
Abstract
Introduction:
Paraesophageal hernias (PEH) represent a small subset of all hiatal hernias. PEHs are often found incidentally during radiographic or endoscopic studies performed for another reason. While asymptomatic or minimally symptomatic PEHs can be safely observed with nonoperative management, the majority of patients with symptomatic PEHs will benefit from surgical repair, typically via a laparoscopic approach. The decision to pursue surgical repair of PEHs is dependent on a thorough evaluation of the patient's symptoms as well as an appropriate workup of the relevant anatomy. This study aims to review components of the clinical workup of PEHs.
Materials and Methods:
A review of the contemporary literature addressing the issue of diagnostic workup of patients with PEHs was performed. Information from available studies were collected and organized into a brief review format.
Results:
Two key principles of the diagnostic evaluation of patients with PEHs include (1) establishing a link between patient symptoms and the PEH, and (2) identifying abnormal anatomy or physiology that may impact surgical repair (e.g., Barrett esophagus, esophageal stricture or diverticulum, delayed gastric emptying). While a multitude of radiographic, endoscopic, and functional testing options are available to evaluate PEH, selection of the appropriate test is dependent on patient clinical presentation.
Conclusion:
Successful management of PEHs depends on a thorough evaluation of patient symptoms and hernia anatomy. Therefore, patients with PEHs should undergo a history and physical examination, upper endoscopy, and obtain radiographic evaluation of the PEH (e.g., barium esophagram, computed tomography scan). Further testing should be directed by patient symptoms, especially in the case of discordance between symptoms and imaging findings.
Introduction
Hiatal hernias represent a disorder in which intra-abdominal contents, most often the stomach, herniate through the esophageal hiatus of the diaphragm into the mediastinum. 1 The vast majority (90%–95%) of hiatal hernias are classified as sliding hernias (type I) which occur when the gastroesophageal junction (GEJ) and proximal stomach migrates cephalad through the hiatus. 2 Of those sliding hiatal hernias that are symptomatic, the vast majority of symptoms are caused by gastroesophageal reflux (GER).1,3 The remaining 5%–10% of hiatal hernias (types II–IV) are classified as paraesophageal hernias (PEH) and involve herniation of the stomach (and in the case of type IV other intra-abdominal organs) into the mediastinum and alongside the esophagus. 4 While PEHs may also cause GER symptoms, patients with PEHs often have symptoms due to intermittent mechanical obstruction, ischemia, or bleeding (e.g., dysphagia, vomiting, epigastric or substernal pain, and anemia).5,6
Once diagnosed, PEHs often require further evaluation using a combination of testing modalities. While the exact tests obtained for each patient vary based on symptoms at presentation, common modalities include barium esophagram, upper endoscopy, high-resolution manometry (HRM), axial imaging, pH testing, and a gastric emptying study (GES).2,7 The main objective of obtaining these tests is to ensure that the patient's symptoms are secondary to the PEH as well as to identify relevant anatomy or pathology, which may impact surgical repair (e.g., Barrett esophagus, functional disorders of the esophagus or stomach).
To date, there is no consensus regarding the appropriate tests to obtain as a part of the diagnosis and potential preoperative workup for PEHs. As a result, controversies regarding which tests are necessary have persisted over the last two decades. 8 While there are multiple testing modalities available in the workup of PEHs, understanding the principles of what each test evaluates is imperative. In this article, we review each component of the clinical evaluation of PEHs and discuss the rationale for testing and which tests may be omitted in certain circumstances.
Materials and Methods
A review of the contemporary literature regarding the diagnostic work-up of patients with PEHs was performed. PubMed was queried for studies published between 1990 and 2022 using the following keywords: paraesophageal hernia, hiatal hernia, dysphagia, regurgitation, gastroesophageal reflux disease, anemia, dyspnea, endoscopy, barium esophagram, manometry, pH testing, and GES. To provide an experience-based review, we selected studies which provided the greatest contributions to the literature addressing workup of PEHs. The information from each of these studies was then compiled and organized into a brief review of all available diagnostic testing options for PEHs. We have included the personal preferences/anecdotal experience of the authors, in addition to evidence-based recommendations.
