
Abstract
Introduction:
Laparoscopic pancreaticoduodenectomy (LPD) is gaining wide acceptance within pancreatic surgery. However, longitudinal data are lacking. The aim of this study was to analyze and assess the short-term outcomes and long-term survival of LPD over a duration of 8 years.
Methods:
Patients who underwent LPD in our institution between November 2013 and September 2021 were included in this study. The perioperative outcomes were statistically analyzed. The long-term survival was studied over a median follow-up duration of 13 months.
Results:
In total, 653 consecutive patients treated at our institution were included, of which 617 cases underwent standard LPD and 36 cases underwent LPD with vascular resection. The rate of death in hospital, reoperation, postpancreatectomy hemorrhage, postoperative pancreatic fistula, and delayed gastric emptying were 4.4%, 10.3%, 11.9%, 12.9%, and 6.1% respectively. There were statistical differences in the intraoperative blood loss and transfusion, operation time, and the R0 resection rate between the LPD cases and LPD with vascular resection cases. A total of 526 cases were pathologically diagnosed of cancer. The 1-, 3-, and 5-year survival rates were 49.2%, 17.9%, and 17.9%, respectively, for pancreatic cancer with the median survival time of 12 months. The 1-, 3-, and 5-year survival rates were 76.9%, 60.8%, and 52.5%, respectively, for bile duct cancer with the median survival time of 35 months. The 1-, 3-, and 5-year survival rates were 80.2%, 62.2%, and 52.9%, respectively, for duodenal cancer with the median survival time of 53 months. The 1-, 3-, and 5-year survival rates were 72.5%, 54.5%, and 50%, respectively, for ampullary cancer with the median survival time of 55 months.
Conclusion:
LPD is a feasible and oncologically acceptable procedure with satisfying perioperative outcomes and long-term survival in a high-volume institution.
Introduction
Laparoscopic pancreaticoduodenectomy (LPD) is a technically demanding and minimally invasive procedure in treating pancreatic cancer, periampullary malignancies or low-grade malignant neoplasm, and benign disease. Compared with open pancreaticoduodenectomy, most studies revealed favorable perioperative outcomes of LPD.1–16 The conflicting evidence on the perioperative outcomes of LPD is associated with the surgeon experience and hospital volume, which are essential for a medical center to reach the end of the learning curve. 17 In China, LPD has already been widely performed in many large medical centers as a routine surgery after a difficult and controversial developmental process.18,19 Although LPD is gaining worldwide acceptance within pancreatic surgery, there were only a few studies concerning both the short-term outcomes and long-term survival of LPD with a large sample. Given the lack of longitudinal data, we aimed to analyze and assess the perioperative outcomes and long-term survival of the 653 LPD cases in our institution, carried out LPD over a period of 8 years.
Patients and Methods
Patients
A total of 653 consecutive patients who underwent LPD in our institution between November 2013 and September 2021 were included in this study. No patient was excluded. The LPD carried out in our institution included standard LPD and LPD with vascular resection for patients without distant metastasis. The pathological diagnoses included malignant tumors (pancreatic head cancer, bile duct cancer, and duodenal cancer), benign tumors, and inflammation. The clinical and long-term survival data were obtained from our internal research database. This study was approved by the institutional review board of the Second Hospital of Hebei Medical University, Shijiazhuang, Hebei Province, China. This study was performed in accordance with the relevant guidelines and regulations and was approved by the Research Ethics Committee of the Second Hospital of Hebei Medical University, Shijiazhuang, Hebei Province, China. Informed consent was obtained from all the study subjects.
