
Abstract
Background:
For children with congenital lung malformations (CLMs), there is insufficient evidence of the efficacy of direct visual paravertebral block (PVB). We aimed to evaluate its effectiveness and safety by comparing it with local anesthetic infiltration (LAI).
Materials and Methods:
This was a nonrandomized control study of CLMs in children younger than 3 years of age who underwent thoracoscopic surgery in our hospital from January to December 2020. The children were divided into group A (PVB analgesia group) and group B (LAI group). The primary outcome was the incidence of rebound pain within 72 hours. Secondary outcomes included the Face, Legs, Activity, Crying, Consolability (FLACC) pain scores at 0, 6, 12, 24, 36, 48, and 72 hours, side effects, adverse events, the number of rebound pains, and the postoperative family observation scores.
Results:
The incidence of rebound pain was 10% in group A and 60.5% in group B within 72 hours (P < .001). The PVB was associated with decreased FLACC pain scores at 12, 24, 36, 48, and 72 hours, family observation scores, and the number of rebound pains (P < .001, P = .01, P = .028, P = .005, P = .006, P = .026, and P < .001, respectively). Group B was also associated with a higher rate of side effects and adverse events. There was no difference in the length of hospital stay.
Conclusion:
The PVB under direct vision analgesia technique is effective and safe for postoperative pain control in pediatric patients with CLMs. It may be an attractive alternative to LAI for pediatric thoracoscopic surgical procedures.
Introduction
Congenital lung malformations (CLMs) are a rare developmental anomaly of the lower respiratory tract 1 but are detected more frequently due to improvements in prenatal examinations. CLMs are usually treated with the thoracoscopic surgical procedure, which is safe and feasible. 2 However, thoracoscopic surgery is an invasive procedure, and postoperative pain stress remains, especially for pediatric patients who cannot accurately complain of pain.3,4 Therefore, postoperative pain control in pediatric patients is integral to rehabilitation. 5 However, nearly 80% of patients reported experiencing postoperative pain, 6 and 80% reported moderate to severe pain. 7
In addition, pain control is less performed in children due to restrictions on the use of analgesic medications or excessive concerns about the side effects of medications.8,9 Poor pain control was associated with severe painful experiences for patients, leading to pulmonary atelectasis and worsening respiratory function. As a result, it can lead to increased hospital stays, poorer quality of life, and immunosuppression due to prolonged stress.10,11
Local anesthetic infiltration (LAI) is commonly used for postsurgical analgesia and is simple, effective, and inexpensive. LAI prevents the introduction of noxious peripheral stimuli. 8 It has been shown to reduce postoperative pain and accelerate recovery of regular activity in pediatric patients.12,13 However, LAI is associated with the limitation of the restricted duration of action and less potent analgesia compared with neuraxial or peripheral nerve blocks. Other regional techniques providing prolonged analgesia in children include continuous intercostal nerve block, thoracic extradural, and intrapleural catheter insertion. All of them have the limitations of either technical difficulty or unreliable efficacy. The paravertebral block (PVB) under direct vision is another promising postoperative analgesia technique that targets major nerve branches directly. PVB under direct vision for thoracoscopic surgical procedures may offer some benefits and provide prolonged postoperative analgesia without increasing complications compared to LAI.
However, PVB under direct vision is an anesthetic technique not commonly used for patients with CLMs. It is unclear whether any of these techniques is superior according to uniform outcome assessment. Therefore, we conducted a nonrandomized controlled trial to compare PVB under direct vision with LAI for thoracoscopic surgical procedures.
Materials and Methods
We conducted a single-center, single-blinded, nonrandomized, controlled study to determine the effect of the PVB with video assistance in comparison with the LAI on reducing postoperative pain in CLMs children who underwent thoracoscopic surgery. The Institutional Research Board of Sichuan University West China Hospital approved this study (trial [941] in 2020). Consent was obtained from each patient's legal guardian.
