
Abstract
Purpose:
Endoscopic sphincterotomy (EPT) combined with endoscopic papillary large balloon dilatation (EPBD) are used to remove large common bile duct (CBD) stones. This meta-analysis compared the efficacy and safety of EPT+EPBD versus EPT alone in the removal of stones based on stone size.
Materials and Methods:
Twenty-two studies (11 randomized control trials [RCTs] and 11 non-RCTs) were identified and reviewed based on searches of Embase, PubMed, and Web of Science. CBD stone's size was measured with reference to diameter of the duodenoscope (13 mm) and size of the large dilatation balloon (17 mm) seen on cholangiogram. The stone clearance rate, required mechanical lithotripsy (ML), procedure time, and pancreatitis were compared according to the mean stone size, and further divided into Groups A (small) 10–13 mm, B (medium) 13–17 mm, and C (large) >17 mm.
Results:
Subgroup analysis according to CBD stone size showed EPT + EPBD had a significantly better initial stone clearance rate than EPT in Groups B (odds ratio [OR] = 2.39, 95% confidence interval [CI]: 1.20–4.77) and C (OR = 3.05, 95% CI: 1.86–5.03), but not for Group A (OR = 1.41, 95% CI: 0.90–2.21). EPT+EPBD also required significantly less ML than EPT in Groups B (OR = 0.34, 95% CI: 0.15–0.77) and C (OR = 0.31, 95% CI: 0.13–0.73). EPT+EPBD had significantly shorter procedure time than EPT in Group B (standardized mean difference = −1.20, 95% CI: −2.08 to 0.32). In meta-regression analysis, Group B had a better OR in initial stone clearance rate and less ML usage rate correlation with the size of CBD stone, but not for Group C with larger stones.
Conclusions
: EPT+EPBD had a significantly better initial stone clearance rate, and required less ML with shorter procedure time than EPT for removing medium-sized CBD stones, but the efficacy was limited to large CBD stones. The study protocol and trial registration had been registered in PROSPERO (Registration No. CRD42020171689).
Introduction
Choledocholithiasis or common bile duct (CBD) stones occur in 10%–20% of patients with gallbladder stones,1,2 and an estimated 15% will eventually become symptomatic 3 and require further treatment. Currently, standard treatment for large CBD stones includes endoscopic retrograde cholangiopancreatography (ERCP) and endoscopic sphincterotomy (EPT) 4 (Some scholars also abbreviate EPT as EST), or endoscopic sphincterotomy followed by large balloon dilation (EPT+EPBD) (also collectively called EST with balloon dilatation, ESBD). 5
EPT involves cutting the biliary sphincter to facilitate removal of CBD stones. 6 Adverse events of the procedure include postsphincterotomy pancreatitis, hemorrhage, perforation, cholangitis, cholecystitis, and procedure-related death. 7 In 2003, Ersoz et al. 8 described EPT+EPBD, which involves a sphincterotomy before using a large-sized balloon to dilate the papillary orifice. This combination improves the passage of larger CBD stones and avoids the risk of stone impaction.
Recent guidelines5,9–12 have suggested that EPT+EPBD may play an important role in the management of large CBD stones. However, few studies have focused on the clinical application of EPT+EPBD. Therefore, a more detailed review and meta-analysis to compare the efficacy of EPT+EPBD versus EPT based on CBD stone size are needed. We conducted a meta-analysis to determine the efficacy of these two techniques in the overall management of CBD stones.
We performed subgroup analysis based on stone size to evaluate its effect on the efficacy and safety of EPT+EPBD in CBD stone clearance. We attempt to define the suitable CBD stone size for EPT+EPBD based on existing clinical data and evidence, to support the application of this technique in clinical practice. The primary endpoints included successful stone removal during the first or initial session of ERCP, including the need for mechanical lithotripsy (ML) and procedure time.
Materials and Methods
This study was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. 13
Study selection
This meta-analysis and systematic review included studies that (1) were randomized control trials (RCTs) and non-RCTs involving primary experimental designs; (2) were designed with clearly defined interventions, that is, EPT+EPBD versus EPT; (3) included participants with CBD stones (mean CBD stone size more than 10 mm or larger CBD diameter); (4) were published in English between 2003 and 2022; and (5) included one of the outcome variables. Studies were excluded if they (1) were published in a non-English journal; (2) were meta-analyses or review studies; and (3) did not include a comparison group.
