
Abstract
Background:
In the difficult gallbladder, the rate of bile duct injury (BDI) remains high. To lessen iatrogenic biliary injury, we attempted to utilize indocyanine green (ICG)–guided fluorescence cholangiography during surgery to illuminate the extrahepatic biliary tract.
Materials and Methods:
According to admission criteria, 38 patients were diagnosed with difficult gallbladder and underwent percutaneous transhepatic gallbladder drainage (PTGBD). Consecutive patients who underwent ICG-assisted laparoscopic biliary surgery (n = 18, ICG group) or conventional laparoscopic biliary surgery (n = 20, white light [WL group) were enrolled in this study. ICG group received ICG fluorescent cholangiography via PTGBD tube during operation; 16 cases of laparoscopic cholecystectomy (LC) and 2 cases of LC plus laparoscopic common bile duct exploration (LC+LCBDE) were performed by fluorescent laparoscopy. In the WL group, 16 cases of LC, 1 case of laparoscopic subtotal cholecystectomy (LSC), and 3 cases of LC+LCBDE were performed under white light without ICG.
Result:
The biliary system was successfully established in the ICG group. Compared with the WL group, the anatomy of the Calot's triangle with severe abdominal adhesion or local inflammatory edema was more clearly displayed by fluorescence. Laparoscopic surgery was completed in both groups without conversion to laparotomy. There were no significant differences in surgery-related complications (P = .232) and postoperative hospital stay (P = .074) between the two groups. However, compared with the WL group, the ICG group had less intraoperative blood loss (P = .002) and shorter operation duration (P = .006).
Conclusion:
ICG fluorescence cholangiography has good clinical application value in the difficult gallbladder, which can avoid iatrogenic BDI, reduce surgery-related complications and intraoperative blood loss, and shorten the duration of surgery.
Introduction
Laparoscopic cholecystectomy (LC) has become the standard surgical treatment for patients with symptomatic cholecystolithiasis and today it is one of the most frequently performed procedures in general surgery. But bile duct injury (BDI) is still a rare but with severe and persistent complication. 1 Especially in the difficult gallbladder, the intraoperative abdominal adhesion is severe, and the local anatomy of the Calot's triangle is not precise. According to Ashfaq's report, 2 a “difficult gallbladder” is necrotic or gangrenous, has Mirizzi syndrome, has extensive adhesions, required conversion to laparotomy, the operation lasted >120 minutes, had prior tube cholecystostomy, or had known gallbladder perforation. So, how to show the anatomical structure of the bile duct clearly during the operation becomes the key to avoiding iatrogenic BDI.
Intraoperative cholangiography (IOC) is a standard method for developing the biliary structure. However, there is no robust evidence supporting the routine use of IOC to prevent BDI, such as using a C-arm X-ray machine during the operation will prolong the operation time; increasing the X-ray exposure of patients and medical staff; the cost is high, and the process of cystic duct intubation may also bring risks such as BDI.3–7
Indocyanine green (ICG) is a relatively safe fluorescent contrast agent, mainly metabolized in the liver. It is excreted through the biliary tract with a short half-life. It is widely used in various surgical operations, for patients with gastric cancer, ICG-navigated lymphadenectomy increases the number of lymph nodes retrieved. 8 ICG is also used to locate sentinel lymph nodes in breast cancer. 9 Scholars have divided the uses of ICG in hepatobiliary surgery into four categories: liver mapping, cholangiography, tumor visualization, and evaluation of partial liver grafts.10,11
Compared with IOC, ICG fluorescence can improve visualization and provide a detailed anatomical mapping of the biliary structures. 12 In most articles about ICG fluorescent cholangiography, ICG is injected intravenously. The background fluorescence of the liver can interfere with optimal viewing of the extrahepatic biliary structures, especially in difficult LC. In this study, patients who underwent percutaneous transhepatic cholecystic catheter drainage (PTGBD) were directly injected ICG through the catheter during the operation, and ICG-guided fluorescence cholangiography was performed to improve the visualization of the bile duct. It effectively avoids the fluorescence interference of the liver and indicates the biliary structure. The report is as follows.
