlloDerm® (Allergan PLC, Dublin, Ireland), and Strattice™ (Allergan PLC).
One of the index studies of biologic mesh was published in 2006 by Oelschlager et al. They randomized a cohort of 108 patients to primary repair alone or primary repair buttressed with biologic mesh made from porcine small intestine submucosa (SIS). 16 At 6 months, patients underwent an upper gastrointestinal series and the SIS buttress group had significantly fewer incidences of recurrence without a difference in perioperative complications. However, this patient cohort was followed out to 5 years and there was no longer a significant difference in recurrence between the two groups. 17
A meta-analysis in 2016 that included nine studies was able to compare synthetic mesh with biologic mesh and found that although synthetic mesh had lower recurrence rates than biologic mesh, both were still superior to suture repair. 18 In 2019, Sathasivam et al also found lower recurrence rates with mesh reinforcement including biologic mesh over suture cruroplasty without significant differences in perioperative complications. 19 A systematic review by Antoniou et al 20 was able to describe a trend toward lower recurrence with biologic mesh but could not draw conclusions about the long-term efficacy of biologic mesh due to inconsistent long-term follow-up among the studies.
A systematic review and meta-analysis in 2017, found that mesh, including biologic mesh was associated with lower recurrence rates (2.6% versus 9.4%) and that biologic mesh was associated with high quality of life scores as measured by the SF-36 questionnaire. The authors suggested this could be due to biologic mesh creating less scarring than permanent meshes. 21 A more recent systematic review in 2021 by Rausa et al showed similar results: an overall lower recurrence rate with the use of biologic mesh. The main limitation of this study was that they were unable to compare the specific types of mesh with their respective recurrence rates. 22
In addition to the positive and equivocal findings associated with the use of biologic mesh, there are also several studies that have found no added benefit. In 2017, Tam et al found that mesh cruroplasty in laparoscopic repair of paraesophageal hiatal hernias did not confer lower recurrence rates and had similar outcomes in symptoms such as dysphagia and bloating. 23 In 2020, Watson et al found no improvement in recurrence rate with biologic mesh and found higher rates of bloating, chest pain, and diarrhea. 24 Finally, a more recent systematic review in 2021 found that data were quite heterogeneous revealing no significant differences when comparing primary closure with routine biologic mesh reinforcement. 25
More recently, research has emerged examining the use of composite mesh to retain the benefits of permanent mesh reinforcement with a lower risk of complications. Composite meshes, such as Crurasoft® (C. R. Bard, Inc., Cranston, RI), Parietex™ Composite (Medtronic, Minneapolis, MN), and others are permanent meshes that also have a viscera protective antiadhesion barrier. In 2013, Zhang et al studied the use of Crurasoft in 21 patients and found a recurrence rate of 0% during the 6-month follow-up period, and 4.76% at a mean long-term follow-up period of 16.28 months. 26 New onset dysphagia did occur in 8 patients (38%), but authors did not report any serious associated complications. Another study by Priego et al published in 2017 studied the use of Crurasoft in 536 patients.
They found a low recurrence rate of 9%; however, the overall postoperative complication rate was 28%. This included dysphagia (5%), 1 death attributable to the mesh placement (1%), and an overall 5.4% mortality rate including 2 cases of esophageal perforation and 1 case of gastric perforation. 27 In 2021, Sawyer et al published a retrospective study on a composite mesh, OviTex, and found no recurrence at 14.2 months. 28 A study by Wang et al attempted to compare composite mesh with biologic mesh in a retrospective study of 101 patients, 66 of which were assigned to a mesh group. 29 The biologic meshes used were 4-ply biologic SIS (Surgisis®, November 2010) and 6-ply SIS (Biodesign™ Surgisis®, March 2011). Crurasoft was the composite mesh used.
The recurrence rates at 6 months for all mesh types was 0%. At a median follow-up period of 31 months, the recurrence for 4-ply SIS, 6-ply SIS, and Crurasoft were 30%, 13.6, and 4.5%, respectively, although this difference did not achieve statistical significance. In the subgroup analysis there was a positive trend in Visick scores, which characterize subjective symptoms postgastric surgery. Crurasoft and 6-ply SIS had similar Visick scores, which were higher than the 4-ply SIS. A higher frequency of postoperative dysphagia was presented in the Crurasoft group compared with other two groups at 6 months postoperatively, but the difference was not significant at 31 months (P = .227). Additional long-term studies specific to composite mesh are needed to determine if this category of mesh can be routinely used in hiatal hernia repairs.
Current Uses of Biologic Mesh
With the heterogeneity in data, standard patient selection for biologic mesh reinforcement still remains elusive. Currently, biologic mesh has been described for use in a few select scenarios such as large hiatal hernias (no standard definition but typically <5 cm defect), giant hiatal hernias (no standard definition but described as >30%–50% of stomach herniation), repairs under tension, and in cases of a recurrent hiatal hernia. These indications are not consistently supported in the existing literature. 30 For example, in 2019, Memon et al found that mesh reinforcement including biologic mesh lowered recurrence rates only in large hiatal hernia. 31 However, a systematic review published by Laxague et al evaluating use of biologic mesh in patients with large hiatal hernias, obesity, or recurrent hiatal hernias found that mesh placement conferred benefits in quality of life in patients with a recurrent hiatal hernia, 25 but not in patients with obesity or large hiatal hernias.
