
Abstract
Background:
This study aimed to clarify the safety and efficacy of laparoscopic surgery for colorectal perforation by comparing the clinical outcomes between laparoscopic and open emergency surgery for colorectal perforation.
Materials and Methods:
We retrospectively reviewed the data of 116 patients who underwent surgery for colorectal perforation. The patients were categorized into two groups: the open group included patients who underwent laparotomy, and the laparoscopic group included those who underwent laparoscopic surgery. Clinical and operative characteristics and postoperative outcomes were evaluated.
Results:
The open and laparoscopic groups included 67 and 49 patients, respectively. More than half of the patients in both groups developed perforation in the sigmoid colon (open, 58.2%; laparoscopic, 61.2%). The most common cause of perforation was diverticulum, followed by colorectal cancer. The mean intraoperative blood loss was significantly lower in the laparoscopic group than in the open group (70.0 mL versus 160.3 mL; P = .0290). The incidence of surgical site infection was lower in the laparoscopic group than in the open group (2.0% versus 13.4%; P = .0430). There were no significant differences in either the short- or long-term outcomes between the two groups. Univariate and multivariate analyses showed that the choice of surgical approach (open versus laparoscopic) did not affect overall survival in patients with colorectal perforation.
Conclusion:
The laparoscopic approach for colorectal perforation in an emergency setting can be safely performed and provides certain advantages over an open approach in suitable patients.
Introduction
In recent years, the usefulness and safety of laparoscopic surgery have been demonstrated in various abdominal surgical procedures, such as cholecystectomy, gastrectomy, and colectomy.1–6 Regarding colorectal diseases, several studies have compared open and laparoscopic surgery under various conditions, such as total colectomy for acute colitis, surgery for colorectal cancers, and colectomy for inflammatory bowel diseases.5–11 These studies suggest that the advantages of laparoscopic surgery include earlier recovery of bowel function, a lower incidence rate of postoperative complications, reduced pain scores, decreased estimated blood loss, and shorter hospital stay.6–9 However, there are few studies on the efficacy of laparoscopic surgery in an emergency setting.
A previous comparative study that examined the laparoscopic approach for emergency colorectal diseases was designed for patients with complicated diverticular disease, 12 and another study targeted patients who underwent colectomy regardless of the primary diagnosis. 13 However, data are limited, and the role of the laparoscopic approach under emergency conditions remains controversial. Furthermore, the studies included patients with various conditions, such as colorectal obstruction, hemorrhage, fistula, and perforation.12,13
Therefore, this study focused on colorectal perforation, which can lead to high morbidity and mortality and often causes generalized peritonitis and septic shock. We aimed to clarify the safety and efficacy of laparoscopic surgery for colorectal perforation by comparing the clinical outcomes between laparoscopic and open emergency surgery for colorectal perforation.
Materials and Methods
Patients
In this retrospective cohort study, we reviewed the data of 388 patients who underwent emergency surgery for abdominal perforation peritonitis at our single institute between August 2010 and April 2022. Emergency surgery was defined as the time from the diagnosis to surgery within 1 day. A total of 116 patients who underwent open or laparoscopic surgery and were diagnosed with colorectal perforation were eligible for analysis. A total of 272 patients diagnosed with upper gastrointestinal perforation, perforation of the jejunum and ileum, perforation of the appendix, or postoperative anastomotic leakage were excluded. Patients were categorized into the open and laparoscopic groups according to the surgical approach used. Cases in which the initial laparoscopic approach was converted to the open laparotomy approach, according to intraoperative judgment, were included in the open group.
Considering the comparison of the clinical features and operative outcomes between the two groups, the laboratory data were collected immediately before surgery. Surgical site infection was defined as the infection that occurred in the regions concerning the surgical procedure within 30 days after surgery. Ileus was diagnosed based on clinical symptoms such as cessation of passing gas and defecation, abdominal pain, and vomiting, and confirmed by the findings of intestinal dilatation and niveau on X-ray or computed tomography.
