
Abstract
Introduction:
Esophageal variceal bleeding (EVB) is a potentially fatal complication of cirrhosis. The purpose of the present study was to evaluate the safety and efficacy of a novel technique of balloon-occluded esophageal varices (EVs) obliteration (BEVO) for EVs classified as F2 (medium size, F2-EVs) and F3 (large size, F3-EVs).
Materials and Methods:
Between December 2020 and December 2021, a total of 73 consecutive patients with EVs were treated using BEVO. An injection of sclerosant was administered via direct puncture of the varices during balloon occlusion. Immediate postprocedural Doppler endoscopic ultrasonography (EUS) was conducted to evaluate the blood flow in the EVs. Several factors, including the technical success, controlling of acute bleeding, intraoperative bleeding at the injection site, variceal eradication, variceal recurrence, and BEVO-related complications, were assessed.
Results:
BEVO was successfully performed in all patients. Immediate hemostasis was achieved in 100% (25/25) of patients with active EVB. The incidence of injection site intraoperative bleeding presenting as oozing and spurting bleeding was 76.71% (56/73) and 8.22% (6/73), respectively. Based on Doppler EUS and endoscopic examination, EVs were completely eradicated in 71 out of 73 patients (97.26%) after three sessions. A total of 3 (4.11%) patients were diagnosed with EV recurrence during follow-up after complete EV eradication. Retrosternal chest discomfort (13.70%; 10/73) and abdominal bloating (2.74%; 2/73) were spontaneously relieved after a few days. No serious BEVO-related complications were observed.
Discussion:
BEVO is a convenient and effective treatment for obliterating F2 and F3 EVs. Clinical Trial Registration No. ChiCTR2000039974.
Introduction
Although esophageal variceal ligation (EVL) is the first-line treatment for esophageal variceal bleeding (EVB), it is associated with a high risk of variceal recurrence. In addition, repeated EVL procedures limit the pliability of the mucosa and prevent further successful banding. 1
In recent years, our group has developed a novel technique for embolizing esophageal varices (EVs) with the aid of balloon occlusion, and this technique is referred to as balloon-occluded EVs obliteration (BEVO). Similar to balloon-occluded retrograde transvenous obliteration (BRTO) for embolizing gastro-renal shunts, BEVO uses sclerosant to embolize EVs. Preliminary evidence has indicated that this technique eliminated EVs more effectively than EVL. 2
In the present study, the BEVO balloon was modified into a 4-cm-long column to improve occlusive effects on EVs. As our primary objective, a prospective multicenter study was conducted to evaluate the technical success, acute bleeding control, intraoperative bleeding at the injection site, variceal eradication, variceal recurrence, and procedure complications in patients undergoing BEVO with F2-EVs and F3-EVs.
Materials and Methods
Ethical Statement
The present study was performed according to the Declaration of Helsinki, which was approved by the institutional review board of The First Affiliated Hospital of Anhui Medical University,
Patients
Three medical centers in China were involved in this prospective clinical trial: The First Affiliated Hospital of Anhui Medical University (Hefei, Anhui, China.), The First Hospital of Bengbu (Bengbu, Anhui, China.), and The Hospital of SheXian (Huangshan, Anhui, China). The patients were performed BEVO between December 2020 and December 2021. All patients signed an informed consent form acknowledging the risks associated with BEVO. The end-point of the follow-up was June 2022.
The inclusion criteria were as follows: (1) patients diagnosed with liver cirrhosis by biopsy or clinical examination and imaging, including ultrasound, computed tomography, or magnetic resonance imaging; (2) patients with moderately enlarged, beady varices (F2) or markedly enlarged, nodular or tumor-shaped varices (F3) according to the Japanese Society of Endoscopy (2010) guidelines; 3 and (3) age between 18 and 80 years.
The exclusion criteria were as follows: (1) diagnosed or accompanied by isolated gastric varices and ectopic varices; (2) poor overall health status, including multi-organ failure, hepatic encephalopathy grade III and IV, and malignancies other than hepatocellular carcinoma (HCC) meeting the Milan criteria; (3) history of endoscopic injection sclerotherapy (EIS), EVL, or transjugular intrahepatic portosystemic shunt treatment or liver transplantation; (4) inability to tolerate endotracheal intubation and anesthesia evaluation; (5) Doppler endoscopic ultrasonography (EUS) was not used to evaluate the blood flow of EVs; (6) allergic to lauromacrogol or methylene blue; and (7) refused to participate in the study.
The present prospective study was approved by the Clinical Research Ethics Committee of the First Affiliated Hospital of Anhui Medical University (Hefei, Anhui, China.) and was conducted according to the Declaration of Helsinki.