Search strategy and data sources
Comprehensive searches of Embase, PubMed, and Web of Science were conducted for studies published between January 1, 2003, and February 1, 2022. A medical librarian (M.-L.F.) assisted in developing the search strategies. Sets of keywords were used in conjunction with OR and AND to ensure that the search was comprehensive. In addition, we cross-referenced and manually searched the bibliographies of pertinent studies. Detailed search strategies and results are summarized in Supplementary Appendix S1. The search yielded 1457 articles, of which 992 nonduplicate citations were screened. Eleven RCTs and 11 non-RCTs were ultimately selected for analysis (Fig. 1).
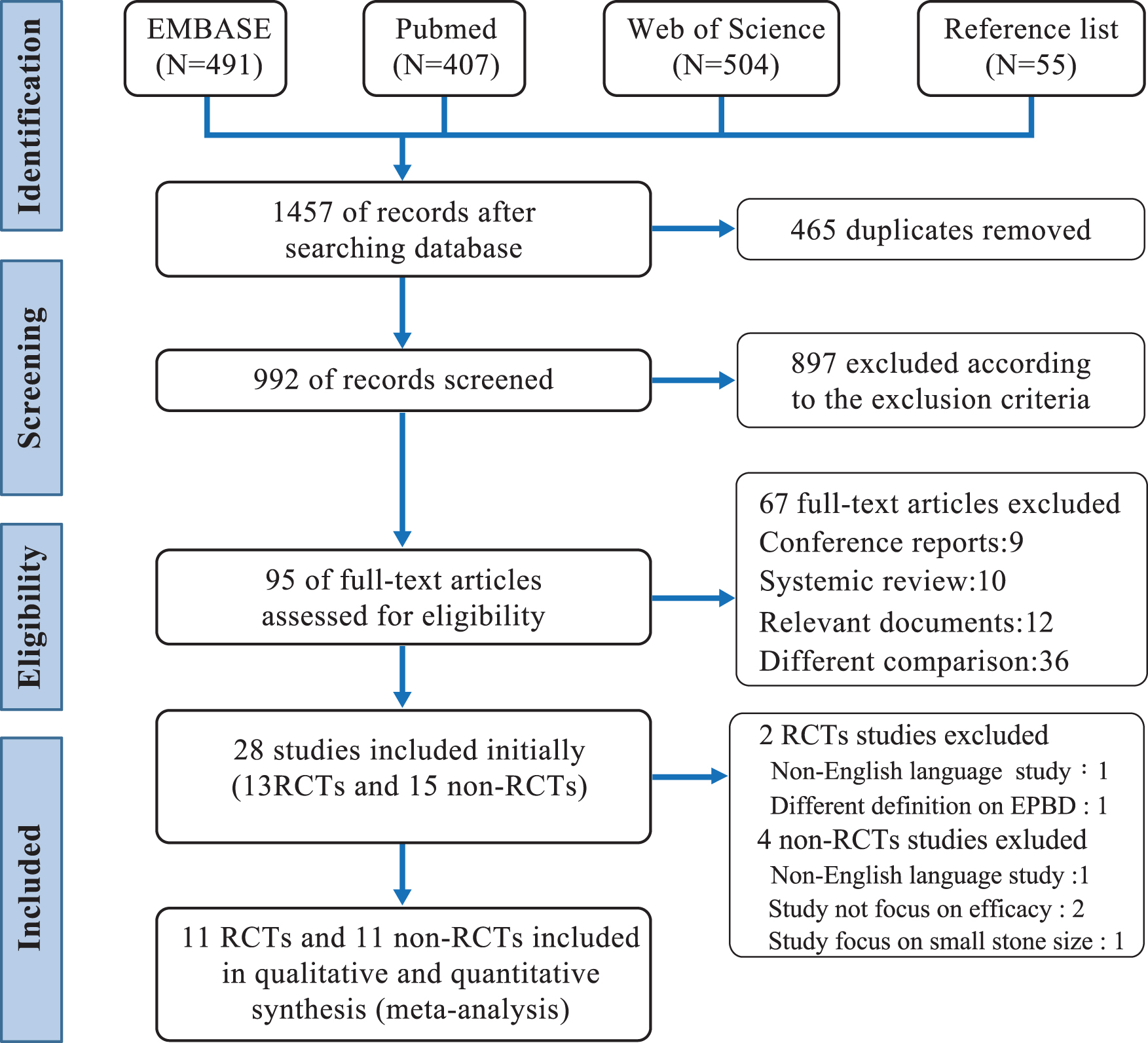
Flowchart studies included in the meta-analysis.
Data extraction and quality assessment
Two investigators (T.-W.C. and J.-L.C.) independently extracted study data including publication year, study design, study population, characteristics of the stones, type of endoscopic technique performed, rate of successful first-session stone removal, the need for ML, and recorded adverse events. Eligibility for study inclusion was based on these data. Any discrepancies or disagreements on which studies to include were resolved through consensus. When the study investigators could not agree, a third investigator (J.L.) was consulted.