Operative techniques
The standard LPD was performed in the following order. (1) The gastrocolic ligament was dissected and the duodenum was mobilized by performing the Kocher maneuver. (2) The right gastroepiploic and pancreaticoduodenal inferior vessels were dissected, ligated, and transected. (3) The distal stomach 2–3 cm from the pylorus was transected. (4) A tunnel was created between the pancreatic neck and the superior mesenteric vein (SMV) or portal vein at the inferior border of the pancreas. (5) The jejunum was exposed through the Riolan avascular area on the left of the SMV and transected 15–20 cm distal from the Treitz ligament. (6) Lymphadenectomy of the hepatoduodenal ligament was performed and the gastroduodenal artery was transected. (7) The jejunum and duodenum were completely mobilized from left to right to expose major vasculatures. (8) The pancreas neck was transected. (9) Cholecystectomy was performed and the common hepatic duct was transected. (10) The inferior vena cava and the left renal vein were exposed by performing the Kocher maneuver. (11). The uncinate process was separated from the SMV. (12) Lymphadenectomy was performed, including the lymph node stations of 5, 6, 8a, 13a, 13b, 14a, 14b, 17a, and 17b. (13) The specimen placed in a retrieval bag was extracted through a 5-cm upper abdominal incision. (14) Pancreatojejunostomy: a duct-to-mucosa anastomosis was performed. (15) Choledochojejunostomy: an end-to-side with ∼10 cm distal to the anastomosis of pancreatojejunostomy was performed. (16) Gastrojejunostomy: ante colic gastrojejunostomy was performed 40–45 cm downstream from the choledochojejunostomy.
As in cases of LPD with vascular resection, wedge resection with repair or circular resection with end-to-end anastomosis was performed when the uncinate process was separated from the SMV. A venous graft was required when the vascular defect was longer than 3 cm.
Data collection and follow-up
Patient characteristics, preoperative laboratory test results, intraoperative data, postoperative complications, and in-hospital outcomes were extracted from the patients' electronic medical records. The long-term survival data were obtained from routine patient or clinic follow-up. All the data were recorded in our internal research database.
Patient characteristics included age, sex, BMI, American Society of Anesthesiologists (ASA) score, and comorbidities (coronary heart disease, high blood pressure [HBP], diabetes mellitus [DM], pancreatitis, hepatitis, and operative history). Preoperative laboratory test results included serum albumin and direct bilirubin. Intraoperative data included blood loss, intraoperative transfusion, and operation time. Postoperative complications included postoperative pancreatic fistula (POPF), delayed gastric emptying (DGE), postpancreatectomy hemorrhage (PPH), abdominal infection, and the Clavien–Dindo classification of surgical complications. In-hospital outcomes included reoperation, death in hospital, intensive care unit (ICU) stay, R0 resection, harvested lymph nodes, positive lymph nodes, and pathological results. Operation time was defined as the duration from the first incision to final closure. POPF, 20 PPH, 21 DGE, 22 and the Clavien–Dindo classification of surgical complications23,24 were defined according to the consensus and guidelines. Abdominal infection was defined as the postoperative fever and increasing level of white blood cells (>10 × 10^9/L) with exclusion of infections in other organs. R0 resection was defined as no tumor cells present at the surface of the specimen margin according to the definition of the Union for International Cancer Control.
Follow-up was calculated in months from the surgery date to the event occurrence or October 31, 2021, and the loss to follow-up rate was 3.7%. The endpoint was death. The median follow-up was 13 months (interquartile range [IQR], 7–30), for a total of 1159 patient-years.
Statistical analysis
Normally distributed continuous variables were presented as mean ± standard deviation and compared using Student's t-tests with Levene's test for homogeneity of variance. Non-normally distributed variables were presented as median with IQR and compared using Mann–Whitney U-tests. Categorical variables were presented as number with percentage and compared using chi-square tests. Longitudinal endpoints were evaluated by the Kaplan–Meier analyses. Statistical analyses were conducted using IBM SPSS Statistical 26.0 (IBM Corp, Armonk, NY). A value of P < .05 was the criterion for statistical significance.
