
Abstract
Background:
Management of acute cholecystitis with emergency laparoscopic cholecystectomy has been established; however, detection and management of concurrent choledocholithiasis are debated. The aim of this study is to develop a more accurate choledocholithiasis predictive model.
Materials and Methods:
A 9-year audit of emergency cholecystectomies and evaluation of preoperative factors in predictive models. Receiver Operating Curve (ROC) analysis/Youdon Index was used to identify thresholds maximizing these associations for continuous variables.
Results:
1601/1828 patients were analyzed. Patients who were diagnosed with choledocholithiasis were more likely to be febrile on admission, have a higher C-reactive Protein, and higher median bilirubin (25.0 μmol/L versus 11.0 μmol/L, P < .001). When excluding bilirubin, multivariate analysis detected several significant variables, including fever, biliary tree dilatation, or a common bile duct stone seen on ultrasound. When bilirubin was included into the model, bilirubin of 20–39 μmol/L (odds ratio [OR] 2.44, 95% confidence interval [CI]: 1.74–3.44) and ≥40 μmol/L (OR 4.84, 95% CI: 3.40–6.91) were shown to have increased likelihood of choledocholithiasis detection on intraoperative cholangiogram, with the ROC model having a significant C-statistic of 0.796 (P < .001).
Discussion:
A perfect predictive model for concurrent choledocholithiasis in acute cholecystitis does not exist; however, the results from this study are encouraging that high and low predictive groups can be established.
Introduction
Gallstone disease is a prevalent condition affecting up to 10%–15% of the adult population. 1 While the large majority are asymptomatic, ∼15% experience symptoms or complications related to gallstone disease, which constitute a broad clinical syndrome ranging from biliary colic to acute gallstone pancreatitis.2,3 However, the most common presentation to the emergency department is acute cholecystitis,4,5 of which the gold standard of treatment is to undergo laparoscopic cholecystectomy. 6 Within this population group, up to 15% of patients may have concurrent choledocholithiasis.7–9 Choledocholithiasis has the potential of causing life-threatening complications, including pancreatitis and cholangitis. 10 The practice of preoperative diagnosis and treatment of choledocholithiasis is varied between surgeons and different institutes.11–13
Various guidelines from organizations, including The National Institute for Health and Care Excellence (NICE) and The European society of Gastrointestinal Endoscopy (ESGE), have made recommendations for the routine use of ultrasound (USS) and liver function tests (LFTs) for the preoperative assessment of choledocholithiasis and suggested that a negative USS and LFT requires no further evaluation while positive findings warrant advanced preoperative imaging. However, these recommendations are based on low to moderate strength evidence in health settings that do not use intraoperative cholangiography as standard practice, and do not provide a definite tool that can be used. 14
Furthermore, additional preoperative investigations such as magnetic resonance cholangiopancreatography (MRCP) are expensive with the cost effectiveness of this being currently queried. 15 The aim of this study is to identity correlating preoperative variables—with a focus on serum bilirubin and abdominal USS—with the risk of choledocholithiasis and hence develop a predictive model that can be used to aid surgeons' clinical decision-making for patients undergoing emergency cholecystectomies.
Materials and Methods
The study was performed as a retrospective audit at The Northern Hospital, Epping, Australia, over a 9-year period (between September 2008 and December 2017). Ethical approval was granted by the Northern Health Office for Research and Governance (ALR 04.2017).
All patients undergoing emergency cholecystectomy were identified from hospital records using operation coding and relevant preoperative, operative, and postoperative data were collected. Complications were recorded according to the Clavien–Dindo classification. 16 Surgical time was recorded routinely by theater staff from the time of anesthetic hand-over to the surgeons to the time dressings were placed. Patients for whom LFTs or intraoperative cholangiogram (IOC) were incomplete or improperly documented were excluded (Fig. 1). The remaining patients were then divided into two groups, those with an IOC result negative for choledocholithiasis, as defined by the operative surgeon noting full visualization of the extrahepatic biliary anatomy with no filling defect and free passage of contrast into the duodenum, and those with a positive IOC indicative of choledocholithiasis, as defined by the operating surgeon identification of a nongas bubble filling defect in the biliary tree.