We used the Cochrane Risk of Bias Tool to assess quality and risks of bias for the RCTs 14 and the modified Newcastle–Ottawa Scale (NOS) 15 according to Cummings et al. 16 to assess quality and risks of bias for the non-RCTs. Two investigators (T.-W.C. and J.-L.C.) independently conducted quality assessment of the RCTs and non-RCTs. The criteria used are presented in Supplementary Figure S1A and B. Stone size was assessed by comparing the largest diameter of the stone with the (ERCP scope) diameter of the duodenoscope 12–13 mm, as measured on the cholangiogram. In addition, dilatation balloon diameter (12, 15, 18, and 20 mm) was chosen according to the CBD stone size and was used as a reference for comparing CBD stone size.
Despite a difference in balloon size, dilatation technique, and management algorithm, there was only minor variation across the included studies, and the main principle and purpose to remove CBD stones are similar among the expert endoscopists. The management algorithm and CBD stone size evaluation method in included studies are summarized in Table 1. In our study, subgroup analyses were performed based on the mean or biggest one CBD stone size of the included studies that they were grouped under A (small): 10–13 mm, B (medium): 13–17 mm, and C (large): >17 mm. They were classified based on reference to the diameter of the (duodenoscope) (12–13 mm) or the diameter of dilation balloons (>17 mm)17,18 for subgroup analysis (Table 2). In clinical practice, CBD stone size is a variable, which is difficult to define with millimeter precision.
Included Studies for Endoscopic Sphincterotomy+Endoscopic Papillary Large Balloon Dilation Management Algorithm, Balloon Size and Dilatation Technique, Evaluation Methods for Common Bile Duct Stone Size, and Procedure Time
Studies have small variations on estimated procedure time: time between randomization and occlusion cholangiogram.
Studies have small variations on estimated procedure time: time between identifying frontal imaging of Vater's papilla to the end of the stone removal procedure.
Studies with modified EPBD by inflation dilatation balloon to estimate target size on cholangiogram or to estimate target pressure.
CBD, common bile duct; CT, computed tomography; EPBD, endoscopic papillary large balloon dilation; EPT, endoscopic sphincterotomy; ES, endoscopic sphincterotomy; MRCP, Magnetic resonance cholangiopancreatography; N/A, not applicable; ref., reference.
Characteristics of Common Bile Duct Stones and Baseline Patient Data of the Included Studies in Comparisons of Endoscopic Sphincterotomy+Endoscopic Papillary Large Balloon Dilation Versus Endoscopic Sphincterotomy
According to the mean size of the CBD stones, studies divided into subgroup analysis (a): groups A (small) 10–13mm; (b): B (medium) 13–17 mm, and (c): C(large) >17 mm.
Studies with unavailable mean or biggest CBD stone size and not included in subgroup analysis.
CBD, common bile duct; EPT, endoscopic sphincterotomy; EPBD, endoscopic papillary large balloon dilation; N/A, not applicable.
After checking the CBD stone measurement method for each of the included studies, we found that most studies assess CBD stone size, number, and bile duct size based on the cholangiogram findings during ERCP, and this was true for both RCTs and non-RCTs and therefore difficult to blind in RCT studies. Therefore, pooled data combining RCTs and non-RCTs were performed for this meta-analysis to study the relationship between stone size and efficacy of EPT+EPBD in stone removal.
Data synthesis and analysis
We used statistical software (Stata 15.0; Stata Corp., College Station, TX, USA) to calculate pooled odds ratios (ORs), risk differences, or standardized mean differences (SMDs) with 95% confidence intervals (CIs) for each pairwise comparison. 19 Pooled ORs and their 95% CIs were estimated with a fixed-effects model if there was no significant heterogeneity, and with a random-effects model if significant heterogeneity existed.
Two methods were used to assess heterogeneity: the chi-square-based Q test, the results of which were considered to be statistically significant if the P value was < .05; and I2 statistics, in which values 30%–60% and 60%–90% suggested moderate and substantial heterogeneity, respectively.20,21 Sensitivity analyses were performed to verify the source of heterogeneity. 14
Relationships between stone size and outcomes (first stone clearance rate and ML usage rate) were analyzed using meta-regression with the logarithmic ORs (log OR) as the dependent variable. 22 Log OR equal 0 means OR equal 1.