How we do it
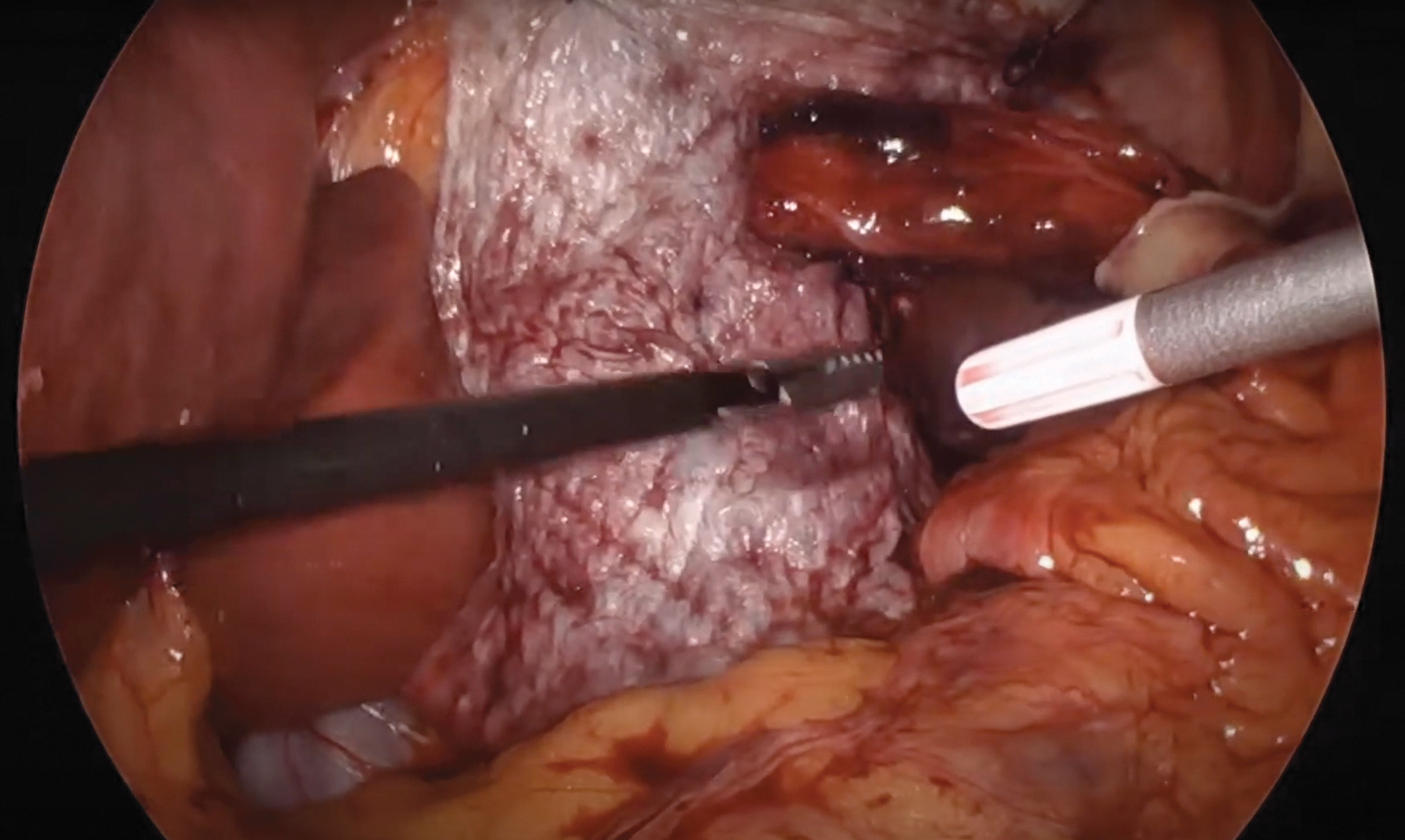
Our practice is to include biologic mesh selectively in hiatal hernia repairs in cases of recurrent hiatal hernias or repairs under tension. We perform a primary suture repair of a hiatus with nonabsorbable sutures and reinforce the repair with a submucosal biologic mesh (Biodesign Hiatal Hernia Graft; Cook Medical). We prefer a C configuration of the mesh during placement as we believe this allows for better coverage of the anterior hiatus. The mesh is secured at each top corner with sutures (Fig. 1). We then lift the mesh to spray TISSEEL fibrin sealant directly on the hiatus and then gently adhere the posterior surface of the mesh to the primary repair (Fig. 2). Once sealed, we spray the sealant on the anterior surface of the mesh as well (Fig. 3).