Moreover, 116 patients were categorized into the cancer group and noncancer group based on the presence of cancer lesions at the time of perforation. In each group, the above-mentioned analyses were performed.
Permission to perform this study was provided by the Institutional Review Board of the National Kyushu Medical Center (20C033). All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and the Declaration of Helsinki of 1964 and its later versions. Informed consent to be included in the study or equivalent was obtained from all patients.
Statistical analyses
Differences in characteristics between the groups were evaluated using Fisher's exact test or an unpaired t-test. Survival curves were plotted according to the Kaplan–Meier method, and differences were analyzed using a log-rank test. Univariate and multivariate analyses were performed using a Cox proportional hazards model to identify independent prognostic factors. All P-values were two-sided, and P < .05 was considered statistically significant. All analyses were performed using JMP PRO 11 software (SAS Institute Inc., https://www.jmp.com/ja_jp/home.html).
Results
Patient characteristics
Patients were categorized into two groups (67 patients in the open group and 49 in the laparoscopic group) according to the surgical approach used. Baseline demographic and clinical features of patients in the open and laparoscopic groups are summarized in Table 1. There were no significant differences in age, sex, location, and causes of perforation between the two groups. More than half of the patients in both groups developed perforation in the sigmoid colon (open, 58.2%; laparoscopic, 61.2%). The incidence of rectal perforation was higher in the laparoscopic group than in the open group (20.4% versus 15.0%). Diverticulum was the most frequent cause of perforation, with 28.4% in the open group and 30.6% in the laparoscopic group, followed by colorectal cancer, with 26.9% and 24.5% in the open and laparoscopic groups, respectively.
Baseline Demographic and Clinical Features of the Open and Laparoscopic Groups
Data are presented as n (%) unless otherwise stated.
A, ascending colon; C, Cecum; CRP, C-reactive protein; D, descending colon; R, rectum; S, sigmoid colon; T, transverse colon; WBC, white blood cell.
Operative outcomes
Operative outcomes were compared between the open and laparoscopic groups and are summarized in Table 2. There were no significant differences in the mean operative times between the two groups (open, 148 minutes versus laparoscopic, 156 minutes; P = .4719). The mean intraoperative blood loss was significantly lower in the laparoscopic group than in the open group (70.0 mL versus 160.3 mL; P = .0290). There were no significant differences in the occurrence of total postoperative complications between the two groups (open, 59.7% versus laparoscopic, 51.0%; P = .4990). Regarding postoperative complications, the occurrence of surgical site infection was higher in the open group than in the laparoscopic group (13.4% versus 2.0%, P = .0430). Regarding prognosis, there were no significant differences in mortality within 30 days after surgery, hospital mortality, and long-term survival between the two groups (Table 2).
Comparison of Operative Outcomes Between the Open and Laparoscopic Groups
Data are presented as the number (%) unless otherwise stated.
CD, Clavien–Dindo classification.
We assessed the operative outcomes by intention to treat, including the cases of conversions by intestinal dilatations or adhesions in the laparoscopic group; these results are summarized in Supplementary Table S1. This analysis demonstrated that intraoperative blood loss was significantly lower in the laparoscopic group, although cases of conversions were included in the laparoscopic group (P = .0330).
Postoperative survival
The Kaplan–Meier method was used to analyze the overall survival (OS) and to compare the postoperative prognosis between the open and laparoscopic groups (Fig. 1). Although the MSTs of the open and laparoscopic groups were 1313 and 653 days, respectively, 1-year OS rates were 61.5% and 68.3%, respectively. There were no significant differences in 1-year OS rates between the two groups (P = .5443). Comparing the prognosis according to the cause of perforation, patients with cancer at surgery had a significantly worse prognosis than patients with other diseases (1-year OS, 39.9% versus 73.9%; P = .0002) (Fig. 2). The survival data between open and laparoscopic surgery were compared for patients with cancer and those with other diseases. There were no significant differences in long-term survival rates between the two groups (Fig. 3).