Publication bias was assessed qualitatively by inspecting funnel plots of log OR versus their standard errors, and quantitatively using the Egger regression test 23 and Begg and Mazumdar adjusted-rank correlation test. Publication bias was considered present if the P value was < .1. 24
Results
Eleven RCTs18,25–34 and 11 non-RCTs35–45 involving a total of 3482 patients with CBD stone disease were included in the analysis. Subgroup analysis based on CBD stone size (small, medium, and large) of included studies was conducted to assess the efficacy and safety of EPT+EPBD. Relationships between stone size and clinical outcomes (i.e., initial stone clearance rate and need for ML) were further analyzed using meta-regression analysis. Characteristics of the CBD stones and baseline patient demographics are summarized in Table 2.
Primary outcome assessment: efficacy of EPT + EPBD versus EPT on experimental studies and real-world studies
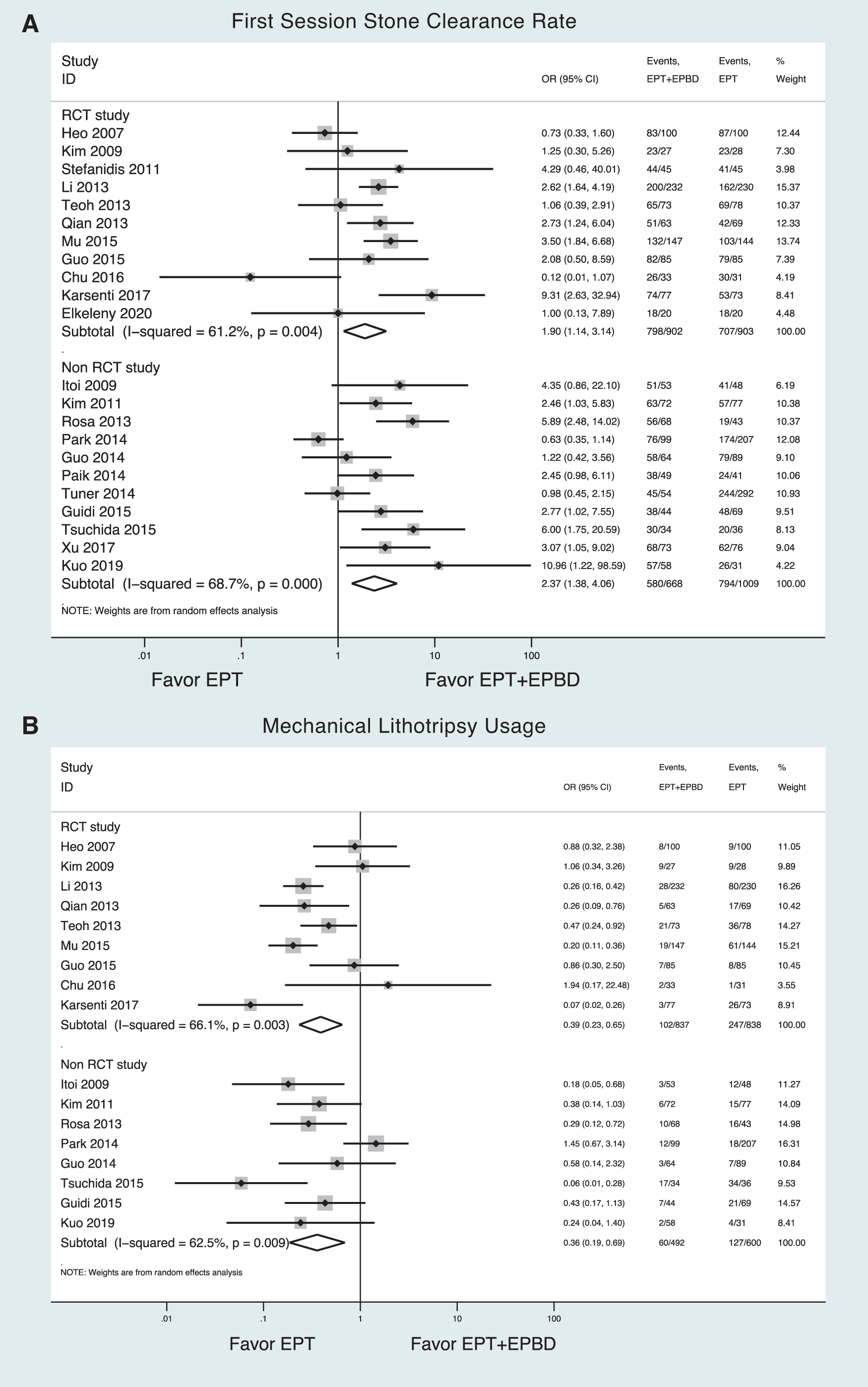
Meta-analysis on first session stone clearance rate of EPT+EPBD versus EPT for removal CBD stones in RCTs and non-RCTs: EPT+EPBD had a significantly better stone clearance rate during the first session of the intervention than EPT in both RCTs (OR = 1.90, 95% CI: 1.14–3.14) and non-RCTs (OR = 2.37, 95% CI: 1.38–4.06) (Fig. 2A).