Materials and endoscopic procedure
Patients who were enrolled in the present study with the diagnosis of F2 or F3 EVs.
BEVO was performed under intravenous anesthesia with endotracheal intubation and mechanical ventilation, as previously reported.4,5 The disposable sterile cylinder-shaped balloon (Jiangsu Vedkang Medical Science and Technology Co., Ltd.) was tested for air leakage before BEVO.
After the deflated balloon had been fixed over an endoscope (GIF Q260J; Olympus Corporation) at a distance of 3 cm away from its distal end (Fig. 1a), a transparent cap (MAJ-290; Olympus Corporation) was placed at the distal end of the endoscope. While the lubricated endoscope and the deflated balloon were placed close to the target varices, a total of 20 mL of air was then pumped into the balloon through the catheter (Fig. 1b).
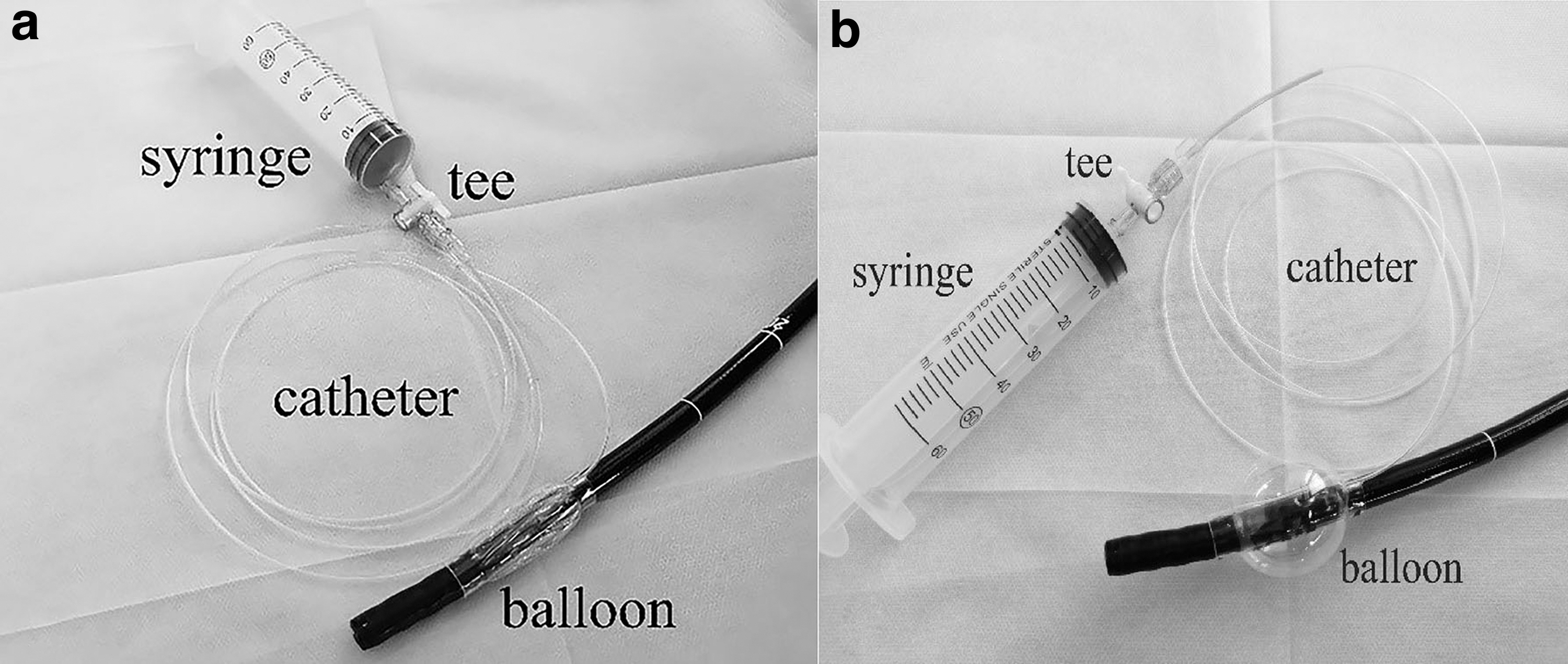
When the diameter (3.5 cm) of the inflated balloon was larger than the inner diameter of the esophagus (ranging between 2.5 and 3.0 cm), EVs were effectively blocked. 6 Subsequently, a 25-gauge sclerotherapy needle (Boston Scientific Corporation) with a transparent sheath was introduced through the working channel of the endoscope and used to puncture the target EVs. It was necessary to draw blood back into the transparent sheath to ensure correct needle placement.