Results
Preoperative clinical characteristics
A total of 653 consecutive patients underwent LPD, including 617 cases of standard LPD and 36 cases of LPD with vascular resection. Patients included 398 men and 255 women with the average age of 59.5 ± 10.8 years. Average BMI was 23.5 ± 3.6 kg/m2. Most patients (85.3%) were categorized as ASA Grade II. Common comorbidities were HBP (31.4%) and DM (16.1%). Preoperative albumin average level was 38.3 ± 4.9 g/L. Preoperative direct bilirubin level was 84.0 ± 83.6 mmol/L. There was no statistical difference in preoperative clinical characteristics between LPD cases and LPD with vascular resection cases. Statistical analyses of patient characteristics and preoperative laboratory test results are given in Table 1.
Statistical Analyses of Patient Characteristics and Preoperative Laboratory Test Results
Independent samples t-tests.
Chi-square tests.
Mann–Whitney U-tests.
ASA, American Society of Anesthesiologists; BMI, body mass index; CHD, coronary heart disease; DM, diabetes mellitus; HBP, high blood pressure; LPD, laparoscopic pancreaticoduodenectomy.
Intraoperative and short-term outcomes
The median intraoperative blood loss was 400 (IQR, 200–800) mL. A total of 344 patients (52.7%) had intraoperative transfusion. The median operation time was 400 (IQR, 320–480) minutes. Eighty-four patients (12.9%) had POPF. Forty patients (6.1%) had DGE. Seventy-eight patients (11.9%) had PPH. Seventy-three patients (11.2%) had abdominal infection. A total of 388 patients (59.4%) had minor complications, whereas 146 patients (22.4%) had major complications according the Clavien–Dindo classification. Sixty-seven patients (10.3%) had reoperations. Twenty-nine patients (4.4%) were dead in hospital. The R0 resection rate was 96.6%. Median ICU stay was 0 (IQR, 0–0) day. Median number of harvested lymph nodes was 11 (IQR, 5–14). Median number of the positive lymph nodes was 0 (IQR, 0–0). For the pathological results, 526 patients (80.6%) were diagnosed with malignancies. There were statistical differences in intraoperative blood loss and transfusion, operation time, R0 resection rate, the number of harvested and positive lymph nodes, and the pathological results of the locations of the malignant tumors between LPD cases and LPD with vascular resection cases. LPD with vascular resection cases had more intraoperative blood loss, higher intraoperative transfusion rate, longer operation time, lower R0 resection rate, and more harvested and positive lymph nodes. Vascular invasion was most found in pancreatic head cancer. Statistical analyses of intraoperative date and short-term outcomes are given in Table 2.
Statistical Analyses of the Intraoperative Data and Short-Term Outcomes
Median and quartiles of the parameter [M(Q1–Q3)].
Mann–Whitney U-tests.
Chi-square tests.
ICU, intensive care unit; LPD, laparoscopic pancreaticoduodenectomy.
Long-term survival
A total of 288 cases (54.8%) had adjuvant therapy after surgery. Figure 1 provides the Kaplan–Meier survival analysis of four distinct cumulative survival curves in patients with different cancers. There was statistical difference between the curves (P < .001). The median survival time of pancreatic cancer, bile duct cancer, duodenal cancer, and ampullary cancer were 12, 35, 53, and 55 months. The 1-, 3-, and 5-year survival rates were 49.2%, 17.9%, and 17.9%, respectively, for pancreatic cancer. The 1-, 3-, and 5-year survival rates were 76.9%, 60.8%, and 52.5%, respectively, for bile duct cancer. The 1-, 3-, and 5-year survival rate were 80.2%, 62.2%, and 52.9%, respectively, for duodenal cancer. The 1-, 3-, and 5-year survival rate were 72.5%, 54.5%, and 50.0%, respectively, for ampullary cancer. The survival rates of the patients with cancer are given in Table 3. The LPD cases of pancreatic cancer had the worst long-term survival, whereas the duodenal cancer had the best long-term survival.