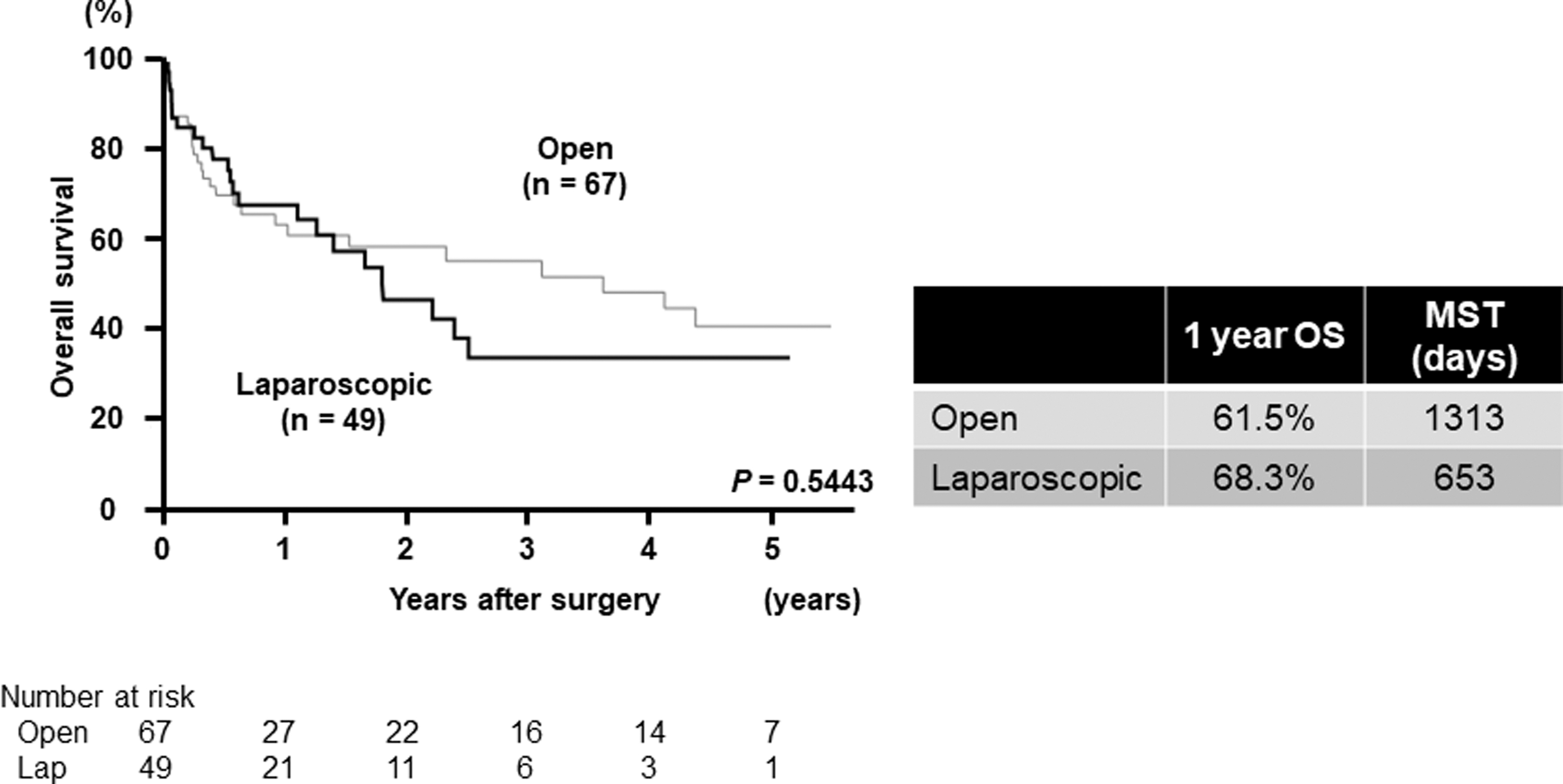
Postoperative survival in patients with colorectal perforation based on surgical approach, including a comparison between the Lap and open approaches. The 1-year OS rates and MST in the two groups are shown in the table. Lap, laparoscopic; MST, median survival time; OS, overall survival.

