
Abstract
Background:
Advancement in surgery has shifted numerous procedures to a same-day discharge (SDD) setting. In this study, we evaluated factors related to SDD after robotic transversus abdominis release (rTAR).
Materials and Methods:
A retrospective analysis of a prospectively maintained hernia databank was performed. Patients who underwent rTAR for incisional hernias were assigned to either the SDD group (length of stay [LOS] <1) or the inpatient group (LOS ≥1 day). Pre-, intra-, and postoperative variables were compared. Predictors of SDD were explored through a logistic regression, and a mediation analysis was performed to assess their effect on the LOS.
Results:
Out of the 167 patients included, 53 patients were discharged the same day. Age, American Society of Anesthesiologists score, history of coronary artery disease, and wound infection were significantly higher in the inpatient group. Overall, median LOS was 1 (0–2). Postoperative complications did not differ between SDD and inpatient groups except for Clavien–Dindo Grade-II (1 versus 14, respectively; P = .039). Thirty-day readmission rates were comparable (P = .229). A binary logistic regression to predict factors associated with SDD rTAR showed statistical significance in age, operative time, mesh area, and history of wound infection. Mediation analysis showed that mesh size indirectly affected the LOS through the operative time (a = 0.54; b = 0.46; P < .001). An age >46-year-old, an operative time beyond 217 minutes, and a mesh size >475 cm2 increased the probability of an inpatient stay (area-under-the-receiver operating characteristic curves: 0.69, 0.81, and 0.82, respectively).
Conclusion:
The pre- and intraoperative factors associated with SDD rTAR were age, history of wound infection, operative time, and mesh area. Further studies are needed to investigate the appropriateness of discharge decisions while balancing patients' benefits, resource utilization, and costs.
Introduction
With the goals of improving efficiency in hospital bed utilization and avoiding unnecessary hospital-acquired complications, surgeons have been shifting surgeries traditionally considered inpatient procedures to a same-day discharge (SDD) setting and developing enhanced recovery programs to expediate this. The COVID-19 pandemic has had a heavy impact on the health sector, accelerating the transition toward this new paradigm and the adoption of safe SDD procedures being favored across specialties.1,2
This shift includes minimally invasive hernia repair, which has been shown to reduce length of stay (LOS) without compromising repair safety and quality. Several studies have confirmed that minimally invasive hernia repairs can be performed as an SDD surgery.3–5 Although many open ventral and especially incisional hernia repairs would necessitate inpatient admission, robotic-assisted repair of these hernias has conferred a shorter LOS, particularly with the retromuscular approach. 6
This study sought to describe the outcomes of SDD robotic transversus abdominis release (rTAR) repairs and to determine variables with a potential predictive value.
Materials and Methods
Patient selection and study groups
A single-center single-surgeon retrospective review of a prospectively collected database of ventral hernia cases performed between February 2013 and March 2022 was performed. Patients who underwent rTAR repair for incisional hernias in an elective setting were included in the study, whereas primary ventral hernia repairs (VHRs) and emergent/urgent cases were excluded. Patients were then divided into two groups based on their hospital LOS, calculated as the duration between the date of the operation and the date of hospital discharge. The “SDD” group consisted of patients discharged on the same day of their operation and the “inpatient” group included patients who were admitted for an overnight or longer stay after their surgery.
Variables
Preoperative variables included patient demographics (age, gender, body mass index [BMI], comorbidities, and risk factors), the modified Ventral Hernia Working Group grade, and the hernia–patient–wound (HPW) stages. 7 The HPW grading system takes into account three different components: hernia width (three categories: H1 < 10 cm, H2 = 10–20 cm, H3 ≥ 20 cm), patient comorbidities (morbid obesity, immunosuppression, smoking, and/or diabetes), and wound status (clear or contaminated).