Meta-analysis on ML usage rate of EPT+EPBD versus EPT in removal of CBD stones in RCTs and non-RCTs: EPT+EPBD had a significantly lower rate of ML than EPT in both RCTs (OR = 0.39, 95% CI: 0.23–0.65) and non-RCTs (OR = 0.36, 95% CI: 0.23–0.65) (Fig. 2B).
Meta-analysis on procedure time of EPT+EPBD versus EPT in removal of CBD stones in RCTs and non-RCTs: Pooled data revealed that EPT+ EPBD had a shorter procedure time than EPT in the RCTs (SMD = −0.63, 95% CI: −1.11 to 0.65), but not in the non-RCTs (SMD = −0.44, 95% CI: −1.18 to 0.31) (Supplementary Fig. S2A).
Meta-analysis on post-ERCP pancreatitis of EPT+EPBD versus EPT in the removal of CBD stones in RCTs and non-RCTs: Pooled data for safety analysis revealed that EPT+EPBD is a safe procedure and its post-ERCP pancreatitis rate was similar with EPT in the RCTs (OR = 0.89, 95% CI: 0.56–1.4) and non-RCTs (OR = 0.84, 95% CI: 0.50–1.40) (Supplementary Fig. S2B).
Pooled rate ratio for first-session stone clearance rate
Subgroup analysis based on stone size (according to the diameter of the duodenoscope 13 mm and large dilatation balloon 18 mm)
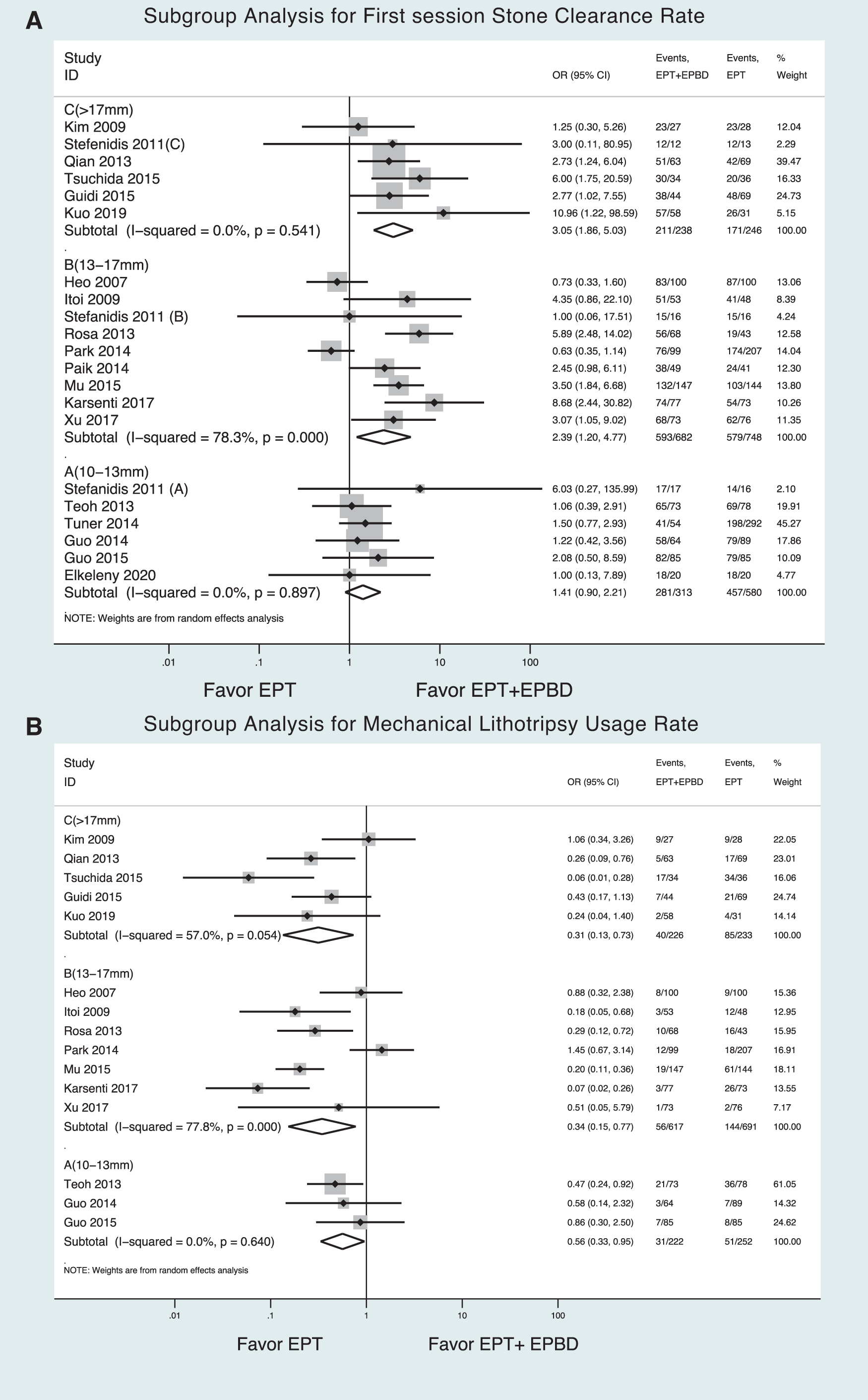
Pooled rate ratio for subgroup analysis in combining RCTs and non-RCTs for first session stone clearance rate, ML usage rate, and procedure time: Pooled data combining RCTs and non-RCTs studies were performed for efficacy analysis, EPT+EPBD had a significantly better initial stone clearance rate than EPT in Group C (OR = 3.05, 95% CI: 1.86–5.03) and Group B (OR = 2.39, 95% CI: 1.20–4.77), but not in Group A (OR = 1.41, 95% CI: 0.90–2.21) (Fig. 3A). In addition, EPT+EPBD had a lower ML usage rate than EPT in Group C (OR = 0.31, 95% CI: 0.13–0.73), Group B (OR = 0.34, 95% CI: 0.15–0.77), and Group A (OR = 0.56, 95% CI: 0.33–0.95). Even though EPT+EPBD was better than EPT in each subgroup in this analysis, the ORs in Groups C and B were better than in Group A (Fig. 3B).