Postoperative survival in patients with colorectal perforation based on the causes of the perforation, including a comparison between cancer and other diseases. The 1-year OS rates and MST in the two groups are given in the table. MST, median survival time; OS, overall survival.
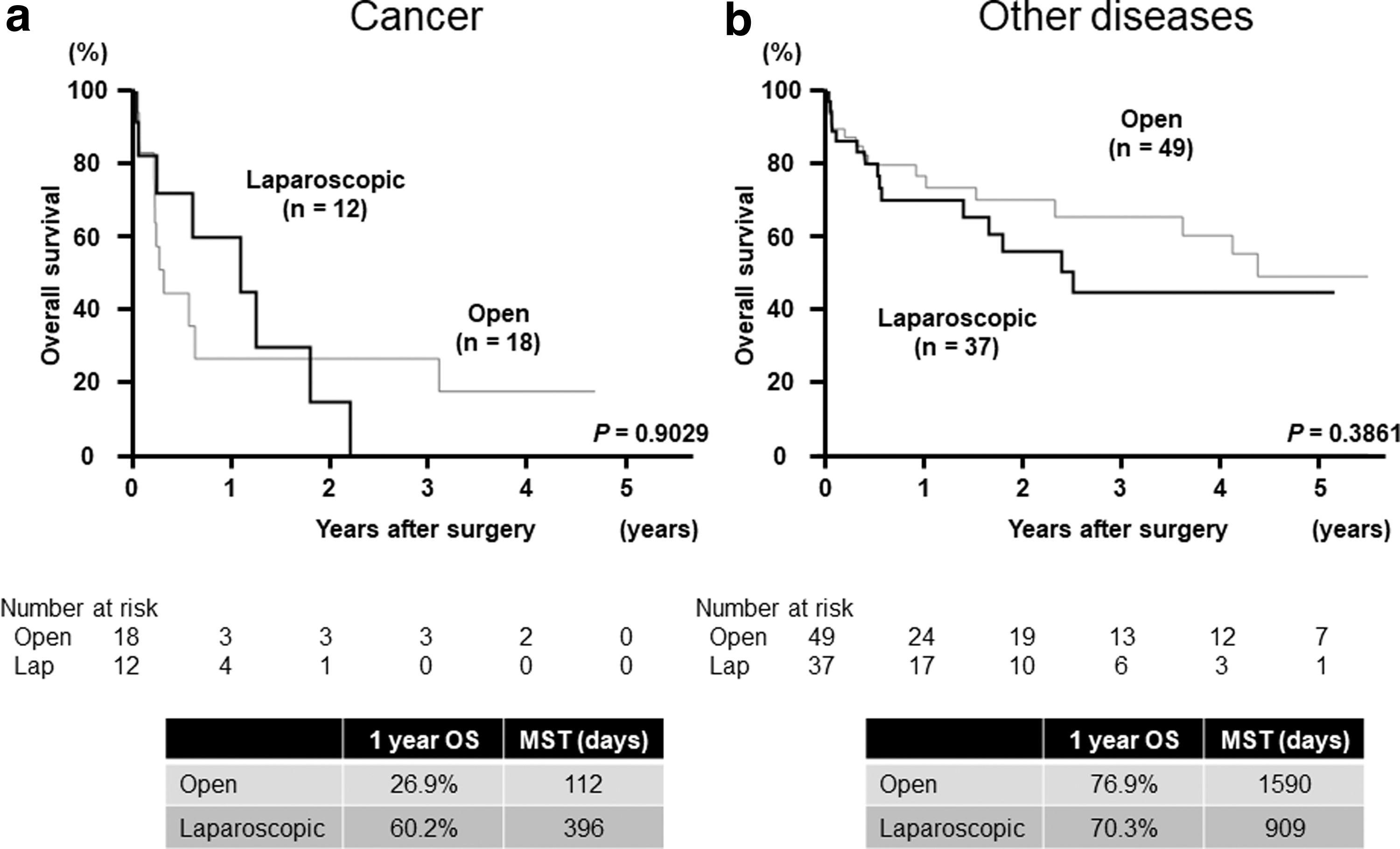
Postoperative survival in patients with colorectal perforation based on surgical approach, including a comparison between the Lap and open approaches after categorizing the patients into
Predictive factors for postoperative survival
Univariate and multivariate analyses showed that age ≥75 years old (versus age <75 years old) (P = .0347 and 0.0401, respectively), the occurrence of postoperative complications (P = .0040 and 0.0315, respectively) and cancer (versus other diseases) (P = .0008 and 0.0009, respectively) were independent predictive factors for poorer OS rates in patients with colorectal perforation. The surgical approach taken (open versus laparoscopic) was not associated with differences in OS rates in patients with colorectal perforation in both univariate and multivariate analyses (Table 3).