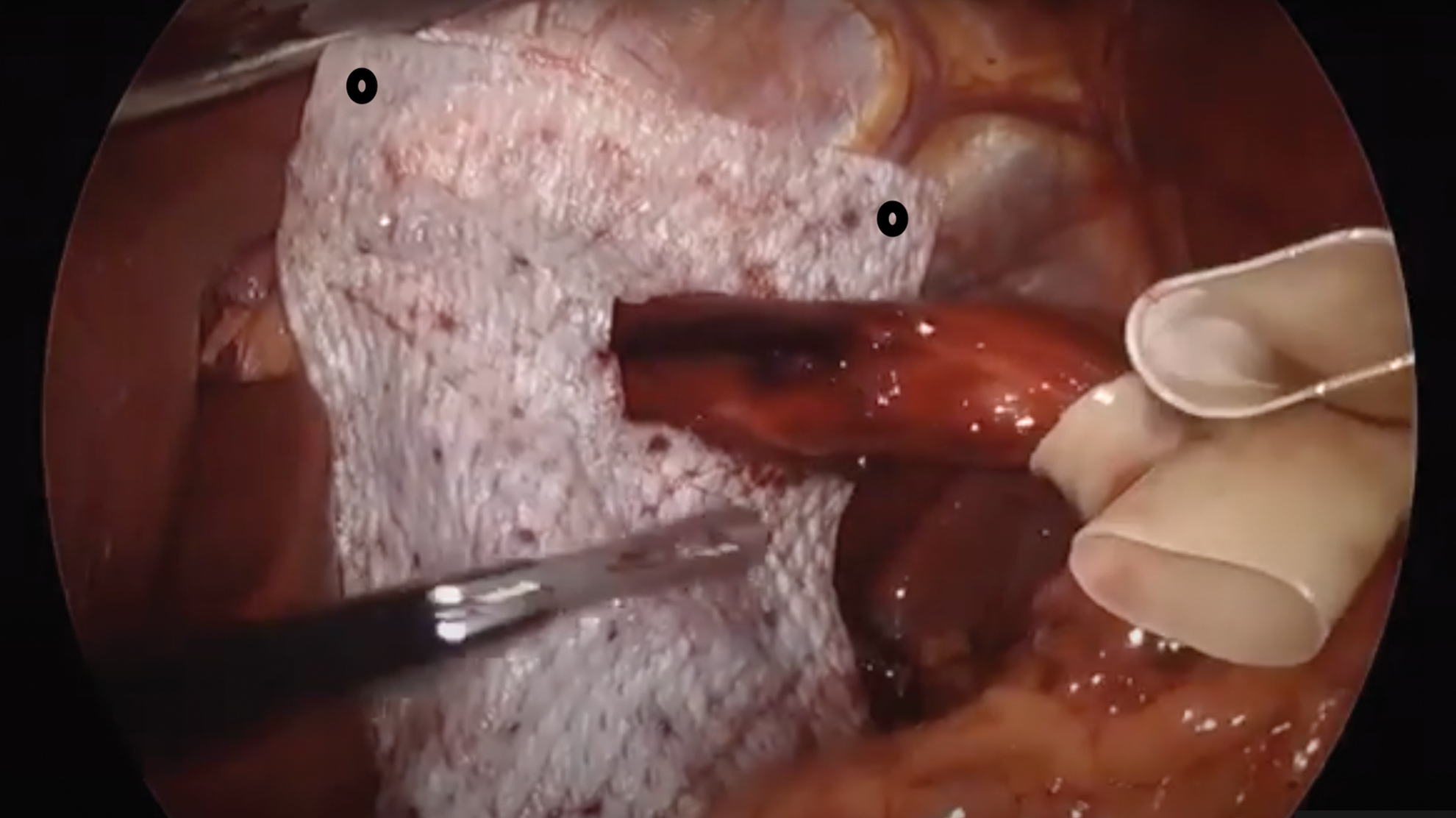
Mesh is placed in a C configuration (A U configuration is also appropriate). Colored dots show where we secure the mesh. Color images are available online.

The mesh is reflected up to administer TISSEEL on the posterior surface against the primary repair. Color images are available online.
As the last step, TISSEEL is placed on the anterior surface of the mesh. Color images are available online.
Conclusion
Synthetic mesh reduces recurrence rates in hiatal hernia repair but should be avoided due to its associated morbidities. Many surgeons use biologic mesh; however, current data are still limited and only suggest a short-term (<5-year) benefit. Biologic or composite mesh may be beneficial in reducing recurrence rates in large hiatal hernias with tension as well as in recurrent hiatal hernias, but this has not yet been shown consistently across studies. More research is needed comparing types of biologic and composite meshes in patients with various risk factors to yield improved consensus and standardization for a reproducible, lasting, and safe hiatal hernia repair.
Footnotes
Authors' Contributions
Both authors contributed to the study conception and design. Material preparation, data collection, and writing the first draft of the article were performed by R.S. Reviewing, editing, and supervision were by H.T.J. Both authors read and approved the final article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.