The operative variables included operative time, estimated blood loss (EBL), intraoperative incidences, hernia and procedure characteristics (laterality of the myofascial releasing, presence of hybrid rTAR approach [which involves a planned skin incision for defect closure and mesh deployment], and/or concomitant procedure, hernia size, hernia defect closure, and mesh type, size, and method of fixation). Postoperatively, pain was assessed using a Verbal Rating Scale from 0 to 10 in the postanesthesia care unit. Morphine milligram equivalent (MME) was also collected. Hospital readmission within a 30-day postoperative period and postoperative complications were also assessed.
Hernia dimensions were measured according to the European Hernia Society (EHS) recommendations. 8 Based on intraoperative measurements of hernia defects, as well as mesh dimensions, the variables of the hernia defect area, mesh area, and mesh-to-defect ratio were calculated using conventional mathematical formulas previously described in the literature. 9 Operative time was defined as the time between skin incision and closure (includes port placement, docking, and undocking).
Postoperative complications were retrieved from documented follow-up visits, patients' medical records, and clinical charts. All complications were categorized according to the Clavien–Dindo classification system. 10 The morbidity score was measured using the Comprehensive Complication Index (CCI®, University of Zurich, Zurich, Switzerland). 11 Surgical wound complications were categorized as follows: Surgical site events (SSEs) were defined as surgical site infections (SSIs) and surgical site occurrences (SSOs).
SSIs were further classified as cellulitis, superficial, deep, and organ space infections. SSOs included sterile fluid collections such as hematomas and seromas. Any SSOs or SSIs requiring procedural intervention such as percutaneous puncturing to reduce symptoms, bedside wound opening, or reoperation were described as an SSO/infection requiring procedural intervention.
Discharge instructions and follow-up
SDD regimen included pain and nausea medications (ondansetron, gabapentin, nonsteroidal anti-inflammatory drugs, narcotics, and stool softeners) and lifestyle modifications (avoidance of strenuous effort and low residue diet). Phone call follow-up was performed routinely by the staff the following morning. Routine follow-up was performed at regular intervals of 2–3 weeks, 3 months, semiannually, and annually.
Statistical analysis
Patient demographics, hernia characteristics, operative variables, and postoperative outcomes were compared between the two groups. Chi-square test or Fisher's exact test was used for categorical variables. Student's t-test or Mann–Whitney U test was used for continuous variables as appropriate. Categorical variables are presented in terms of frequency (n and/or %), whereas continuous variables were reported as the mean ± the standard deviation (SD) for normal distributions or the median with interquartile range (IQR) for non-normal distributions. A logistic regression analysis was run to determine the predictors for SDD.
Bivariate correlations were assessed using Pearson or Spearman correlation tests, as appropriate. A mediation analysis, which is a statistical method used to quantify the causal sequence, was conducted by using the PROCESS macro version 4 for SPSS that uses a regression-based approach to mediation and estimates path coefficients.12,13 Confidence intervals (CIs) were estimated using 10,000 replications and indirect effects were considered significant when the 95% bootstrapped CI did not contain 0. An alternative mediation model was also tested to exclude the presence of a spurious path effect in the hypothesized pathway. Statistical analysis was performed using the SPSS software (Statistical Package for Social Sciences for Windows Version 22). A P < .05 was considered statistically significant.
Results
In total, 167 patients were included in the study. The median (IQR) LOS was 1 (0–2) day for the entire cohort (maximum LOS of 14 days). Of those, 53 (31.7%) patients were discharged on the same day of the operation.
A comparison of patient demographics between the two groups is given in Table 1. In terms of laterality, 31 (58.5%) patients in the SDD group underwent a unilateral TAR, whereas 96 (84.2%) patients in the inpatient group underwent a bilateral TAR (P < .001). The rate of hybrid procedures was significantly higher in the inpatient group than in the SDD group (P < .001; 25.4% versus 1.9%, respectively). The rate of concomitant procedures did not differ between the SDD and inpatient groups (P = .369, 28.3% and 21.9%, respectively).