Univariate and Multivariate Analyses for Overall Mortality
CI, confidence interval; HR, hazard ratio.
Discussion
This study demonstrated that laparoscopic surgery for colorectal perforation was associated with a reduced amount of intraoperative blood loss. The operative outcomes indicated that the laparoscopic approach could be performed safely in emergency surgery for colorectal perforation with accurate decision-making regarding the indications.
Several studies have compared outcomes between open and laparoscopic approaches for various diseases and conditions.1–13 Siletz et al have suggested that laparoscopic surgery is associated with reduced complication rates, shorter operative times, shorter lengths of stay, and lower rates of discharge to skilled nursing facilities for various abdominal conditions, such as gastric perforation, small bowel disease, and ventral hernia. 14 Despite this, Cocorullo et al have indicated that, for the elderly population, there are no differences in operation times, morbidity rates, and mortality rates between patients undergoing open and laparoscopic approaches for abdominal emergencies, including gastroduodenal ulcer, small bowel disease, colonic acute disease, cholecystitis, and appendicitis. 15 Thus, these studies demonstrate that the laparoscopic approach can be safely performed even for emergency abdominal surgery.14,15
Focusing on the previous reports related to surgery for colorectal disease in the emergency setting, Turley et al compared laparoscopic and open Hartmann procedures for the emergency treatment of diverticulitis and demonstrated that the laparoscopic approach results in fewer overall complications and a shorter mean length of hospitalization; however, it does not decrease morbidity or mortality. 16 Koh et al compared the outcomes of laparoscopic colectomies with those of open colectomies under emergency conditions, such as colorectal bleeding, obstruction, and perforation, and demonstrated that the operative times in laparoscopic colectomies were longer than those in open colectomies, whereas the duration of hospitalization and postoperative morbidity between the two groups were similar. 13
Letarte et al compared the perioperative outcomes of laparoscopic colon resection and open colon resection for the treatment of complicated diverticular disease in the emergency setting, and they suggested that laparoscopic surgery was associated with decreased morbidity, intraoperative blood loss, time to oral intake, and length of hospital stay, whereas the mean operative time was longer than that of the open approach. 12
The above studies targeted colorectal disease with indications for emergency surgery, and they included various conditions, such as perforation, hemorrhage, and obstruction. The differences among these conditions are important and may substantially affect surgical procedures or perioperative outcomes. Of note, colorectal perforation has an extremely poor prognosis owing to generalized peritonitis and sepsis, and it often requires extensive drainage. Therefore, this study only focused on colorectal perforation. Most previous studies have demonstrated that the laparoscopic approach requires longer operative times,12,13 whereas our study showed that the mean operative times were not different between the open and laparoscopic groups. This finding might be related to the patients in our study, who had all received a diagnosis of colorectal perforation and were usually in poor general condition and required urgent surgery. Consequently, decisions to convert to open surgery for patients in whom it was difficult to complete laparoscopic surgery may have been made faster than for those with other diseases.