In procedure time analysis, EPT+EPBD had a significantly shorter procedure time than EPT in Group B (SMD = −1.20, 95% CI: −2.08–0.32), but not in Group A (SMD = −0.26, 95% CI: −1.32–0.61) or Group C (SMD = −0.11, 95% CI: −0.31–0.10) (Fig. 4A). Pooled data for safety analysis revealed that EPT+EPBD versus EPT had a similar post-ERCP pancreatitis rate among Groups A, B, and C (Fig. 4B).
Pooled rate ratio for first-session stone clearance rate

Pooled rate ratio for procedure time
Meta-regression analysis of CBD stone size correlation with log ORs (EPT+EPBD versus EPT) for first stone clearance and ML usage rate
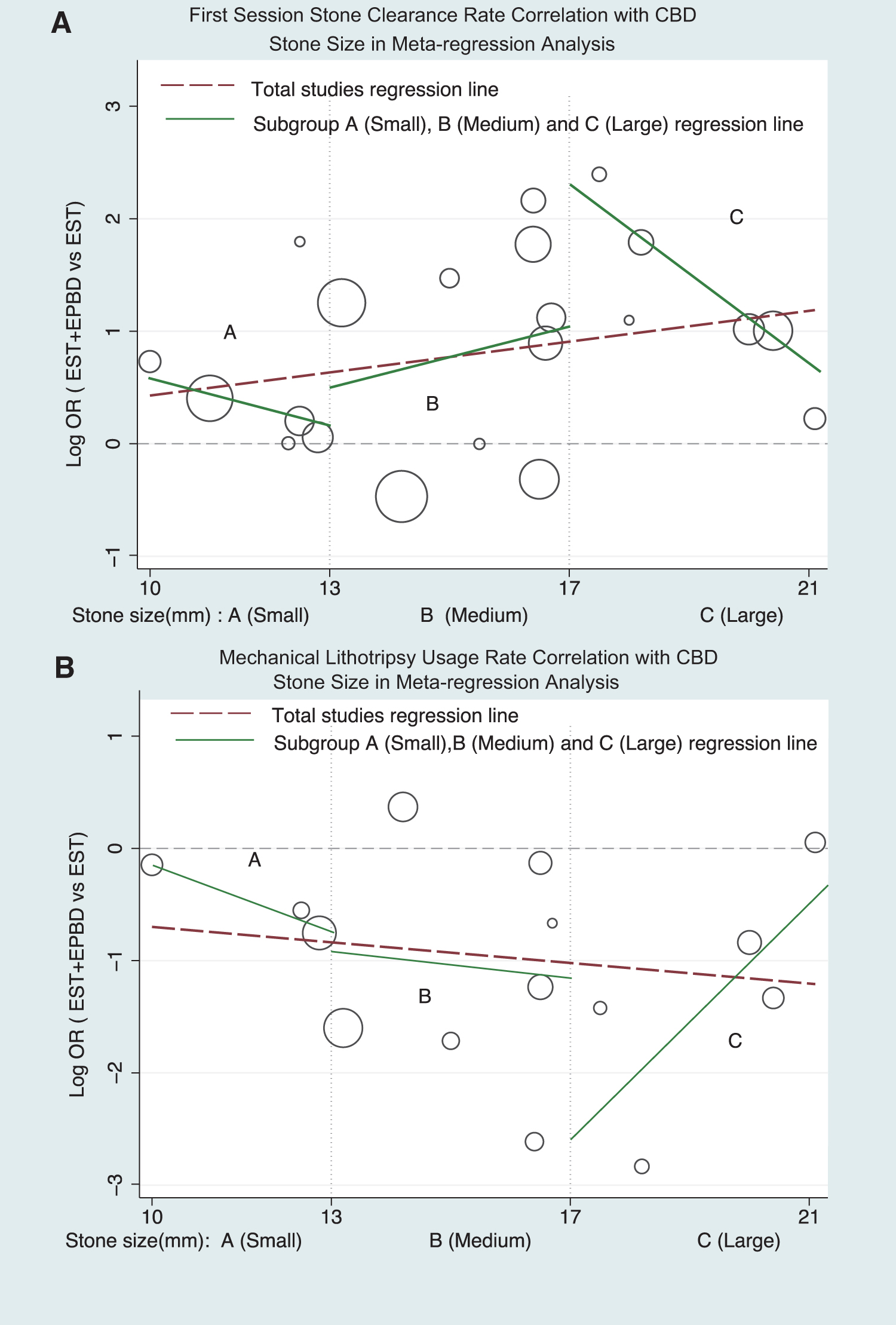
In meta-regression analysis for CBD stone size, Group B had a better coefficient with log OR (EPT+EPBD versus EPT) and OR over 1 in first stone clearance rate as stone size increases. Group B with positive slope rate (slope coefficient up to 1.88) than Group A and C with negative slope rate indicated Group B or the medium size stones have the best initial stone clearance rate for EPT+EPBD than EPT when stone size increases. In Groups A and C, size of CBD stones had a negative slope coefficient with a trend of OR near 1 (Log OR = 0 means OR = 1). The slope coefficient became negative and near 0 especially in Group C with a larger size stone, indicating that the initial stone clearance rate for EPT+EPBD was not better than EPT (Fig. 5A).
