
Abstract
Background:
Extralevator abdominoperineal excision (ELAPE) procedure leaves a large pelvic floor defect, and can result in a high rate of perineal hernia. Pelvic peritoneum reconstruction (PPR) could reduce the rate of perineal hernia. In this article, the authors reconstructed pelvic peritoneum by retracing running sutures with unidirectional barbed thread after laparoscopic ELAPE. The aim of the study is to evaluate the efficacy and safety of PPR by retracing running sutures with unidirectional barbed thread in laparoscopic ELAPE.
Materials and Methods:
Intact clinical data were collected retrospectively from 27 distal rectal cancer patients who underwent laparoscopic ELAPE. All the patients underwent PPR by retracing running sutures with unidirectional barbed thread in the operation. Pooled data of perineal-related complications were analyzed.
Results:
After retracing running sutures, the tension of pelvic peritoneum was enhanced. Of the 27 patients included, 2 patients had perineal dehiscence and 1 patient developed bowel obstruction. There were no instances of perineal hernia and pelvic peritoneal internal hernia.
Conclusions:
PPR by retracing running sutures with unidirectional barbed thread in laparoscopic can reduce the risk of perineal hernia.
Introduction
With the rapid developments and popularity of laparoscopic technology in the colorectal cancer, extralevator abdominoperineal excision (ELAPE) surgery has gained much more attention than ever before.
The ELAPE procedure improves the quality of resected specimens, but also leaves a large pelvic floor defect, which increased risk of perineal hernia.1–3 The pelvic peritoneum is supposed to be closed, as a standardized procedure to prevent postoperative complications, such as perineal hernia and radiation-induced enteritis. 4 Repair of peritoneal defects with a prosthesis or closure of the pelvic peritoneum has been developed to close pelvic defects after ELAPE.5–8
During ELAPE surgery we found that the reconstructed peritoneum is flabby in some patients, which could not provide enough supporting force. Thus, there is still a risk of perineal hernia after reconstruction of pelvic floor.9–12 Moreover, increase of intra-abdominal pressure can cause the small bowel fall into pelvic space through the defect area of peritoneal suture and lead to an internal hernia. 13
In this study, we describe a modified method of pelvic peritoneum reconstruction (PPR) by retracing running sutures with unidirectional barbed thread in laparoscopic ELAPE, which can reduce the risk of perineal hernia.
Materials and Methods
Patients
Intact data were collected retrospectively from 27 distal rectal cancer patients who underwent curative laparoscopic ELAPE from June 2017 to June 2022 at two centers, including The Second Hospital of Tianjin Medical University, Tianjin, China and The First Affiliated Hospital of Kunming Medical University, Kunming, Yunnan, China. This study was conducted in accordance with the Declaration of Helsinki, and with the approval of the Ethics Committee of the Second Hospital of Tianjin Medical University and the First Affiliated Hospital of Kunming Medical University. Written informed consent was obtained from all the participants (Table 1).
Clinical Data of Patients
Surgical procedure
Reconstruction of the peritoneum
The pelvic peritoneum edge was closed by running sutures with unidirectional barbed thread (3-0, V-Loc™ 180; Medtronic) from the bifurcation of common iliac artery to the back of bladder/uterus. The pelvic peritoneum defects were closed completely. Then turn back and the retracing suture is performed cephalad until it returns to the starting position (Fig. 1).