Diagnostic and Preoperative Workup
History and physical examination
As with any disease process, a thorough history and physical examination remain critical components of the diagnostic workup of PEH. The main objective of the history is to obtain information regarding any potential hernia-related reflux, obstructive, hemorrhagic, or ischemic symptoms. These may manifest as heartburn, regurgitation, dysphagia, epigastric or substernal pain, postprandial fullness, nausea, vomiting, weight loss, and/or anorexia. Attention should also be paid to evaluating for dizziness, fatigue, or dyspnea as these may occur in patients with PEHs secondary to anemia from Cameron's erosions or cardiac dysfunction due to hernia compression. In rare cases, patients with PEH may present with gastric strangulation secondary to an acute volvulus. In cases of acute gastric strangulation patients may report acute onset substernal pain, inability to tolerate oral intake, and retching with an inability to vomit. 9 These patients may also present with signs and symptoms of systemic sepsis.
While there are no specific physical examination findings associated with PEH, a complete examination of the patient's abdomen should be completed during initial assessment. Evaluation for abdominal wall hernias or previous surgical scars provides valuable information should the patient requires operative repair of their PEH. In patients who present with acute strangulation or perforation secondary to gastric volvulus, physical examination findings may include peritonitis and hemodynamic instability. These findings should prompt immediate surgical evaluation.
Barium esophagram
A barium esophagram represents an important component of the evaluation of PEHs. The study establishes the diagnosis of a PEH, while also providing information regarding the anatomy of the hernia and esophagus (Fig. 1). In particular, a barium esophagram will reveal the amount of stomach herniated into the mediastinum as well as the location of the GEJ in relationship to the esophageal hiatus. 2 This study has the added benefit of providing information on the potential presence of concurrent esophageal anatomic pathology that may impact surgical planning (e.g., strictures, diverticulum, shortened esophageal length). Furthermore, a video barium esophagram may reveal evidence of a functional or mechanical obstruction based on bolus transit. 10