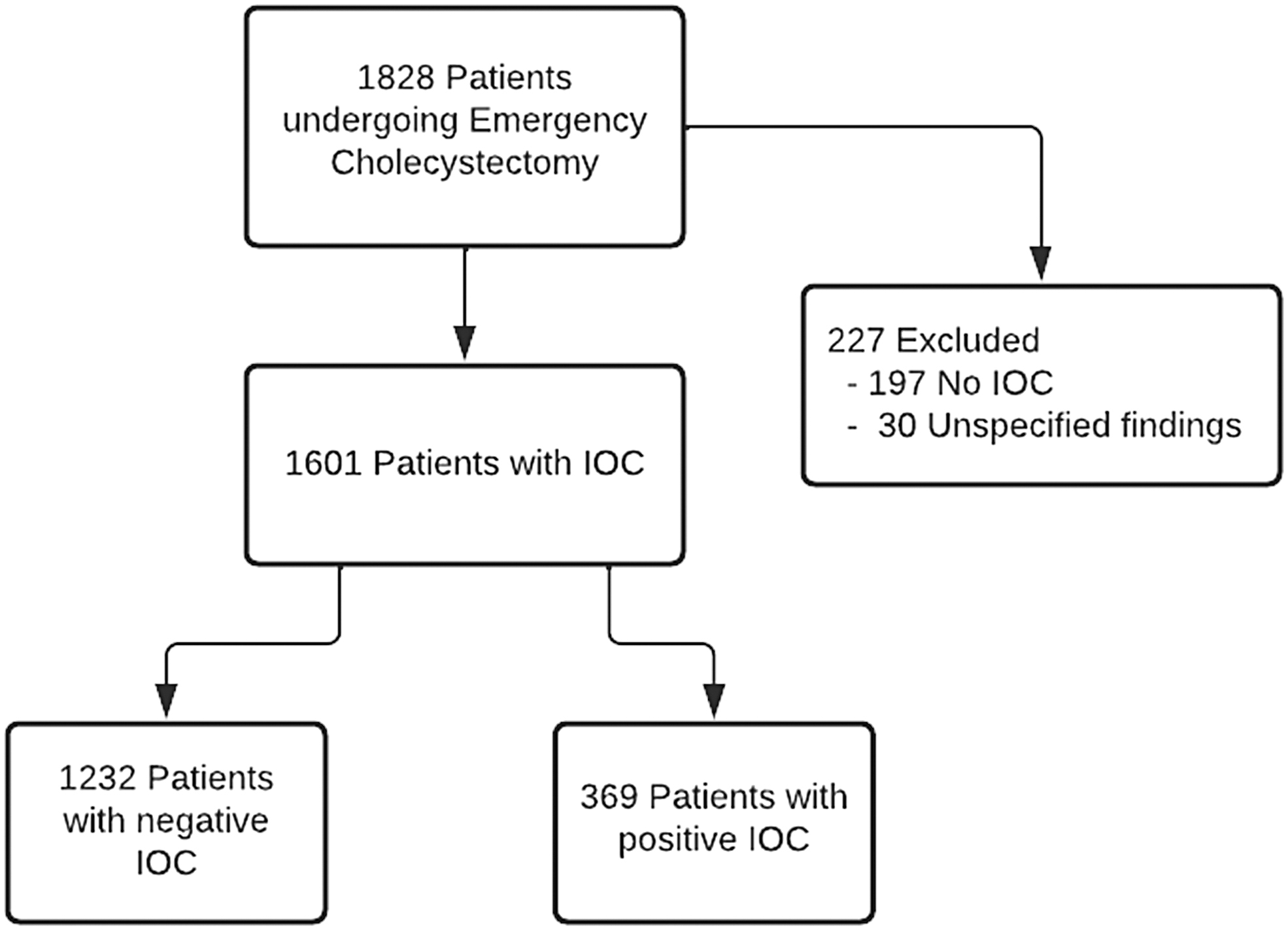
Patient selection and exclusion criteria.
For patients with a preoperative abdominal USS, positive findings of dilatation of the common bile duct (CBD), as reported by the radiologist, and a stone being visualized in the CBD were recorded.
Laparoscopic cholecystectomies were performed with a standard four-port American technique with IOC performed with iohexol (Omnipaque, GE Healthcare, Chicago, IL, USA). Cholangiograms were interpreted intraoperatively by the operating surgeon with further decision on CBD exploration, endoscopic retrograde cholangiopancreatography (ERCP), or conservative management made by the operating surgeon. CBD explorations were performed through a transcystic approach where possible.