Comparison of Patient Demographics Between the Two Groups
Values in bold represent a P value < 0.05.
ASA, American Society of Anesthesiologists; BMI, body mass index; CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; DM, diabetes mellitus; HT, hypertension; IQR, interquartile range; MI, myocardial infarction; SD, standard deviation.
No differences were found between SDD and inpatient rTAR rates before and after the COVID-19 outbreak (P = .631). Also, SDD rates did not show a significant difference between the learning curve phases of rTAR, which were defined in a previously conducted study (P = .689). 14
A comparison of hernia characteristics and operative variables of the two groups is given in Table 2. Mesh area was significantly larger in the inpatient group than in the SDD group, also corresponding with a larger hernia defect area. Consequently, the mesh-to-defect ratio was higher in the SDD group. There were no significant differences in mesh material used between the two groups (P = .135). The rate of mesh fixation was 30.2% in the SDD group versus 16.7% in the inpatient group (P = .065). Operative time was significantly longer in the inpatient group. None of the procedures were converted to conventional open or laparoscopic approaches.
Comparison of Hernia Characteristics and Operative Variables Between the Two Groups
Values in bold represent a P value < 0.05.
EBL, estimated blood loss; HPW, hernia–patient–wound; IQR, interquartile range; LOA, lysis of adhesions; rTAR, robotic transversus abdominis release; SD, standard deviation; VHWG, Ventral Hernia Working Group.
An intraoperative complication occurred in 9 (5.4%) patients in the entire cohort, all of whom were in the inpatient group (P = .059). There were no differences between the two groups in terms of median (IQR) postoperative pain scores, and MME (median [IQR] pain score: SDD 5 [4–7] versus inpatient 5 [3–6]; median [IQR] MME: SDD 12.5 [7.5–20] versus inpatient 11.7 [5–17.5]; P = .206 and P = .421, respectively).
Thirty-day readmission rates did not differ between SDD and inpatient groups (P = .229; 3.8% versus 10.5%, respectively). The distribution of postoperative complications between the two groups is presented in Table 3. The rate of Clavien–Dindo grade-II complications and median (IQR) CCI scores were significantly higher in the inpatient group. Mean ± SD follow-up periods did not differ between the two groups (P = .957; 27.8 ± 17 months in the SDD group versus 28.7 ± 19 months in the inpatient group).
The Comparison of Postoperative Outcomes
Values in bold represent a P value < 0.05.
CCI, Comprehensive Complication Index (University of Zurich, Zurich, Switzerland); rTAR, robotic transversus abdominis release; SSEs, surgical site events; SSIs, surgical site infections; SSOs, surgical site occurrences; SSO/I-PI, surgical site occurrence or infection requiring procedural intervention.
A binary logistic regression analysis using statistically significant and/or clinically relevant variables to predict factors associated with SDD rTAR resulted in a best fit logistic regression model showing statistical significance in age, operative, mesh area, and history of wound infection (Table 4). Correlations were found between the continuous variables (Table 5).
Binary Logistic Regression Model Assessing the Likelihood of Being Discharged at the Same Day of Robotic Transversus Abdominis Release Procedure
Values in bold represent a P value < 0.05.
TAR, transversus abdominis release.
Correlations Between the Continuous Variables
Values in bold represent a P value < 0.05.
LOS, length of stay.
Afterward, a mediation analysis was performed to see whether mesh area affects the hospital LOS through its effect on operative time, after obtaining appropriate results from assumption tests (linearity and homoscedasticity). Results from a simple mediation analysis (corrected for age and history of wound infection) indicated that mesh size was indirectly related to LOS through its relationship with operative time. As shown in Figure 1, mesh size first correlated with operative time (a = 0.54; P < .001), and subsequently longer operating time was related to a longer LOS (b = 0.46; P < .001).