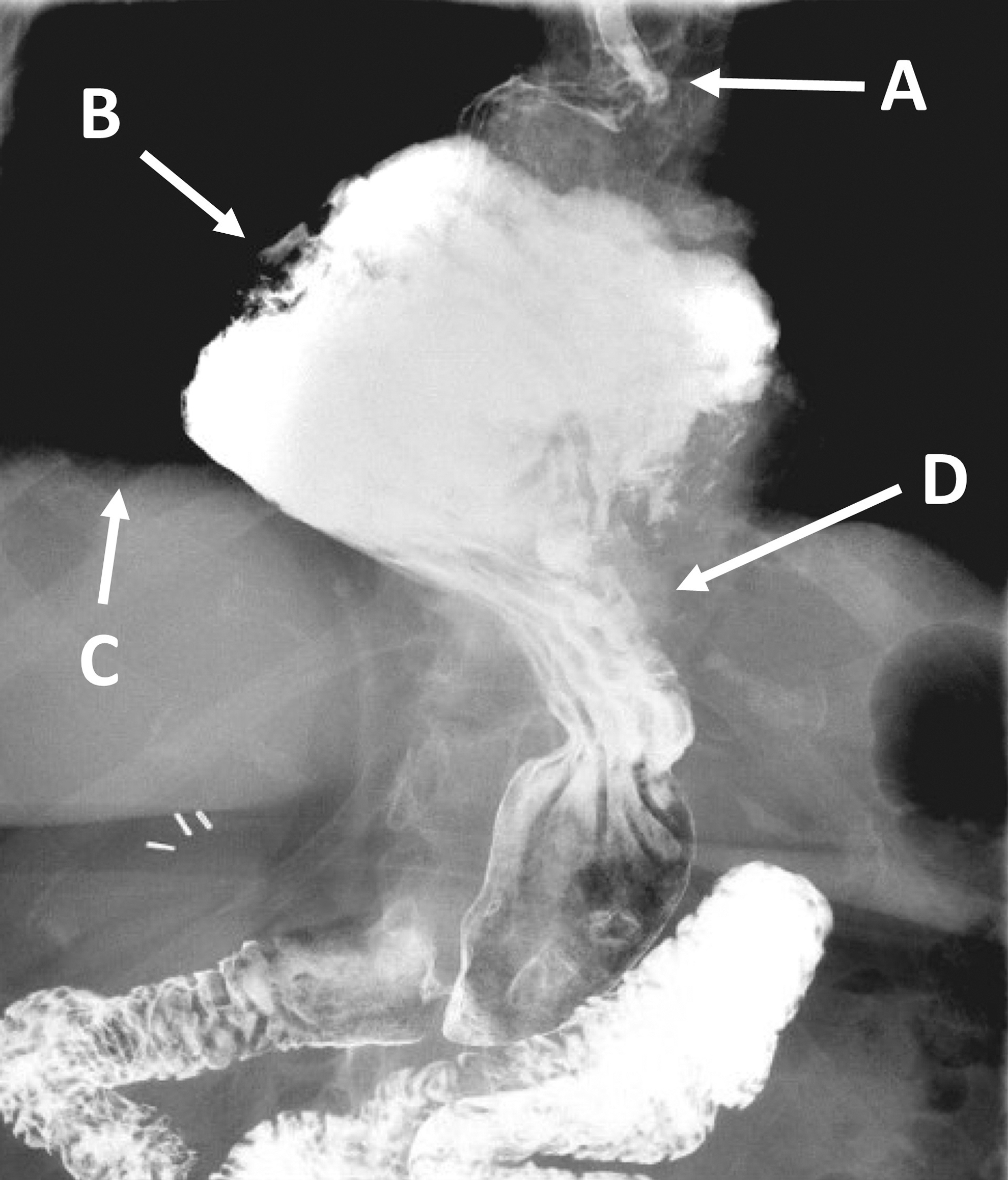
A barium esophagram showing a large paraesophageal hernia. A tortuous esophagus
In actual practice, patients have often already had a chest and/or abdominal computed tomography (CT) scan performed when presenting for evaluation of a PEH. While not a functional study, CT will demonstrate the size of the hernia and degree of volvulus of the stomach. Most often if the patient has had a CT and high-quality upper endoscopy, we do not feel it is necessary to also obtain an UGI preoperatively unless there is suggestion of an esophageal diverticulum or other altered anatomy that had not been adequately characterized.
Cross-sectional and plain film imaging
Many PEHs are incidentally found on radiographic studies obtained for the evaluation of vague abdominal or thoracic symptoms. As a result, patients will often present for further evaluation of a PEH after the hernia was noted on chest X-ray or CT scan (Fig. 2). Findings of a PEH on chest X-ray include retrocardiac soft tissue opacity as well as intrathoracic air–fluid levels. While retrocardiac air–fluid levels is indicative of a hiatal hernia, CT scans with oral and IV contrast are more sensitive radiographic measures of PEHs than plain film imaging.
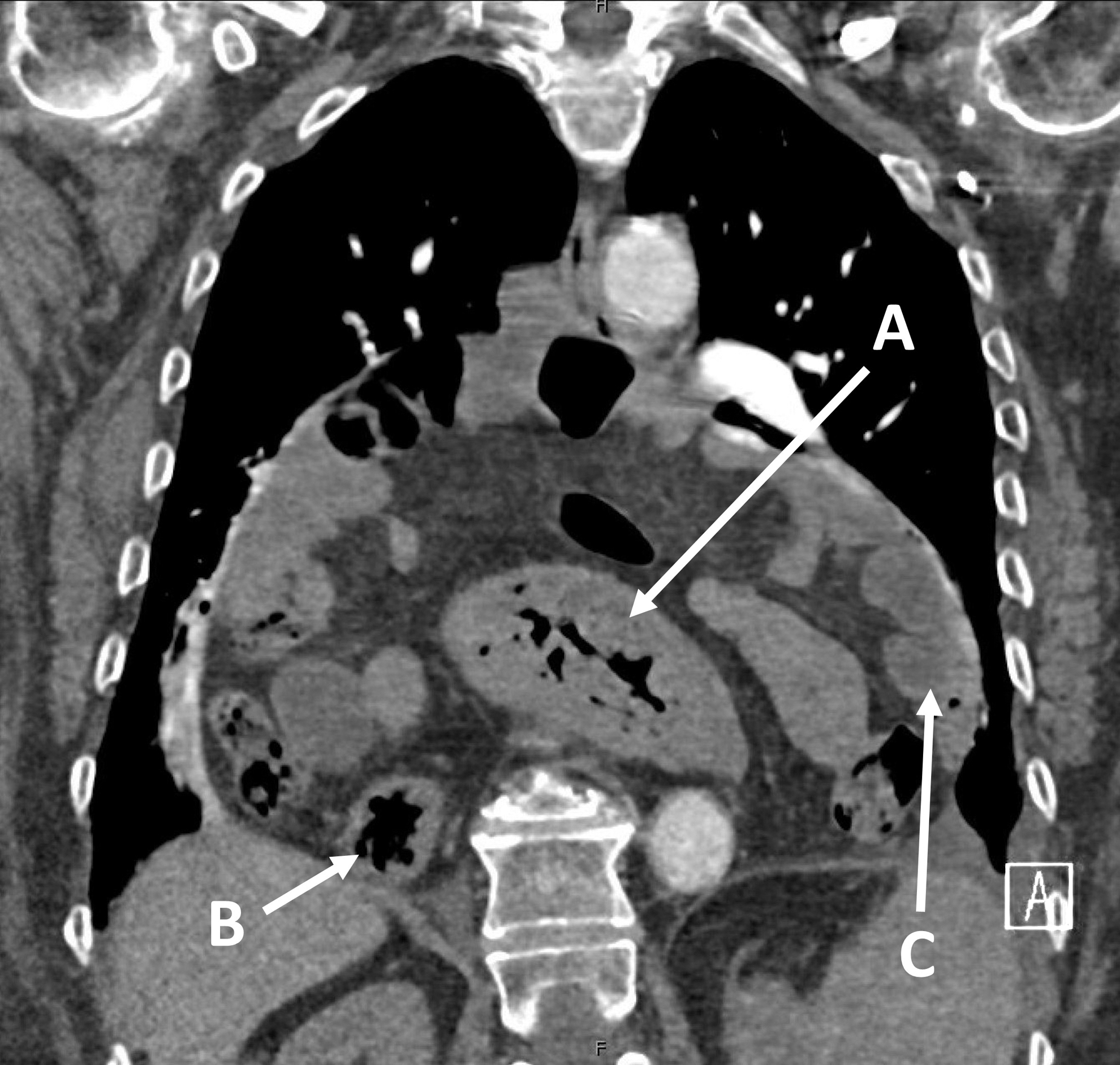
A giant paraesophageal hernia is seen on a coronal image of a CT scan. This is a Type IV hernia containing stomach
These scans provide information regarding the width of the hiatal defect as well as axial length and orientation of the PEH. CT scans are particularly useful in the acute setting when evaluating a patient for possible gastric volvulus. However, as with the barium esophagram, the primary value of the CT scan is to establish the diagnosis in patients with symptoms, which may be secondary to PEH. As such, there may be little utility in obtaining a CT scan in patients who have already undergone barium esophagram (and vice versa).
Upper endoscopy