Participants, treatment allocation, and blinding
CLMs patients younger than 3 years of age with no contraindications to surgery who were scheduled to undergo thoracoscopic surgical procedures from January 2020 to December 2020 were approached for inclusion. Exclusion criteria included the following: parental guardian refusal; participation in other clinical studies; other underlying diseases (heart, liver, kidney, cardiovascular and cerebrovascular, and other underlying severe diseases); combined psychiatric and central nervous system diseases; and conversion to thoracotomy. Patients were divided into group A (the PVB analgesia group) and group B (the LAI analgesia group) based on whether the surgery was performed in the first 6 months of the study. The study data were collected by the researchers blinded to the group allocation. The surgeon, regional pediatric anesthesiologist, and operating room staff were not blinded to the treatment group. However, the patients, their caregivers, and ward nurses who collected the data from families were blinded.
Interventions
The same team of surgeons enrolled their patients in the study and performed lobectomy or segmental lung resection. Patients were nonrandomized to one of the following two groups using equivalent, volume-adjusted doses of ropivacaine hydrochloride: (1) LAI injected at the incision site (2) PVB performed under direct vision at the end of the operation.
Anesthetic technique
Patients received no acetaminophen or midazolam before surgery. Anesthesia was induced via a mask using inhalational anesthetics and oxygen. After peripheral intravenous placement, general anesthesia was maintained via laryngeal mask airway or endotracheal tube, depending on the intraoperative anesthesiologist's preference. At the end of the surgery, for group A, a stimulation needle for single-shot technique in peripheral regional anesthesia was advanced under direct vision of thoracoscopy through the port site at the level of the fourth to fifth rib by thoracic surgical team before closing the trocar port sites. Ropivacaine of 0.2% (0.2 mL/kg) was injected after confirming no blood return in the needle. The procedure was completed by retiring the needle after the drug had spread in the paravertebral space.
In addition, observing the injection sites for 5 minutes is needed to determine whether a hematoma has developed. For group B, a single shot of 0.2% ropivacaine (0.2 mL/kg) was injected directly into the subcutaneous tissue of portal sites at the end of surgery. No self-control analgesia pump was used in either group of children postoperatively. Both groups of children's Analgesic drugs were 0.2% ropivacaine and 5 μg/mL epinephrine of epinephrine for a total dose of no more than 4 mg/kg.
Postoperative management
Both groups received standard postoperative management, including cefuroxime sodium (30 mg/kg ivgtt Q8h) to prevent infection and acetylcysteine solution (3 mL inh bid) to aid airway clearance. Ibuprofen (5 mg/kg/po 4–6 h/T) is used for postoperative rebound pain in children. The postoperative temperature of the children was 37.5°C–38.5°C, considering the physical cooling method. If the temperature exceeded 38.5°C, ibuprofen (5 mg/kg/dose po 4–6 h/T) was used to treat the fever as required. The children's condition was observed 72 hours after surgery, and symptoms such as fever, vomiting, abdominal distension, and temperature abnormalities (≥ 38.5°C) were recorded in detail. The number of children with symptoms was counted, and the children who experienced any abnormal changes in condition after surgery were counted. We also recorded the total length of stay and postoperative length of the children.
Face, legs, activity, crying, and consolability scale
In this study, the Face, Legs, Activity, Crying, and Consolability (FLACC) scale, valid for patients younger than the age of 3 years, 14 was chosen to assess postoperative pain. Before the study, the nursing staff was trained in using the FLACC scale. The scale consisted of five components, namely expression, behavior, physical movement, comfortability, and crying, each of which was scored 0–2 out of 10 (0 = relaxed and comfortable; 1–3 = mild discomfort; 4–6 = moderate pain; 7–10 = severe pain, discomfort, or both). 15 We conducted pre-experiments and a survey of health care professionals before the study began. Combine these two results and select T1, T2, T3, T4, T5, T6, and T7 for accurate postoperative pain assessment. We also recorded postoperative rebound pain after surgery, including the number and frequency of patients' rebound pain due to inadequate analgesia.
Parents' postoperative pain observation and satisfaction questionnaire
In this study, we also evaluated parental records of the patient's postoperative pain. A pilot survey of parents of children who underwent CLMs surgery revealed that the parents believed that their children were affected in three areas before and after surgery: daily life, sleep, and mood. So the study used a self-designed questionnaire consisting of daily life, sleep, and mood, scoring 1–5 out of 15. In addition, we added satisfaction to this questionnaire, including the analgesic effect and recovery of the child.