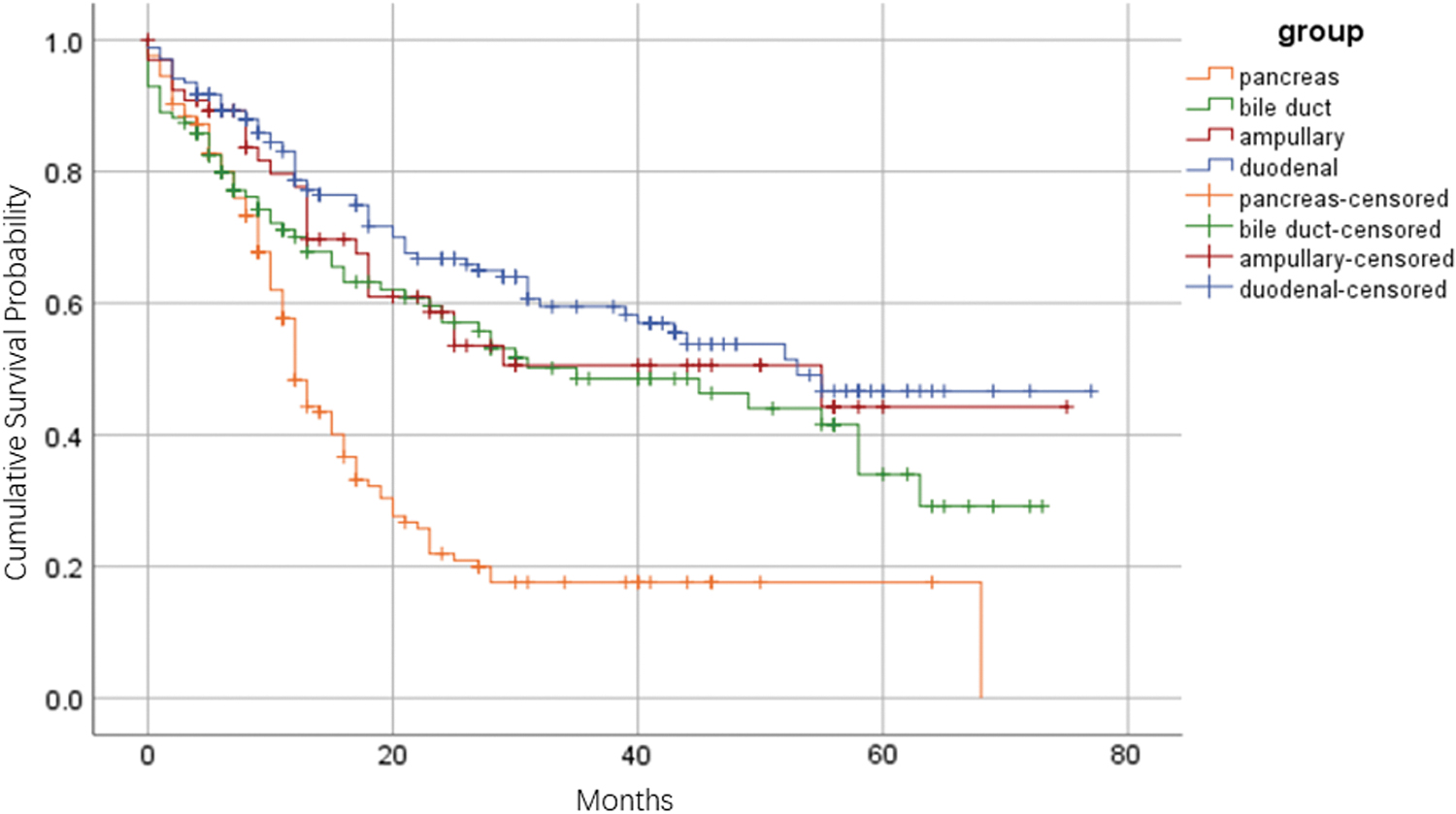
Kaplan–Meier survival analysis of four distinct cumulative survival curves in LPD cases with different cancers. LPD, laparoscopic pancreaticoduodenectomy.