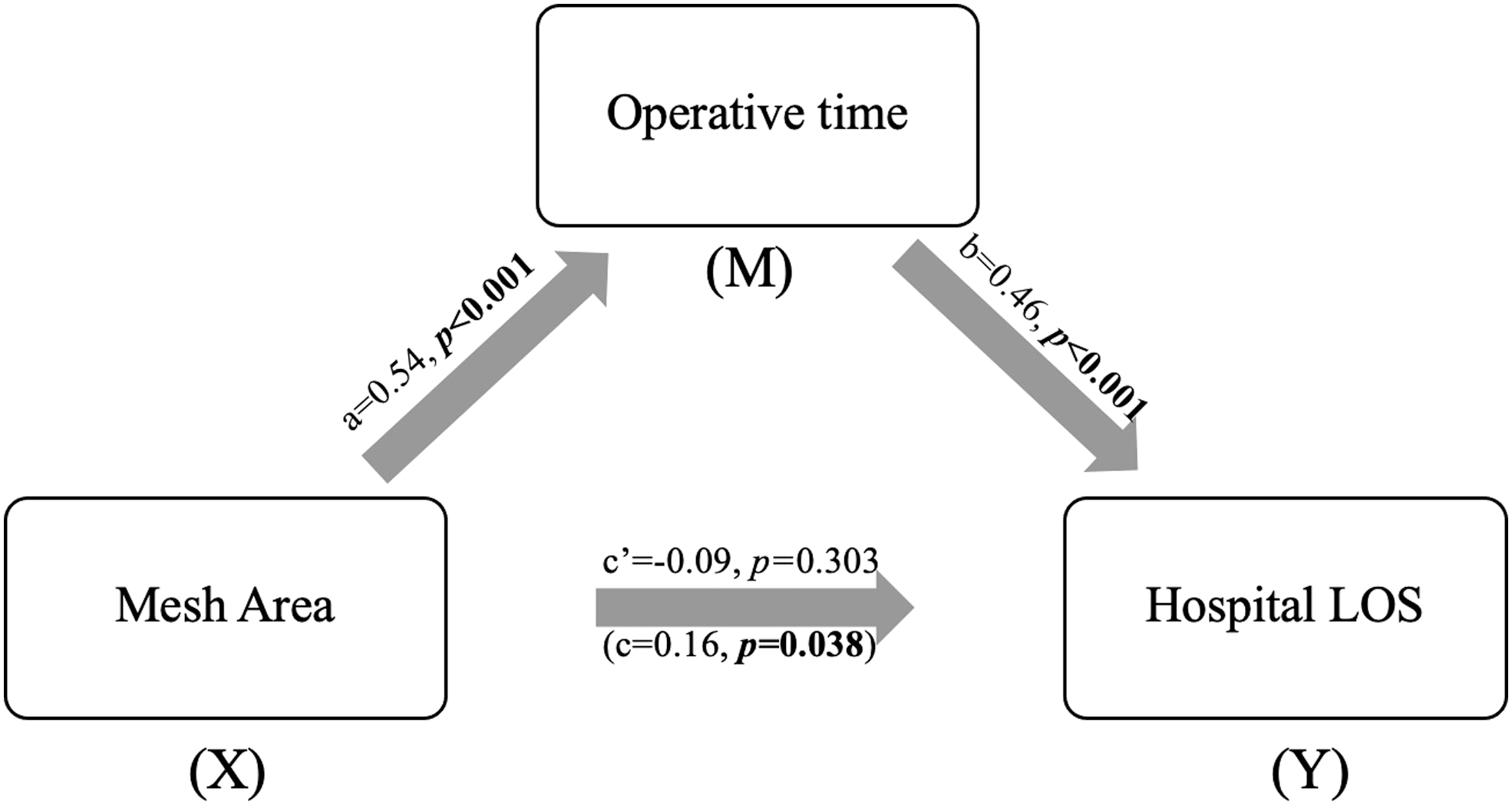
The mediating effect of operative time in the relationship between mesh area and the hospital LOS. All presented effects are standardized; a is effect of mesh area on operative time, b is effect of operative time on the hospital LOS, c’ is direct effect of mesh area on the hospital LOS, c is total effect of mesh area on the hospital LOS. LOS, length of stay.