A solution of 1% lauromacrogol (Shanxi Tianyu Pharmaceutical Co., Ltd) was mixed with methylene blue (Jumpcan Pharmaceutical Group Co., Ltd.), which served as a tracer, and was injected into the target EVs until the color of methylene blue appeared on the EVs and perforating branches. Methylene blue disappeared rapidly from the EVs if the balloon diameter was insufficient to occlude the varices completely, so reinflation of the balloon to a diameter of 4 cm was required. BEVO was performed again according to the operating procedure.
Once the intravenous injection was completed (Fig. 2a), the sheath or transparent cap continued to press the injection site for 2–3 minutes to prevent sclerosant overflow and bleeding (Fig. 2b). Generally, because of the interconnection of EVs by perforating vessels, a single injection in the largest target varices was sufficient to provide sclerosant to all remaining varices. If some of the EVs were not stained with methylene blue, supplementary injections of lauromacrogol were administered. The total dose of lauromacrogol was <35 mL. During this procedure, the inflated balloon was kept occluded for 20–30 minutes to induce thrombosis in the EVs. Usually, the greater the size of the EVs, the longer the inflation time.
After treatment was completed, the balloon was deflated and carefully removed together with the endoscope through the esophagus. Doppler EUS was subsequently used to confirm the thrombosis in EVs and the absence of blood flow. After 1 week, if EVs were not completely eradicated, BEVO was repeated.
Follow-up and definitions
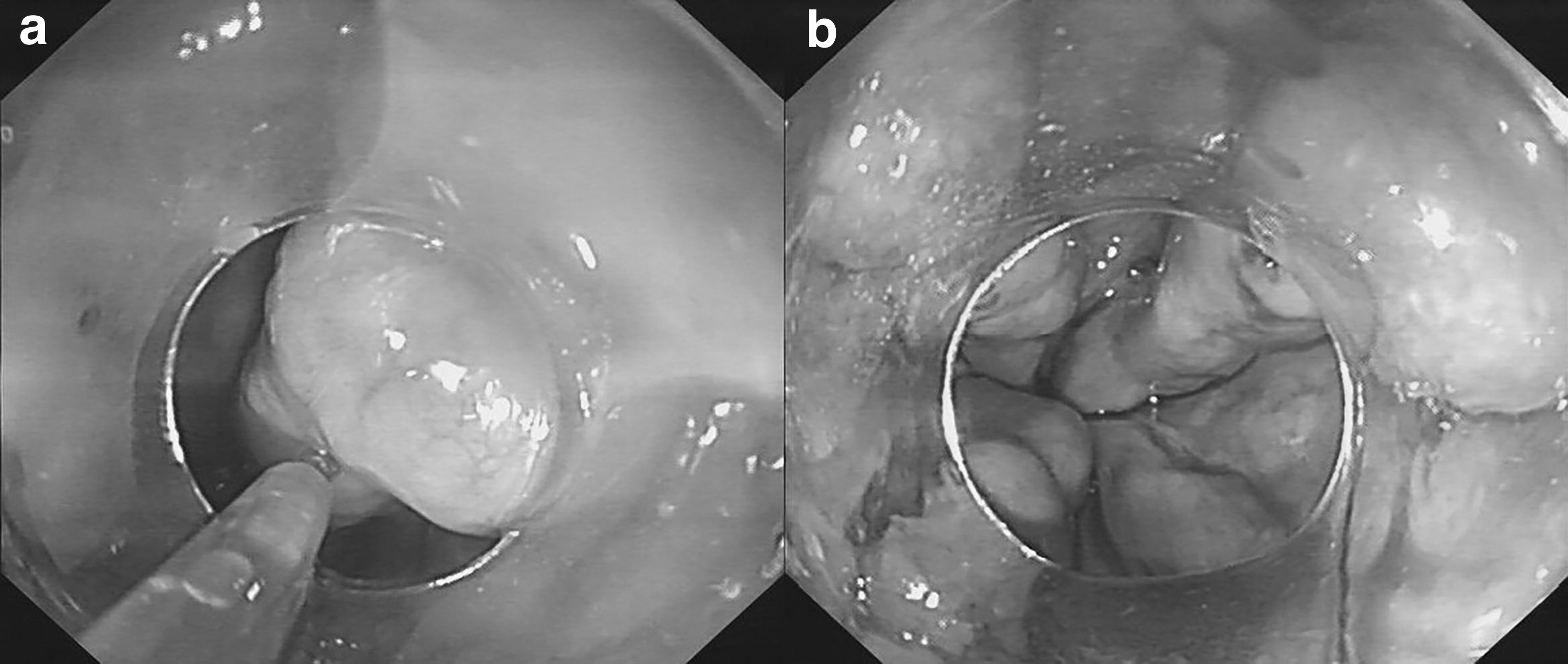
Direct endoscopy examination and BEVO were repeated monthly until EVs were completely eradicated (Fig. 3a, b). After EV eradication, a repeat endoscopy examination was performed at 6-month intervals. The technical success was defined as a marked shrinkage as well as the immediate elimination of EVs during the BEVO procedure. Eradication was defined as the absence of flow within the esophageal wall, as confirmed by Doppler EUS, and by the absence of visible EVs during endoscopy. Hemostasis referred to the successful arrest of bleeding attributed to EVs within 120 hours after BEVO, according to the Baveno VII criteria. 7

Rebleeding was defined as an episode of bleeding arising from EVs with clinical signs, including hematemesis, melena, or a decrease in hemoglobin >3 g/dL at >120 hours post-treatment.8,9 Postoperative BEVO-related complications were collected through clinical follow-ups.