Survival Rates of Laparoscopic Pancreaticoduodenectomy Cases with Cancer in Our Institution
Discussion
LPD has been widely performed in China nowadays. Concomitant vascular resection during LPD is performed in cases with vascular invasion. Positive and promising results of the safety and feasibility of LPD were reported in the studies carried in large medical centers in China.19,25,26 After a long and challenging learning curve, LPD has become a routine surgery in our institution. To better assess and improve the LPD technique, we longitudinally analyzed the data over a median follow-up duration of 13 months (IQR, 7–30), for a total of 1159 patient-years. Our study represents one of the largest reported series of perioperative outcomes and long-term survival of LPD cases from a single institution in China.
The perioperative outcomes of LPD cases in our institution were analyzed. Our study showed that the median intraoperative blood loss was 400 (IQR, 200–800) mL and the median operation time was 400 (IQR, 320–480) minutes. The most common complication was POPF (12.9%). A total of 146 patients (22.4%) had major complications according the Clavien–Dindo classification with the reoperation rate of 10.3%. The in-hospital death rate was 4.4%. The R0 resection rate was 96.6%. Most of the LPD cases without R0 resection were found in LPD with vascular resection cases. Although we diagnosed according to the clinical symptoms, imaging scans, and laboratory tests, only 80.6% of the cases were diagnosed with malignancies, indicating that our methods for diagnosis should be improved. Vascular invasion was mostly found in pancreatic head cancer. LPD with vascular resection cases had more intraoperative blood loss, higher intraoperative transfusion rate, longer operation time, lower R0 resection rate, and more harvested and positive lymph nodes. The results indicated that the decision of LPD with vascular resection should be made cautiously.
Our study showed satisfying survival rates of LPD cases with cancer. A total of 288 cases (54.8%) had adjuvant therapy after surgery. The “cure rate” for pancreatic cancer is 9%, and without treatment, the median survival of patients with metastatic disease is only 3 months. 27 The 5-year survival rate of LPD cases with pancreatic cancer in our institution was 17.9% with a median survival time of 12 months. For the bile duct cancer, the 5-year survival associated with surgical resection of extrahepatic cholangiocarcinoma is estimated to be 16%–52%. 28 The 5-year survival rate of LPD cases with bile duct cancer in our institution was 52.5% with a median survival time of 35 months. For the duodenal cancer, the prognosis of duodenal cancer was reported to be better than that of other periampullary cancer with a 5-year survival rate of 25%–75% after surgical resection. 29 The 5-year survival rate of LPD cases with duodenal cancer in our institution was 52.9% with a median survival time of 53 months.
Ampullary cancer arises from the ampulla of Vater terminal to the confluence of the distal common bile duct and the pancreatic duct. Histological diagnosis is commonly intestinal epithelial (47%) or pancreatobiliary epithelial subtypes (24%). The 5-year survival rate of ampullary cancer ranges from 70% to 80% for node-negative disease compared with 20%–50% for node-positive disease. 30 The 5-year survival rate of LPD cases with ampullary cancer in our institution was 50.0% with a median survival time of 55 months.
There are limitations in this study. First, the long-term survival of LPD cases with vascular resection was not analyzed because of the small sample size. Second, the influence of adjuvant therapy on the long-term survival was not analyzed because of many different kinds of therapies. Further studies involving more detailed follow-up data should be carried to better assess the long-term survival of LPD cases.
In conclusion, LPD is a feasible and oncologically acceptable procedure with satisfying perioperative outcomes and long-term survival in a high-volume institution.
Footnotes
Authors' Contributions
D.L., J.L., C.D., J.Z., and T.Z. collected and analyzed the clinical data. D.L. and J.L. designed the study. L.R. and L.H. wrote the article. All authors read and approved the final version of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by two grants from the Key R&D Program of Hebei Province of China (Grant No. 19277758D) and the Nature Science Foundation of Hebei Province of China (Grant No. H2019206571).