Sample size and power considerations
Assuming an approximate rate of positive IOC of 15% and a maximum of 20 variables to be considered in the multivariable model(s), the sample size calculation described in Peduzzi indicated that the required sample size for the analysis was ∼1333 cases. 17
Statistical analysis
Descriptive analysis was conducted to compare patients with positive IOC with negative IOC patients using Stata version 17.0 (Stata Corp, College Station, TX, USA). For continuous variables, normality was determined through Shapiro–Wilk test, with normally distributed variables reported as mean and standard deviation (SD) and differences between groups tested using the Student's t-test. Non-normally distributed variables were reported as median and interquartile range, with Mann–Whitney (rank-sum) test used to test for differences across groups. Univariate analysis was conducted to identify variables associated with positive IOC. Receiver operating curve (ROC) analysis and the Youden Index was used to identify thresholds maximizing these associations for continuous variables. Continuous variables were also assessed by categorizing based on median values to create a dichotomous variable, tertiles, or quintile thresholds.
The standard thresholds of bilirubin of <20 μmol/L (normal), 20–39 μmol/L, and ≥40 μmol/L (greater than twice normal) were considered, and found to provide the best predictive performance for the bilirubin variable. Variables with P < .2 were considered in multivariable logistic regression analysis using backward stepwise regression techniques to identify independent statistically significant variables associated with positive IOC. C-statistics (Area under the ROC), Schwarz’ Bayesian Information Criterion, and the Hosmer–Lemeshow test were used to compare model fit and select the proposed model. Statistical significance was set at a P < .05.
Results
A total of 1828 patients who underwent emergency cholecystectomy were identified during the 9-year period. One hundred ninety-seven patients were excluded from data analysis due to lack of or inadequate documentation of IOC result with 30 cases of unspecified findings, leaving 1601 patients for analysis (Fig. 1). The mean age for the IOC-positive group was slightly higher (49.8 years versus 47.0 years, P = .013), and there was no difference in the proportion of sex (P = .70). Patients who had choledocholithiasis on IOC were more likely to be febrile on presentation (14.4% versus 7.2%, P < .001), have a higher median C-reactive Protein (12.0 mg/L versus 9.7 mg/L, P = .028), and higher median preoperative bilirubin (25.0 μmol/L versus 11.0 μmol/L, P < .001; Table 1).
Patient Demographics and Preoperative Variables and Associations with Intraoperative Cholangiogram Status
ASA, American Society of Anaesthesiologists; CBD, common bile duct; CRP, C-reactive Protein; CT, computed tomography; HPB, hepatopancreaticobiliary; IOC, intraoperative cholangiogram; IQR, interquartile range; LFT, liver function test; MRCP, magnetic resonance cholangiopancreatography; MRI, magnetic resonance imaging; RUQ, right upper quadrant; SD, standard deviation; US, ultrasound; WCC, white cell count.
For the prediction of IOC-positive patients, the assessment of bilirubin alone provides an area-under the curve (C-statistic) of 0.679 (95% CI: 0.652–0.707), when considering the threshold of less than or greater than or equal to 18.5 μmol/L, which was the median value for bilirubin in this dataset. The C-stat increases slightly to 0.694 (95% CI: 0.666–0.723) when using the thresholds of <20, 20–39 and ≥40 μmol/L for bilirubin.
As indicated in Table 2, the multivariable analysis identified six variables that were statistically significant in their association with IOC positive, when not including bilirubin (Model 1). Patients aged <35 years (OR 1.56, 95% CI: 1.12–2.17) and ≥55 years (OR 1.38, 95% CI: 0.99–1.93) were found to have increased likelihood of IOC positivity. Patients with fever (OR 1.80, 95% CI: 1.17–2.78), dilated biliary tree/obstruction (OR 5.29, 95% CI: 3.69–7.56), and CBD stone seen (OR 8.65, 95% CI: 5.05–14.82) were also associated with positive IOC.
Multivariable Analysis Models for Association with Intraoperative Cholangiogram Positive Status
CBD, common bile duct; CI, confidence intervals; CT, computed tomography; OR, odds ratio; US, ultrasound.
As shown in Table 3, the C-statistic increased from 0.747 to 0.793 (P < .001) when bilirubin was included in the model (Model 2), with patients with bilirubin of 20–39 μmol/L (OR 2.44, 95% CI: 1.74–3.44) and ≥40 μmol/L (OR 4.84, 95% CI: 3.40–6.91) having increased likelihood of positive IOC when compared to those patients with bilirubin values of less than 20 μmol/L (both P < .001). With bilirubin included in the model, fever and organ dysfunction fail to reach the threshold of significance of <0.05 and are removed from the model, while the strengths of association for the dilated biliary tree/obstruction and CBD stone seen variables reduce in magnitude but remain statistically significant.
Multivariable Model Prediction Performance: Area Under the Curve (C-Statistic)
Versus Model 1.