In meta-regression analysis correlation of log OR with stone size in ML usage rate: in Group B analysis, Log OR was kept negative (OR <1) and OR less than 1 indicating that EPT+EPBD required less ML usage than EPT. In contrast, a trend of OR near 1 in some Group A and C studies, indicating that the frequency of ML usage became more equivalent for both EPT+EPBD and EPT for smaller size stone in Group A and larger size stone in Group C (Fig. 5B).
Pooled rate ratio for first-session stone clearance rate
Quality assessment results
All of the 11 RCTs were of moderate-to-high quality and three had allocation bias (Supplementary Fig. S1A). Of the 11 non-RCTs, 10 did not indicate how the sample size was calculated, and 7 had partial adjustments for confounding factors related to the papilla (i.e., the presence of periampullary diverticulum and naive papilla or postsphincterotomy). Eight non-RCTs were of high quality (Supplementary Fig. S1B).
Publication bias
A funnel plot showed symmetry, and 8/11 RCTs and 9/11 non-RCTs were within the 95% confidence limit, as shown in Supplementary Figure S3A. Egger's test 23 for small-study effect analysis showed t = 0.60, P = .555, as shown in Supplementary Figure S3B.
Discussion
A combined EPT+EPBD offers a more effective way of destroying the biliary sphincter as the radial expansion force of the dilation balloon provides stretching and a more complete tear of the sphincter muscle, and the size of the opening is indicated by the diameter of the dilation balloon. The usual assessment of stone size is done by referencing the instrument used (e.g., diameter of a therapeutic duodenoscope 13 mm, or a fully inflated dilation balloon is >17 mm), because of this, the bile duct stone size that influenced the therapeutic outcome could not be blinded during the ERCP procedures.