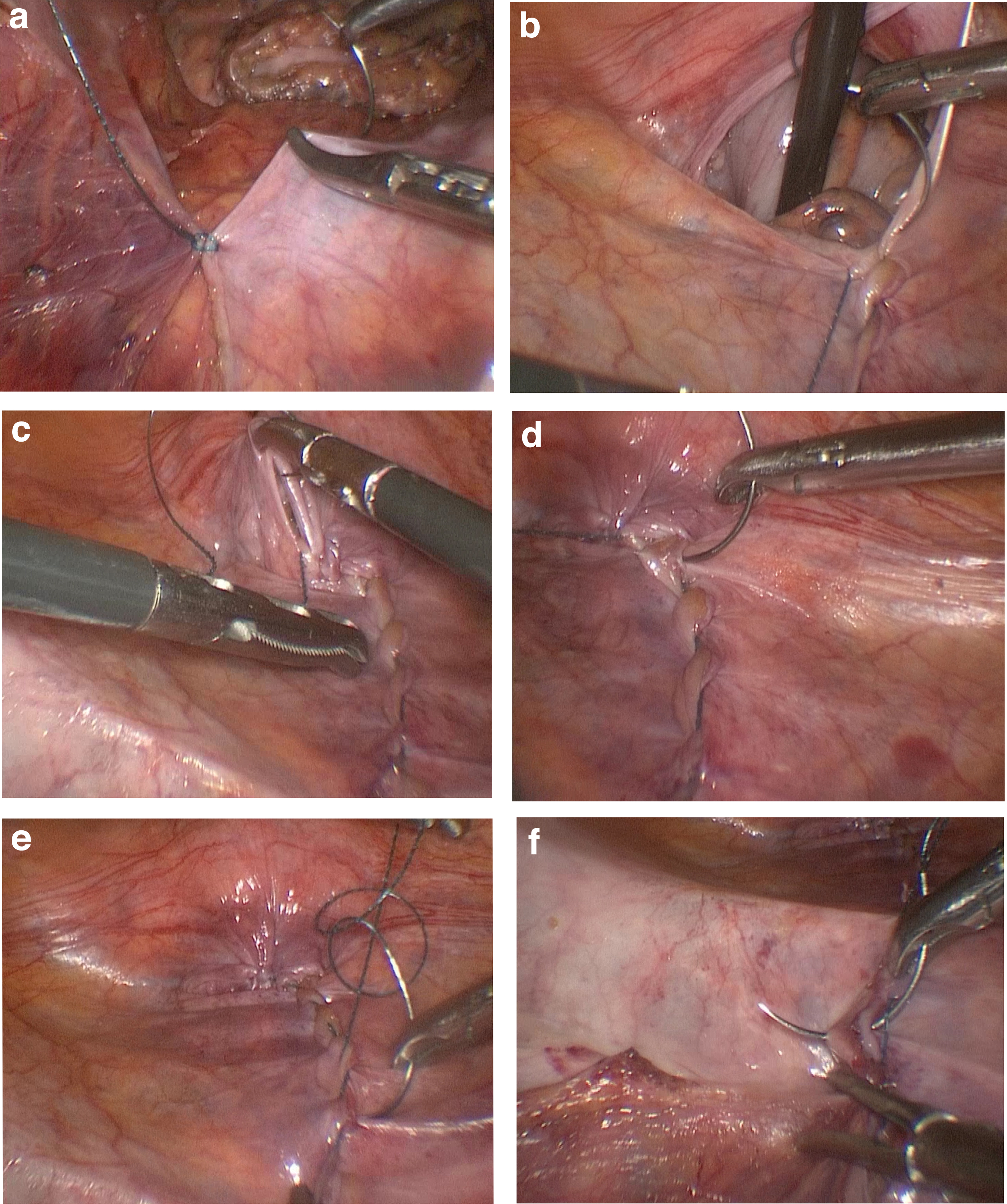
Procedure of modified pelvic peritoneum reconstruction.
Operating time for the peritoneum reconstruction, postoperative intestinal obstruction, perineal hernia, pelvic peritoneal internal hernia, perineal wound dehiscence, and chronic perineal pain was recorded.
Follow-up
Patients were followed up for an average of 12 months postoperatively. Carcinoembryonic antigen CEA was monitored every 3 months for 2 years, then every 6 months for a total of 5 years. Patients received chest/abdominal/pelvic computed tomography and lower abdominal magnetic resonance imaging every 6–12 months for a total of 5 years. Colonoscopy was delivered as described in the literature. 14
Statistics
All data were analyzed using the SPSS 23.0 software program (IBM Corp., Armonk, NY). Continuous variables were expressed as mean ± standard deviation. For all statistical analysis, P < .05 was considered to indicate a statistically significant difference.
Results
All of the 27 patients underwent PPR by retracing running sutures with unidirectional barbed thread in laparoscopic ELAPE. After retracing running sutures the pelvic peritoneum was obviously contracted and the tension of pelvic peritoneum was enhanced. Moreover, the double threads form double helix structure can provide additional supporting force for pelvic peritoneum (Fig. 2).