Statistical analysis
Normally distributed continuous data are presented as the means ± standard deviations; skewed continuous data are presented as medians (interquartile range). The Kolmogorov–Smirnov test was used to test distribution. Continuous data between two groups conforming to a normal distribution were analyzed by t-test, while they were not analyzed by Mann–Whitney U test. Categorical data were presented as proportions and were tested by the χ 2 test or Fisher's exact test as appropriate. Repeated numerical data of postoperative FLACC scale scores at different time points were analyzed using repeated-measures analysis of variance. All data were analyzed with SPSS software (version 28.0, IBM, Armonk, NY, USA), and P < .05 was used to determine statistical significance.
Results
Demographic and surgical characteristics
Ninety-eight children and their parents who met the study criteria completed the questionnaires during the study period. Sixty patients with a median age of 8 months were nonrandomly assigned to group A, and 38 patients with a median age of 7 months were assigned to group B. All patients experienced an uneventful procedure, and conversion to thoracotomy and transfusion were not needed. In addition, none of the patients in group A developed a visible hematoma during the surgery. There was no significant difference in the demographic characteristics and basic surgical information between the two groups of children (P > .05) and their parents (P > .05) in Table 1.
Demographic Characteristics of the Children and Basic Surgical Information
BMI, bogy mass index.
Postoperative rebound pain
Postoperative rebound pain occurred in 6 patients (10%) in group A and 23 patients (60.5%) in group B (P < .05). Meanwhile, the number of postoperative analgesics used in group A was significantly lower than that in group B (P < .05), as shown in Table 2.
Comparison of Rebound Pain Results Between the Two Groups
Postoperative pain scores at different time points
Group A had significantly lower pain scores than group B (F = 54.593, P < .01), and the pain scores decreased gradually with time (Fig. 1). Both groups had the highest pain scores at T2 (6 hours postoperatively). There was a significant difference in pain scores at T3, T4, T5, T6, and T7 postoperatively between the two groups (P < .05), while there was no significant change at T1 and T2 (P > .05), as shown in Table 3.
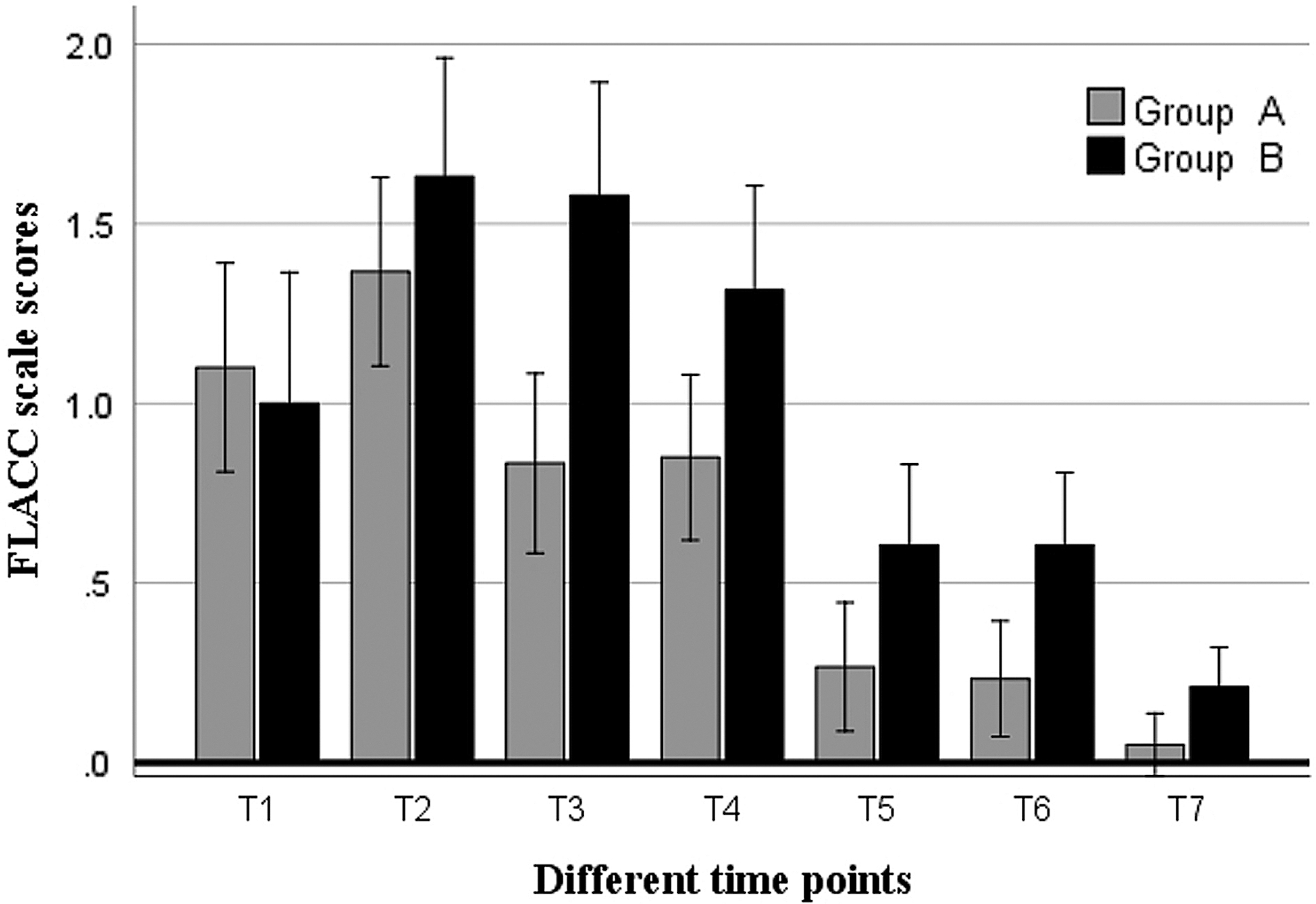
Graphic representation of FLACC Scale pain scores at each postoperative time point for PVB (gray bars) and LAI (black bars). There was a statistically significant difference in favor of the PVB at the T3 (P < .001), T4 (P = .014), T5 (P = .021), T6 (P = .005), and T7 (P = .025) postoperative time points. FLACC, Face, Legs, Activity, Crying, and Consolability; LAI, local anesthetic infiltration; PVB, paravertebral block.