Versus Model 2.
When testing the sensitivity of the exclusion of cases with missing or unknown values for the variables included in the model (Model 3), the total sample size reduces by 28 patients and provides only minor changes to the odds ratios estimated for the variables included in the model, and no significant change to the C-statistic (0.791, 95% CI: 0.762–0.820). Figure 2 provides the ROC for the three models considered in multivariable analysis, with the gap between Models 2/3 and Model 1 indicating the effect of considering bilirubin in a prediction model.
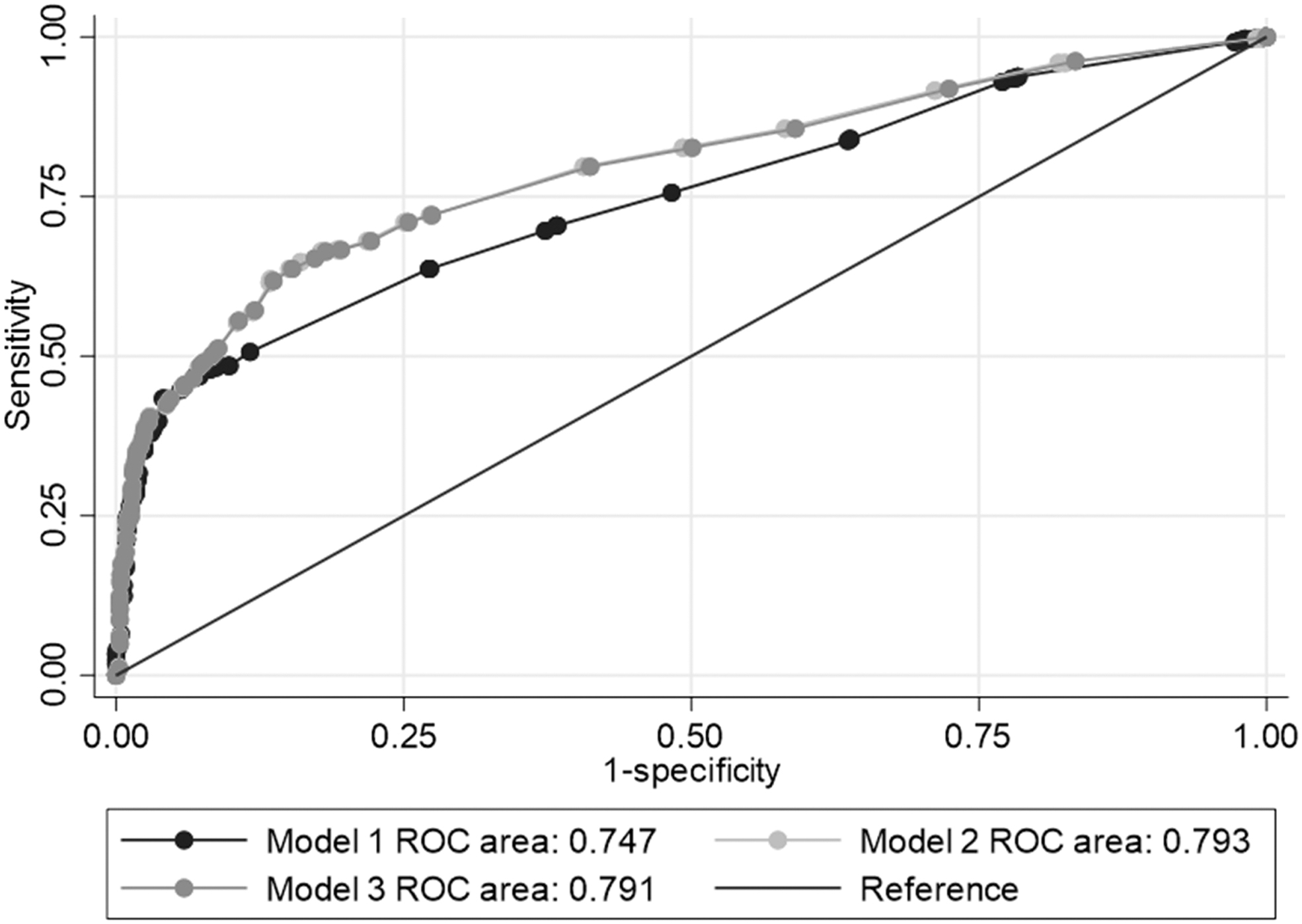
Receiver operating curve for Models 1–3 from multivariable model analysis.