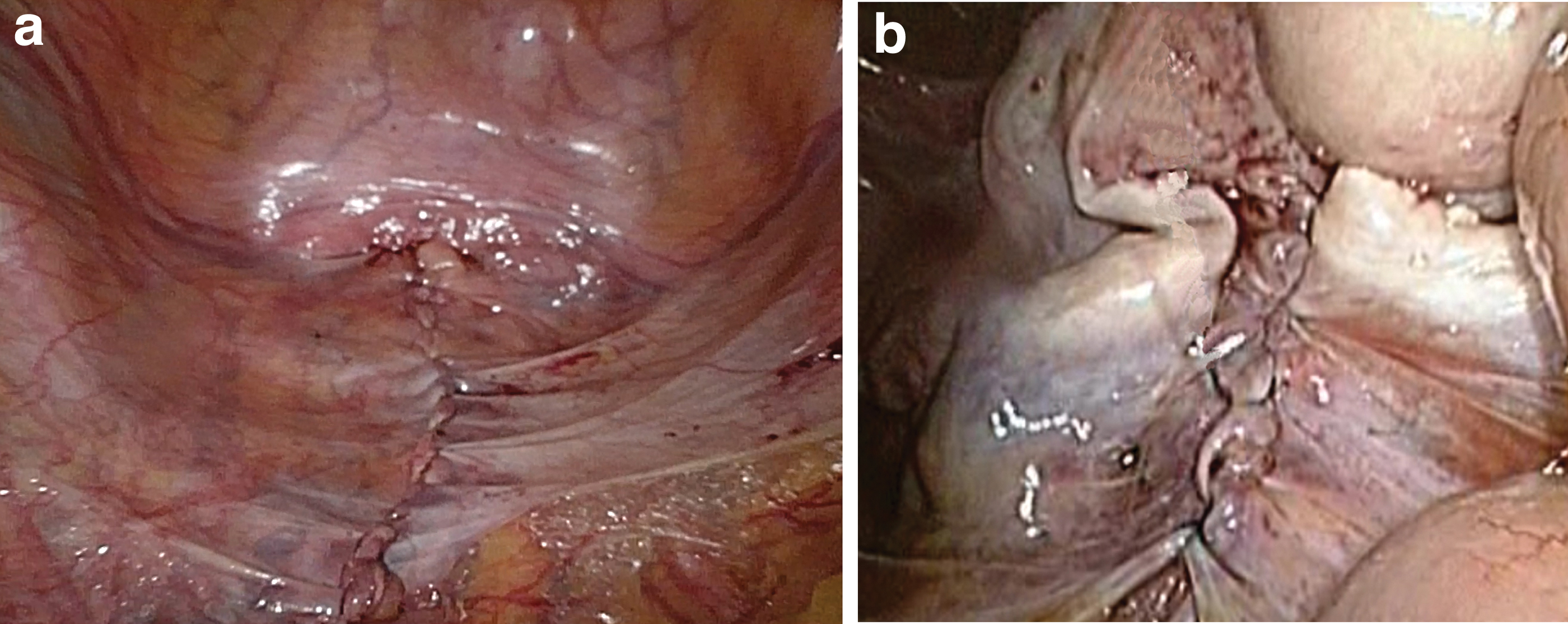
Reconstructed pelvic peritoneum by retracing running sutures with unidirectional barbed thread
One patient developed postoperative intestinal obstruction and 2 patients developed perineal wound dehiscence; those 3 patients were discharged after conservative treatment. None of the patients developed perineal hernia, pelvic peritoneal internal hernia, and chronic perineal pain after 1 year followed (Table 2).
Outcomes in Extralevator Abdominoperineal Excision
Discussion
PPR is capable of separating the abdominal and pelvic cavity so as to prevent the spread of infection from pelvic cavity. Therefore, the patient whose perineal wound dehisced can still be discharged from the hospital. 15 Furthermore, RPP can prevent the small bowel from descending into the pelvic cavity and patients who need radiotherapy are not prone to develop radiation enteritis after RPP.4,16–19
During ELAPE surgery we found that flabby peritoneum and the long distance of suture might be the main cause of perineal hernia under the effect of abdominal pressure. After retracing running sutures the pelvic peritoneum was obviously contracted and the tension of pelvic peritoneum was enhanced. Moreover, the double threads form double helix structure can provide additional supporting force for pelvic peritoneum.
In this study, all of the 27 patients underwent PPR by retracing running sutures with unidirectional barbed thread in laparoscopic ELAPE. After 1-year follow-up, none of the patients developed perineal hernia. It indicated that PPR by retracing running sutures with unidirectional barbed thread can reduce the risk of perineal hernia in laparoscopic ELAPE.
It was difficult to close pelvic peritoneum in laparoscopic surgery than open surgery. Sometimes the surgeon cannot find out the defects area of peritoneal suture timely, through which the small bowel may fall into the pelvic space and cause internal hernia. PPR by retracing running sutures with unidirectional barbed thread can efficaciously eliminate the defects area of peritoneal suture. In this study, after one-year follow-up, none of the patients developed pelvic peritoneal internal hernia, which indicated that PPR by retracing running sutures with unidirectional barbed thread can reduce the risk of internal hernia in laparoscopic ELAPE.
Although retracing running sutures will take a little more time, the mean operating time for the PPR was 25 minutes in this study. Our results suggest that retracing running sutures with unidirectional barbed thread is a simple and quick yet safe and reliable alternative option for PPR after ELAPE.
Footnotes
Authors' Contributions
All authors have contributed significantly and are in agreement with the content of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by grants from the National Natural Science Foundation of China (81660302 and 81660238) and The Youth Foundation of the second hospital of Tianjin Medical University (grant no. 2019ydey02, 2019ydey09, and 2020ydey20).