Comparison of Pain Scores Between the Two Groups of Patients
Parents' postoperative pain observation and satisfaction questionnaire
The parents' postoperative pain observation scores in group A were significantly lower in all dimensions than in group A. Patients in the two groups showed a significant difference in parents' postoperative pain observation scores in their daily life dimension (P < .05). At the same time, there was little change in mood and sleep dimensions (P > .05). The total parents' postoperative pain observation score was more variable in group A than in group B (P < .05). The two groups showed no difference in the satisfaction results, as shown in Table 4.
Comparison of Parents' Postoperative Pain Observation and Satisfaction Scores Between the Two Groups
Postoperative outcome
There was no significant difference in the incidence rate of vomiting, abdominal distension, subcutaneous emphysema, fever, or pneumothorax between the two groups. Moreover, although a total of 32 cases (53.3%) and 29 cases (76.3%) occurred with postoperative complications in the two groups, respectively, which was statistically significant (P = .032), the postoperative length of stay and total length of stay between groups were comparable. As shown in Table 5.
Comparison of Postoperative Variables Between Two Groups
Discussion
To our knowledge, this is the first nonrandomized controlled study to compare outcomes of PVB under direct vision with LAI for pediatric thoracoscopic surgical procedures. Our results demonstrate that PVB under direct vision is a promising regional anesthesia technique in terms of analgesic efficacy and safety compared to LAI. PVB prolonged postoperative analgesia improved the analgesia effect and has not increased complications.
All PVB in our study was performed by the same surgeon under direct vision of thoracoscopy, which is vital in the current climate of increased use of minimally invasive thoracic surgery and enhanced recovery after surgery. Currently, thoracoscopic surgery treats more than 20 pediatric diseases 2 and thus increases the feasibility of conducting PVB under direct vision with the possibility of decreased vascular puncture and spinal nerve injury. Continuous extrapleural paravertebral infusion of local anesthetics under direct vision has been used extensively in pediatric children to provide safe and effective post-thoracotomy analgesia. A single shot of ropivacaine immediately before trocar port closure was used in our study, which simplified the PVB technique.