Discussion
The accepted management regime for acute cholecystitis is emergency laparoscopic cholecystectomy; however, there remain many options for the management of concurrent choledocholithiasis. The management of choledocholithiasis usually requires confirmation radiologically, particularly if ERCP and its associated risks are contemplated. However, to delay emergency laparoscopic cholecystectomy for further imaging may also add risks to the patients, particularly in jurisdictions where intraoperative cholangiography is not routine. There is a need for better predictive models for concurrent choledocholithiasis in acute cholecystitis.
The overall aim of this study was to establish a simple and effective preoperative screening tool to identify patients who have a high likelihood of choledocholithiasis before undergoing laparoscopic cholecystectomy. The data from this study were compared to previous studies of similar nature, which were included in the NICE guidelines on management of gallstone disease.18–24 The current study contained the largest cohort size compared to previous studies; in addition, by including all patients undergoing laparoscopic cholecystectomy as opposed to only those with a clinical suspicion of choledocholithiasis, the generalizability is increased to encapsulate a cohort with lower pretest probability of CBDS. In turn, this approach may be more useful in the context of a screening tool, which needs to be applicable to all patients.
The key preoperative factors identified in this study were bilirubin level and abdominal USS, which produced strong positive and negative predictive values when used in conjunction. The study also demonstrated that not all positive USS findings were equivocal. A stone visualized within the CBD was highly specific for choledocholithiasis, whereas a dilated CBD was not only more sensitive but also more prone to false positives.
This variation may exist as the result is confounded by the impact of age on CBD diameter, with older patients typically exhibiting larger diameters. 25 This suggests that there is more nuance to interpreting the results of an abdominal USS than in a binary manner. Rather than using a binary cutoff value such as >6 mm, as used recently by Chisholm et al., 24 this study has relied on the reporting radiologists' assessment of these subtle differences and allow more accurate reporting of a dilated CBD, although this could and should be assessed with further studies.
The sensitivities and specificities of preoperative factors used to predict choledocholithiasis were comparable to prior studies; however, this is in the context of patients with a lower pretest probability compared to previous studies. This study has demonstrated that a serum bilirubin <10 μmol/L combined with a normal USS had a high negative predictive value for CBDS, whereas a serum bilirubin >45 μmol/L regardless of USS finding was highly predictive of CBDS. However, mild bilirubin elevation combined or not combined with USS findings of a dilated biliary tree had varying sensitivities and specificities that were not useful clinically.
Thus, a subset of patients can be confidently prepared for likely CBD stone management, but many patients are less predictable and may need further imaging such as intraoperative cholangiography to diagnose CBDS. CBD stone management pathways are now heading toward laparoscopic CBD exploration and postoperative ERCP rather than preoperative ERCP given the rates of spontaneous stone passage and evidence suggesting worse outcomes with ERCP before cholecystectomy.7,26,27
To ensure that all potential variables associated with positive IOC could be included in the modeling process with suitable power to detect statistical significance, it was not possible to consider a randomly selected internal validation cohort for this study. Therefore, a future extension to this study would be to determine how accurate the model performs in predicting the positive IOC patients in an external validation cohort. There were also some variables with missing observations that may impact on the precision of effect size for some statistically significant variables, although the analysis did explore how excluding cases with missing observations impacted on the predictive performance of the model. Some of these missing data may be due to patients having their acute cholecystitis diagnosed on computed tomography scan rather than USS, although the low numbers of these patients would be difficult to adjust for in future models.
While the modeling shows the additional benefit of including bilirubin in the model, the C-statistic of 0.79 indicates that improvements to the risk prediction of the model is possible with the consideration of some other unknown factors. Other limitations to this study include case selection, with only patients undergoing intraoperative cholangiogram at operation included, with nonoperative patients not included in the study. Patients undergoing preoperative ERCP may have also been missed. This, however, is offset by the denominators of this study, with a high patient population and over 350 abnormal IOC reported.
Conclusions
In summary, this study demonstrated that the preoperative factors identified in this study are not able to definitively rule in or rule out CBDS in patients before cholecystectomy. However, they do highlight that these relatively simple and noninvasive tests, when interpreted in conjunction, can significantly alter the clinical suspicion for CBDS, which does offer great clinical utility in decision-making for further imaging such as MRCP, as well as planning and preparing for intraoperative management. This can be especially useful in a center that does not routinely perform IOC during cholecystectomy; the authors believe that with some further refinement, this method can be used to remove the need for further routine investigations for CBDS in patients before undergoing emergency laparoscopic cholecystectomy.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
There was no funding received for this study.