This study focused on the causes of colorectal perforation, that is, malignant or benign diseases, because they might affect the prognosis. Indeed, there were significant differences in the prognoses of patients with and without cancer. Moreover, in patients with cancer, progression of the primary cancer may be associated with their prognoses. In this study, both the cancer and other disease groups demonstrated no significant differences in OS rates between the open and laparoscopic approaches.
Other possible causes of perforation included ileus or steroids in several patients. When ileus occurs, the oral side of the colon is usually dilated, which could result in colorectal perforation by thinning of the intestinal wall or increase in the internal pressure. Moreover, steroids have broad anti-inflammatory properties by inhibiting prostaglandin synthesis, and they are known to contract vessels and inhibit tissue repair, increasing the risk of gastrointestinal perforation.
Moreover, in this study, cases in which the initial laparoscopic approach was converted to the open laparotomy approach were included in the open group. Our conclusions could be affected if the reason for conversion was bleeding. However, there were no cases in which the reason for conversion was bleeding. The reasons for conversion were intestinal dilatation and adhesion, and laparoscopy was used with the aim of only observation in the remaining cases. Therefore, most cases were converted to open procedure immediately; we considered that these cases should be regarded as the open group. Moreover, our analysis demonstrated that intraoperative blood loss was significantly lower in the laparoscopic group although cases of conversions by intestinal dilatations or adhesions were included in the laparoscopic group. These results strengthened our conclusion.
This study had a few limitations. A main limitation of our study was selection bias. The surgical procedure chosen, namely, an open or a laparoscopic approach, was dependent on each surgeon's decision. Consequently, surgeons who are proficient in laparoscopic surgery may tend to select the laparoscopic approach for wider indications, and choices of the surgeons may affect surgical and postoperative outcomes. In addition, this was a single-institution retrospective study that included a small sample size. Patients in this study were diagnosed with colorectal perforation and underwent emergency surgery; therefore, it was impossible to avoid selection bias or to design a prospective study. A comparison of the findings obtained from retrospective studies from various institutes would be meaningful. The findings from this study may provide useful information regarding the clinical value of the laparoscopic approach for colorectal perforation in an emergency setting.
The laparoscopic approach for colorectal perforation in an emergency setting is a safe procedure when conducted after careful patient selection, and it may decrease intraoperative blood loss and incidence of surgical site infection.
Footnotes
Acknowledgments
The authors thank the Kaibara Morikazu Medical Science Promotion Foundation, the Uehara Memorial Foundation, the Clinical Research Promotion Foundation and Fukuoka Public Health Promotion Organization Cancer Research Fund for financial support. The authors also thank Editage Group (![]() ) for editing the draft of this article.
) for editing the draft of this article.
Authors' Contributions
K.K. designed the study. K.K., E.K., H.H., Y.T., H.U., and R.Y. acquired the data. K.K., E.K., and Y.S. analyzed the data. K.K. performed statistical analyses. K.K. and T.K. drafted the article. T.K. and Y.S. revised the article critically for important intellectual content. T.K. and Y.S. approved the final version of the article. All authors have read and approved the article.
Consent to Participate
Written informed consent to be included in the study was obtained from participants, or the form of opt-out on the website was also used from participants who cannot obtain informed consent. Permission to perform this study was provided by the Institutional Review Board of the National Kyushu Medical Center (20C033). All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Declaration of Helsinki of 1964 and later versions.
Data Availability Statement
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Disclosure Statement
T.K., H.H., Y.T., E.K., H.U., R.Y., and Y.S. have no conflicts of interest or financial ties to disclose.
Funding Information
K.K. was supported by grants from the Kaibara Morikazu Medical Science Promotion Foundation in 2019, the Uehara Memorial Foundation in 2020, Grant of The Clinical Research Promotion Foundation in 2020 and Fukuoka Public Health Promotion Organization Cancer Research Fund in 2021.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.