Clinical treatment of CLMs mainly relies on surgical resection of lobes or segments of the lung, and many of them receive surgery at 6–12 months. We chose CLMs because of the relatively homogenized participants and because postoperative pain management in pediatric patients is urgently needed for evaluation.
Pediatric postoperative pain assessment and management is challenging because some children, especially infants, cannot adequately complain of pain. 16 The pain may be caused by traction at the incision site, removal of the ribs, intercostal nerve injury due to dislocation of the cribriform joints, irritation of the pleura by the thoracic duct, and hyperextension of the ipsilateral brachial plexus and associated shoulder muscles. 17 However, the continuity of pain expression within the pediatric age range has been well described. Infants may cry violently, be stiff, have poor oral intake, and be ornery. Children may push away stimuli, protect painful body parts, cry violently, or exhibit regressive behavior. Considering that most children receiving CLMs surgery were younger than 3 years of age, the FLACC scale had the highest clinical utility score, followed by NAP. 18 Consequently, the FLACC scale was chosen for this study to assess postoperative children.
In this study, we found that the incidence and frequency of the postoperative FLACC pain scores and rebound pains were significantly lower than LAI. This may be attributed to the enhanced analgesic efficacy of PVB. In particular, FLACC pain scores were significantly different between the two groups more than 12 hours after surgery. This is in line with a previous study that showed that in thoracoscopic surgery, postoperative analgesia for a single PVB could last between 6 and 48 hours. Zhang 19 and Syal 20 also reported that the PVB group had lower postoperative pain scores at 12–72 hours.
However, there was no statistically significant difference between the two groups for postoperative pain scores from 0 to 6 hours. The children may have had more residual anesthetic drugs in their bodies during this period, and their somatic sensations had not fully recovered, so there was no significant difference in pain scores between the two groups.
Family members are in close contact with the child and are often the critical factor in the child's postoperative pain control.21,22 Therefore, parents need to assess their child's pain. The total score of the PVB group family pain observation was significantly lower than that of the LAI group, which was consistent with that of children, suggesting indirectly that PVB analgesia is better than local infiltration. However, there was no difference in the postoperative mood and sleep scores between the two groups, with both groups scoring lower.
However, there was a significant difference in daily activities, and both groups scored higher. Changes in daily activities were mainly due to a decrease in children's voluntary activities after surgery compared to presurgery, such as a decrease in children's reluctance to roll over and limb extension. This indicated that the pain had a more significant impact on the child's daily activities, but less on the child's mood changes and sleep.
The PVB group had comparable postoperative complications with the LAI group, and there was no significant difference in the incidence of single abnormal body temperature, vomiting, or abdominal distension. Patients in both groups had a similar postoperative length. They recovered smoothly, suggesting that PVB has not increased the incidence of postoperative complications and that PVB techniques were feasible in pediatric thoracoscopic surgery.
There are several limitations. First, this was a single-blind nonrandom study, and a blank control group was not included in this study concerning postoperative pain. Only PVB analgesia and wound infiltration analgesia were compared. Since none of the analgesic techniques may achieve the analgesic effect, in theory, combining multiple analgesic technologies may further enhance the analgesic effect, and further studies are needed. Second, postactivity pain was not assessed because many of these patients were younger than 1 year old. We only considered three general items in family pain observation without further refinement analysis, such as daily activities in eating and independent activities refinement. Thus, the analgesic effect requires further study.
In conclusion, our study suggests that PVB under direct vision is effective and safe postoperative analgesia in thoracoscopic surgery and is associated with improved and prolonged analgesia compared with LAI. However, larger studies are needed to assess the efficacy of these approaches.
Footnotes
Authors' Contributions
M.J. and W.H. have contributed substantially to the conception or the design of the article, and Y.Y. and Y.L. the data acquisition, analysis, and interpretation. C.L., L.W., and T.L. designed data collection instruments, collected data, conducted preliminary analysis, and reviewed articles. C.X. conceptualized and designed the study, coordinated and supervised data collection, and critically reviewed the article for important intellectual content. All authors read and approved the final version of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.