Since the 95% bias-corrected CI of ([0.10–0.37) based on 10,000 bootstrap sample did not include 0, the indirect pathway (ab = 0.25) was statistically significant. Furthermore, an ROC curve analysis to find cutoff values for continuous variables showed that an age >46 years old, an operative time beyond 217 minutes, and a mesh size >475 cm2 increased the probability of an inpatient stay (area under the ROC curves: 0.69, 0.81, and 0.82, respectively).
Discussion
To our knowledge, this is the first study to evaluate SDD after rTAR and to define the factors influencing its associated hospital LOS. In general, reduced postoperative LOS is an advantage of minimally invasive surgery, and SDD robotic approaches are feasible in selected patients for certain procedures.15,16
When compared with open retromuscular VHR, robotic retromuscular VHR has reduced hospital LOS, with comparable outcomes. 6 Studies in the literature report a mean hospital length of stay of two days for robotic TAR.6,17 Several factors related to the patient, the procedure, and the immediate postoperative course could potentially impact the hospital LOS. In our study, medial history, such as age, history of wound infection, and of coronary artery disease affected the LOS. Intraoperative complications occurred only in the inpatient group, with no complications in the SDD group.
This finding is of minimal clinical relevance as we believe surgeons would not discharge their patients immediately after the surgery if an intraoperative complication occurred. Also, concomitant repairs, with a rate comparable between the two study groups, did not seem to influence the LOS in this study. Our cohort consisted only of robotic repairs, and postoperative pain did not differ between the inpatient and SDD groups. In terms of clinical outcomes and postoperative complications, patients who were discharged on the same day of their surgery did not suffer from increased complications, and thus the decision for an early discharge did not affect their postoperative course.
The concept of SDD of incisional hernia repair is not a recent one and dates to the early 2000s when Moreno-Egea et al. reported their experience with 55 SDD laparoscopic incisional/VHRs. In their study, 42 patients out of the 55 were discharged on the same day. Out of the 13 patients who required admission immediately after their surgery, 5 had intraoperative complications, 4 underwent concomitant procedures, and 4 were admitted for pain. The authors reported no SSIs or 30-day readmissions, and only one recurrence postoperatively. 18
Carbonell et al. 6 compared open versus robotic retromuscular VHR. The robotic arm included a total of 111 patients, out of which 80% underwent a TAR. The authors reported a median LOS of 2 days for the robotic arm, with no SDDs and 56 discharges on postoperative day 1. Two intraoperative complications occurred. The SSI rate reported was at 2% and 30-day readmission at 6%.
In general, a decreased LOS likely could reflect a decrease in perioperative pain associated with the robotic approach. 19 Carbonell et al. 6 reported reduced pain as one of the possible factors associated with reduced LOS in open versus robotic retromuscular VHR, with a multitude of components contributing to this finding. Smaller incisions, decreased traction on the abdominal wall, and mesh fixation with sutures instead of transfascial fixation may all be factors contributing to reduced pain. However, this finding was observed when comparing open versus robotic approach, which is not the case in our study.
Leonard et al. 20 investigated risk factors associated with prolonged LOS after laparoscopic VHR. They reported a median LOS of 2 days. A univariate analysis showed that operative time, mesh size, narcotics dose, and female gender were associated with prolonged LOS. Similarly, we found that operative time and mesh size are independent predictors of hospital LOS. However, no association between increased LOS and both the MME and gender was found in our study. Furthermore, when we performed a mediation analysis, mesh area indirectly affected the hospital LOS through the increased operative time.