According to the meta-analysis on efficacy and safety, we found that the efficacy study on real-world non-RCTs is similar and comparable with the RCT studies (Fig. 2 and Supplementary Fig. S2). These results were partially attributed to the nature of the ERCP procedure, which is skill and technology dependent. In contrast, well-designed non-RCT studies can preserve the basic parameters and reflect the real-world status than experimental studies especially on the therapeutic strategy ( Supplementary Fig. S2A). To verify the true efficacy of EPT+EPBD in the removal of CBD stones of different sizes, we combined non-RCT and RCT data after performing quality assessment on each study, the management algorithm, and CBD stone size evaluation method (Table 1).
Our analysis showed that combined EPT+EPBD had a significantly higher success rate of removing medium-sized (13–17 mm) CBD stones during the initial ERCP and required less ML to assist in ductal clearance than EPT based on both RCTs and non-RCTs.
In subgroup analysis based on stone size, it showed that EPT+EPBD had a significantly better stone clearance rate than EPT in the initial ERCP session for Groups B (medium) and C (large) (Fig. 3A). Meta-regression analysis revealed that EPT+EPBD was more superior than EPT in Group B with a better OR correlation and better efficacy in initial stone clearance rate, but the coefficient of Log OR slope became negative and near 0 for Group C, meaning the OR is decreasing and near 1 as stone size increases in Group C, which limits the efficacy of EPT+EPBD (studies with large-sized CBD stones) (Fig. 5A).
ML is often needed to reduce stone size to facilitate removal. In our analysis, EPT+EPBD had a much lower ML usage rate than EPT. In subgroup analysis according to mean stone size, meta-regression showed that EPT+EPBD had less ML usage rate than EPT in Group B (Log OR negative and below 0). In Groups A and C, the usage of ML was similar between EPT+EPBD and EPT for log OR near 0 (OR = 1) (Fig. 5B). This indicates that the frequency of the usage of ML for removal of smaller stone in Group A and larger stone in Group C was similar for both EPT+EPBD and EPT. The larger size of the stones in Group C limited the efficacy of EPT+EPBD in stone removal.
With regard to procedure time, EPT+EPBD had a shorter procedure time than EPT in the RCTs, and especially for stones in Group B (Fig. 4B). It is understandable that small stones may not require lithotripsy because extraction is easy with either procedure. However, larger stones will often require lithotripsy to fragment the stone to facilitate extraction and ductal clearance. EPT+EPBD is more effective in destroying the sphincter of Oddi and thus achieves better patency for the exit passage (distal bile duct and sphincterotomy), which facilitates stone extraction and reduces the risk of stone impaction.
The sphincter of Oddi consists of two groups of circular muscles: the common sphincter (first ring) and the biliary sphincter (second ring), which is known as the “two-ring theory.” 46 EPT+EPBD can open both rings, while EPT can only cut the distal first ring. EPT+EPBD is therefore more effective in opening both biliary and common sphincters than EPT to facilitate clearance of medium stones (Group B). Larger stones (Group C), which approach the maximum diameter of dilation balloons, will likely require more ML for stone fragmentation to facilitate ductal clearance. In summary, EPT+EPBD in Group B had better efficacy than Groups A and C, as shown in this meta-analysis. Future studies may allow for better comparison between the two techniques with regard to different sized CBD stones.
To the best of our knowledge, this meta-analysis is the first to evaluate the efficacy of EPT+EPBD versus EPT based on CBD stone size. However, there are some limitations to this study. We only included articles that were published in English, and included studies with a defined stone size clearly. In addition, small variations in the combined technique of EPT and EPBD existed among the studies. These variations and bias were verified during the study and to minimize their influence on outcome analysis.
Conclusions
EPT+EPBD has different efficacies in stone clearance among small-, medium-, and large-sized CBD stones compared with EPT and a safe procedure as EPT.
For small CBD stones (Group A), EPT+ EPBD has a similar initial stone clearance rate as EPT.
For medium CBD stones (Group B), EPT+EPBD has a significantly better first-session CBD stone clearance rate, required less ML, and a shorter procedure time than EPT.
For large CBD stones (Group C), the initial stone clearance rate and ML rate for EPT+EPBD were similar and not better than EPT for larger Group C stones (size more than 20 mm). The large stones may limit the efficacy of EPT+EPBD in ductal clearance.
Footnotes
Acknowledgments
The authors thank Isabel Elane Allen for statistic assistance and Malcolm Higgins for proofreading the article.
Authors' Contributions
T.-W.C. and J.-L.C. were involved in the conceptualization and methodology of the study; in the collection, analyses, and interpretation of data; in the writing of the article, and in the decision to publish the results. J.-J.C., P.-L.L, H.-D.T, M.-L.F., M.-C.O.Y., and J.L. were involved in the acquisition and interpretation of data for the work. All authors have read and agreed to the published version of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.