Thorough upper endoscopy is an absolute requirement before proceeding with PEH repair. Endoscopic evaluation allows for direct visualization of the esophageal, gastric, and duodenal mucosa (Fig. 3). Care is taken during endoscopy to assess for mucosal changes that may relate to patient-reported symptoms or impact operative planning, such as erosive esophagitis, eosinophilic esophagitis, strictures, masses, Barrett esophagus, or Cameron's ulcers. In addition, upper endoscopy may provide information concerning esophageal length and the possibility of a foreshortened esophagus. Endoscopic evidence of a dilated esophagus or retained food within the esophagus may also indicate the degree of mechanical obstruction or presence of a concurrent motility disorder.

A paraesophageal hernia seen in retroflexed view during upper endoscopy. The herniated stomach
While endoscopy is capable of establishing the presence of hiatal hernias, obtaining accurate measurements of the hernia size, or if there is a paraesophageal component, remains difficult. Anatomic delineation between Type I hiatal and PEH is typically better evaluated by radiographic studies such as CT scan or barium esophagram. In our experience, upper endoscopy most often underestimates the degree to which a hiatal hernia contains a paraesophageal component. Patients with obstructive symptoms and “hiatal hernias” often undergo multiple endoscopies over months or even years before an esophagram shows that a PEH with partial volvulus is the obvious etiology of their symptoms.
High-resolution manometry
The use of HRM in the workup of PEH remains controversial. Under ideal settings, HRM in patients with PEHs is able to identify the level of the crura, the location of the lower esophageal sphincter (LES), measurements of esophageal function (e.g., LES relaxation, esophageal body motility, bolus transit), as well as the respiratory inversion point (i.e., location of the diaphragmatic hiatus).
While these data points may prove useful in the evaluation of esophageal motility, especially in cases of sliding hiatal hernias, manometric measurements can be challenging to obtain in patients with PEHs. In particular, placement of the catheter below the diaphragm and across the lower esophageal sphincter in these patients may be technically difficult and may require endoscopic assistance. Furthermore, HRM in the setting of a PEH may be challenging to interpret as measurements (especially LES relaxation pressure) may reflect mechanical obstruction secondary to the herniated stomach rather than a functional disorder.