Statistical analysis
Quantitative values with a normal distribution are presented as the mean ± standard deviation (SD), and all other data are presented as the median (interquartile range). Categorical variables are expressed as percentages. Statistical analyses were performed using SPSS 22.0 software (IBM Corp., Armonk, New York, NY).
Results
Patient characteristics
The clinical characteristics of the patients are summarized in Table 1. A total of 73 patients with EVs (27 women and 46 men; mean age, 54.16 ± 11.06 years) received BEVO at the three medical centers between December 2020 and December 2021. Hepatitis B virus infection was the primary cause of cirrhotic EVs in the present study. The severity of liver disease was graded according to the Child-Pugh scoring system, and 43 (58.9%) patients were graded as Child's class A and 30 (41.1%) as class B.
Clinical Characteristics of the Patients
IQR, interquartile range; SD, standard deviation.
Among them, 7 (9.59%) patients had concomitant HCC. The form of EVs in 51 (69.86%) patients was categorized as F2 and that in 22 (30.14%) patients as F3. Red color signs were observed in 73 (100%) patients. At the initial endoscopy, 25 (34.25%) patients had active EVB.
Technical success
Procedural and follow-up data are summarized in Table 2. All patients entered the follow-up phase. The median follow-up period was 476 days (348.5–551.5 days). BEVO was successfully performed in 73 patients, achieving a technical success rate of 100%. Immediate hemostasis was achieved in 100% (25/25) of patients with active EVB, without recurrence of bleeding over the next 120 hours, and none of the patients exhibited rebleeding episodes during the follow-up period.
Procedural and Follow-Up Data
Hemostasis was performed on 25 patients during the procedures.
One patient required four sessions and another patient required five sessions to achieve complete eradication.
IQR, interquartile range; SD, standard deviation.
Eradication and recurrence
Complete eradication of EVs was achieved in 71 (97.26%) patients after three sessions, of whom 47 (64.38%) required a single session, 19 (26.03%) required two sessions, and 5 (6.85%) required three sessions, with blood flow disappearance confirmed by Doppler EUS. In 2 cases, complete eradication required four and five sessions, respectively. Reinjection of lauromacrogol was performed in the 2 patients during endoscopic surveillance. However, 3 (4.11%) patients were diagnosed with EV recurrence on routine follow-up endoscopic examination after complete EV eradication.
Endoscopic outcomes
The mean volume of lauromacrogol per session was 17.73 ± 7.86 mL. In total, only 8.22% (6/73) of patients exhibited spurting bleeding in the procedure. The EVs of 73.97% (54/73) of patients were compressed by the needle sheath or transparent cap on each puncture site, and 26.03% (19/73) of patients exhibited spontaneous cessation of bleeding. As determined by the retention of the mixture of methylene blue and lauromacrogol in EVs under direct endoscopic visualization, the mean occlusion time of the balloon during each session was 13.52 ± 4.42 minutes.
Complications
There were no fatal or severe complications, including treatment-induced ulcers, perforation, stricture, and ectopic embolism, during the follow-up period. As shown in Table 3, the overall complication rate in the present study was only 16.44% (12/73). A total of 10 out of 73 (13.70%) patients experienced retrosternal chest discomfort the day after BEVO, which was spontaneously relieved after a few days. Mild-to-moderate abdominal bloating or distension was recorded in 2 patients (2.74%) a few hours after the procedure, and this was relieved spontaneously.