Hernia complexity inherently plays an important role in the difficulty of the defect repair. Several studies found the complexity of the hernia to be associated with a longer LOS in laparoscopic VHR.21,22 Although the HPW staging system was introduced to predict both short-term wound morbidity (SSE) and long-term efficacy (recurrence), a strong association between HPW and increased LOS was found in this study. Thus, patient and wound characteristics should be considerable components in hernia complexity. Interestingly, our study showed that a history of wound infection was found to be an independent predictor for increased LOS.
Mesh area was substituted for hernia dimension in the best-fitting logistic regression model, even though hernia dimension was a predictor in the multiple regression analysis. Other potential risk factors such as hybrid procedures, as seen in this study, and EBL may also prolong LOS—these cannot be accounted for using traditional complexity scoring systems and may have an important role in predicting inpatient versus SDD robotic procedures.
A recently published study by Dyas et al. 23 discussed a validation of a prediction model for conversion of SDD to inpatient surgery. The SURPAS (Surgical Risk Preoperative Assessment System) uses eight preoperative variables, of which four are related to the procedure itself (Current Procedural Terminology [CPT], specific event rate as calculated from the ACS-NSQIP database, work relative value unit of the CPT code of the primary operation, specialty of the primary surgeon, and inpatient/SDD setting of the operation), and four related to the patient (American Society of Anesthesiologists class, age, emergency status, and functional health status [independent, partially dependent, and fully dependent]).
The model accurately predicted patient risk of unplanned immediate postoperative admission. With the COVID-19 pandemic draining the health care sector on all levels, such prediction models were of ultimate need to avoid unnecessary inpatient admissions and hospital overload. However, a comparison of pre- versus post-COVID-19 outbreak in this study did not show significant difference between SDD rates for rTAR. This leads the discussion to an important factor, which is the surgeon's decision-making process.
Although the results of this study show the importance of procedure-related factors, several preoperative questions ought to be asked. Before deciding on the surgery setting, surgeons should assess the patient's capacity of undergoing a same-day surgery. The surgeon should consider patient's ability to tolerate pain, psychological support, and baseline level of independence, and ensure that postoperative expectations are clearly understood.
This study has some limitations. First, this is a retrospective study evaluating rTAR repairs performed at a single center. Judgment of the surgical team constitutes a cornerstone in the decision on patient's readiness for discharge and needs to be evaluated across multiple centers to minimize its bias. Second, important sociocultural factors were not included in the analysis, such as the dependency level and cultural beliefs of the patient, as both components could either prolong or shorten the LOS. Finally, patient-reported outcomes are needed to evaluate the satisfaction and quality of life after SDD surgery. With the goal of elucidating helpful factors for the decision, future studies should focus on the conversion rate from the outpatient to the inpatient setting, and vice versa, to further concretize our findings.
Conclusion
In our cohort of patients undergoing rTAR, we found that preoperatively, age and history of wound infection impacted the decision for SDD, whereas operative time and mesh area were the predictive intraoperative factors. Further studies are needed to investigate the appropriateness of discharge decisions while balancing the benefits to the patients, resource utilization, and costs.
Footnotes
Authors' Contributions
O.Y.K. contributed to conceptualization, writing—review and editing, and supervision. G.K. was involved in software, data curation, writing—original draft, writing—review and editing, and visualization. N.B.-A. carried out data curation and writing—review and editing. K.V. took charge of writing—review and editing. F.G. was in charge of conceptualization, methodology, software, formal analysis, writing—review and editing, and visualization.
Ethical Approval
The database used for this study was approved by the institutional review board (IRB No. HW202).
Human and Animal Rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Disclosure Statement
G.K., N.B.-A., K.V., and F.G. have no conflicts of interest or financial ties to disclose. O.Y.K. has received teaching course, grant funding, and/or consultancy fees from Intuitive Surgical, Bard, and W.L. Gore outside the submitted study.
Funding Information
No funding was received for this article.