Some have argued that the use of HRM in the preoperative workup of PEH may aid in the choice of which fundoplication to create (partial versus total). 11 Others have countered that a high-quality video barium esophagram is sensitive enough to detect major functional disorders, 10 obviating the need for routine preoperative HRM in the majority of patients with PEH. Previous studies have also shown no difference in the type of fundoplication performed during PEH repair based on presence or omission of preoperative HRM. 12 Furthermore, there appear to be minimal differences in postoperative outcomes between patients undergoing partial versus total fundoplication.13–15
In our practice, we almost always perform a partial fundoplication in the setting of a PEH repair, as partial fundoplication has been shown to result in equivalent GER control with less functional side effects (dysphagia and gas bloat). In addition, it would be extremely rare to encounter a patient with both a PEH and separate esophageal motility disorder, and the rate of “false positive” HRM showing esophagogastric junction outflow obstruction due to mechanical obstruction from the PEH is high. As a result, for most PEH patients, we do not obtain a HRM preoperatively.
pH testing
Unlike in cases of sliding hiatal hernias, the role of pH testing in patients with PEH remains limited. Documentation of increased esophageal acid exposure may be helpful in patients with PEH who present with predominantly reflux-associated symptoms. 1 However, pH testing does not alter treatment in patients presenting with obstructive symptoms (e.g., dysphagia, postprandial pain, vomiting) and therefore provides little utility in the workup of these patients. In routine clinical practice, we very rarely obtain pH testing before PEH repair.
Gastric emptying study
A GES may serve as an important part of the diagnostic workup of PEH in patients who exhibit discordance between symptoms and imaging findings. 2 In particular, a GES may be useful in patients who present with symptoms that may be due to gastroparesis (e.g., early satiety, postprandial nausea, and bloating). Proper evaluation of gastric motility would be critical in these patients to prevent continued symptoms despite surgical repair of the PEH. Furthermore, preoperative evidence of delayed gastric emptying in patients with PEHs may impact surgical repair with the addition of pyloroplasty to the PEH repair.
It is important to carefully review the results of the GES with the radiologist to determine whether delayed emptying is due to obstruction from the PEH or true gastroparesis. If the radionucleotide tracer is retained, cephalad to the diaphragm, this is an indication that the PEH is the cause of delayed emptying. Conversely, if the tracer is delayed, in passage through the stomach below the hiatus, the patient may have true gastroparesis separate from the PEH.
Other testing