Complications
In addition, no damage, such as bleeding, mucosal ulceration, or mucosal injury, to the esophageal mucosa in the area where the balloon compressed was observed. None of the 73 patients died during the follow-up period.
Discussion
In our previous studies, an endoscopic tip balloon that could be used to occlude EVs and remove foreign bodies from the esophagus was developed.4,5,10 In a previous study, a balloon-assisted sclerotherapy technique using lauromacrogol as a sclerosant was similar to BRTO as an approach to occluding varices and inducing thrombosis, which resulted in marked varices shrinkage and disappearance. However, the research also revealed that it was challenging to puncture and inject EVs of type F1, and BEVO was more appropriate for F2 and F3 EVs.
The present study was the first report of BEVO in the treatment of F2 and F3 EVs. To decrease the heterogeneity of endoscopic operator-individual techniques, the study of this case series was conducted in three hospitals. The preliminary results of our research indicated that BEVO was performed in 73 patients, achieving a technical success rate of 100% and immediately efficient hemostasis in active EVB (25/25). Endoscopic follow-up and Doppler EUS confirmed that 97.26% (71/73) of patients had completely eradicated EVs after three sessions, and all patients did after five sessions. Recurrence of EVs occurred in 3 patients after 6 months. None of the patients had rebleeding episodes during the follow-up period.
In the present study, a dose of lauromacrogol ranging between 10 and 20 mL was regularly used for the complete filling of the EVs during the BEVO procedure. The patients who underwent sclerosant embolism mostly required a mean ± SD volume of embolic agents of 17.73 ± 7.86 mL. Considering that our two procedural eradication-related failures after three sessions resulted from using an insufficient amount of lauromacrogol, we hypothesized that the amount of lauromacrogol should be the amount needed to fill all EVs.
Further, the systemic effects of lauromacrogol were alleviated by occluding outflow veins during obliteration, which was the notable difference from EIS.11–13 A total of 10 patients experienced retrosternal chest discomfort, which was spontaneously relieved after a few days and associated with endotracheal intubation. Mild-to-moderate abdominal bloating was recorded in 2 patients a few hours after the procedure, and this might be induced by the accumulation of carbon dioxide in the upper gastrointestinal tract after balloon occlusion.
The advantages of the novel sclerosant embolism technique termed BEVO were validated at three medical centers. Compared with the lifebuoy-shaped balloon reported in our previous studies,4,5 a modified cylinder-shaped balloon was utilized during BEVO, which could more completely occlude EVs, as confirmed by the long-term non-fading of the methylene blue tracer. In the present study, F2 and F3 EVs were suitable for puncture to achieve embolization; however, larger varices required more sclerosant and a longer occlusion time.
In addition, Doppler EUS was used to evaluate blood flow in EVs following BRTO, which was more reliable than direct endoscopy. Further, compared with X-rays (with iohexol added), BEVO provided a more detailed assessment of the distribution of sclerosant mixed with methylene blue. Both patients and doctors would be protected from radiation exposure. In addition, accumulated sclerosant was at high levels in EVs after balloon occlusion, which might be associated with no bleeding at the injection sites.
There are limitations of the present study. First, to minimize and avoid the risk of the balloon occlusion remaining in the esophagus for too long, the balloon was occluded for no more than 30 minutes at the most. As a result, this only initiated EV thrombus formation, but no inherent thrombosis has been formed immediately. Therefore, it was necessary to perform a Doppler EUS to determine the blood flow through the EVs. Further, the treatment would be conducted again if EVs remained present 1 week after the initial treatment. Second, a control group was not available. In the future, randomized controlled clinical trials are warranted for validation and to compare this technique with other treatments.
In conclusion, BEVO may be an effective and convenient option for F2 and F3 EVs. In addition to providing higher eradication rates, BEVO also reduced the occurrence of complications and recurrences.
Footnotes
Acknowledgment
The authors thank all the staff at the Department of Gastroenterology for their contribution to this work.
Informed Consent Statement
Informed written consent was obtained from patients before the publication of the present study and any accompanying images.
Authors' Contributions
Q.Z. and D.K. designed the study; Q.Z. and F.Z. collected and analyzed the patients' clinical data; J.J. and Z.Z. contributed to making the intraoperative recording; and D.K., J.-G.W., C.W., and X.M. contributed to carrying out the technique.
Disclosure Statement
No competing financial interests exist.
Funding Information
The present study was supported by the sixth batch of appropriate technology for the health promotion project of the Anhui Provincial Health Commission (SYJS202103).