Several additional tests may prove useful in the workup of PEHs depending on patient symptoms. For example, patients who present with dyspnea on exertion in the setting of large PEHs should undergo pulmonary and cardiac testing before operative intervention to ensure that the dyspnea is not due to a cause unrelated to the PEH. Pulmonary function testing would allow for an evaluation of pulmonary function in an attempt to rule out primary pulmonary pathology. Similarly, cardiac evaluation (e.g., echocardiogram, stress test), may prove useful in ruling out primary cardiac pathology. Patients with PEH who have dyspnea without a clear pulmonary or cardiac etiology represent a diagnostic dilemma. PEH itself can result in dyspnea, which likely occurs due to left atrial compression by the herniated stomach (Fig. 4). 16
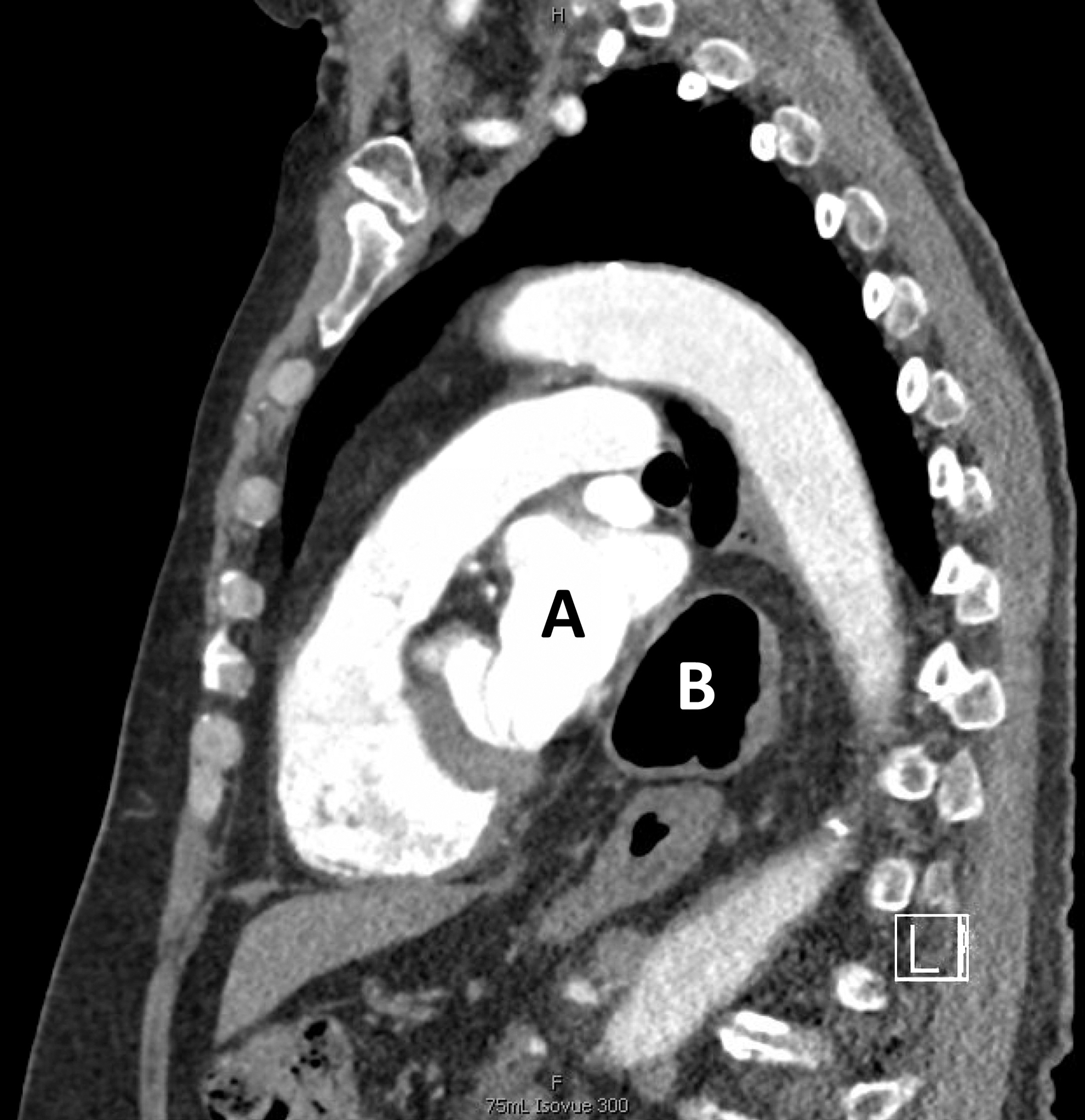
A sagittal CT scan section shows the left atrium
In patients with unexplained dyspnea in addition to gastrointestinal (GI) symptoms, the surgeon can proceed with PEH repair without testing specifically linking the dyspnea to the PEH. However, in patients with isolated idiopathic dyspnea and no GI symptoms, we often obtain (in consultation with the patient's cardiologist) dedicated cardiac imaging (e.g., cardiac CT or magnetic resonance imaging) to determine the degree of left atrial compression due to the PEH. This can help in counseling patients as to the likelihood their symptoms are in fact due to the PEH and thus the chances they will improve/resolve after repair. Overall, ∼80% of patients with dyspnea on exertion will have a significant improvement after PEH repair.
Additional testing that may prove useful in patients with PEHs includes full endoscopic workup (e.g., upper endoscopy, colonoscopy, possible capsule endoscopy, or device-assisted enteroscopy) for those who present with anemia. The goal of thorough endoscopic evaluation is to ensure that the anemia can be attributed to the PEH (i.e., Cameron's erosions) before consideration of surgical repair. In our opinion, patients with iron-deficiency anemia should undergo a colonoscopy preoperatively if one has not been performed within the recommended screening interval, but endoscopic evaluation of the small bowel is rarely needed.
Conclusions
Proper management of PEHs is dependent on a detailed evaluation of patient symptoms and relevant anatomy. If the decision is made to proceed with surgical repair, it is critical that the PEH workup has established a link between patient symptoms and the hernia. In addition, care must be taken to fully assess for esophageal and gastric pathology that may impact surgical planning. As such, patients presenting with PEH should undergo a thorough history and physical examination, obtain radiographic evidence of a PEH (e.g., barium esophagram, CT scan), and complete endoscopic evaluation of the esophagus and stomach. Additional testing should be guided by patient clinical presentation, with attention paid toward evaluating any potential discordance that may be present when comparing symptoms to radiographic or endoscopic findings.
Footnotes
Disclosure Statement
T.K.Y.: None.
E.N.T.: Boston Scientific—consulting.
Funding Information
There are no funding sources for this manuscript.