Materials and Methods
Ethical statement
This study was approved by the Institutional Review Board, under authorization No. 2018001-04.
Patients
We reviewed patients who underwent elective laparoscopic biliary surgery after PTGBD for difficult gallbladder from January 2017 to August 2022 at Hangzhou Hospital of Traditional Chinese Medicine, affiliated to Zhejiang Chinese Medicine University. The criteria for selecting patients with difficult gallbladder were as follows: patients diagnosed with acute cholecystitis Grade II or III according to 2018 Tokyo Guidelines (TG18) and are unable to undergo emergency surgery,13,14 with or without Mirizzi syndrome, and extensive adhesions because of previous upper laparotomy, so that the PTGBD tube was positioned. According to whether ICG or fluorescent laparoscopy were used intraoperatively, they were divided into the ICG group (18 cases in total, including 16 cases of fluorescent LC and 2 cases of fluorescent LC plus laparoscopic common bile duct exploration [LC+LCBDE]) and WL group (20 cases in total, all under white light, including 16 cases of LC, 1 case of LSC, and 3 cases of LC+LCBDE).
Intraoperative fluorescence imaging with ICG
Indocyanine green for injection produced by Dandong Yichuang Pharmaceutical Co., Ltd, 25 mg/bottle, was diluted with 10 mL water for sterilizing injection and PINPOINT Laparoscopic fluorescence imaging System (PINPOINT Imaging System; Novadaq, Canada) was used.
Operative technique
In the ICG group, after induction of general anesthesia, pneumoperitoneum and observation hole were established through the umbilical foramen, and then ICG 3 mL was directly injected into the PTGBD tube. Under fluorescence, the Calot's triangle was carefully separated with an electric hook and an attractor, and the cystic canal and cystic artery were clipped. Gradually the gallbladder bed was separated from the PTGBD tube; and an assistant extracted it in vitro. If patients were diagnosed with CBD stone preoperatively, LCBDE should be continued. Intraoperatively, the puncture site of the liver was found to adhere to the abdominal wall in most patients, and a local sinus tract was formed. After removing the PTGBD tube, the sinus opening is treated with an electric coagulation hook or Prolene wire if no sinus tract has formed. The surgical area was carefully rinsed to check that there was no local bleeding or bile leakage.
In the WL group (the case of LSC), the patient was complicated with liver abscess, and percutaneous catheter drainage was carried out. During the operation, severe adhesion and edema around the gallbladder were found. Dissection of the Calot's triangle to obtain a critical view was unsafe, so the surgeon decided to perform the LSC under white light. Separating adhesions to expose the gallbladder, opening the Hartmann's pouch, aspirating the bile, and extracting all stones into a collecting bag were the basic steps in the procedure. Then an electric hook was used to circumferentially transect the gallbladder neck, and a gallbladder fistula tube was inserted into the remaining gallbladder. The remaining part was closed with sutures to form residual gallbladder. In the subhepatic fossa, a drainage tube was implanted. Finally, the collection bag was removed through a 10 mm umbilical port. The remaining 19 cases underwent conventional LC with or without LCBDE under white light according to their preoperative diagnosis. The timing of PTGBD tube removal in all patients was the same as in the ICG group.
Objectives
The conversion to laparotomy rate, intraoperative blood loss, operation duration, surgery cost, hospitalization cost, postoperative hospital stay, and surgery-related complications were compared between the two groups.
Statistical analysis
IBM SPSS Statistics 26.0 (Armonk, NY) was used to perform the statistical analysis. All variables were expressed as mean ± standard deviation. Categorical variables were compared using the chi-squared test, and continuous variables were compared using the parametric t-test. A value of P < 0.05 was considered statistically significant.
The study was approved by the Institutional Review Board, under authorization No. 2018001-04, and conducted in the Department of General Surgery, Hangzhou Hospital of Traditional Chinese Medicine, affiliated to Zhejiang Chinese Medicine University.
Results
A total of 38 patients were enrolled in the study. The ICG group consisted of 18 patients and the WL group of 20 patients, with a mean age of 64.7 ± 15.5 years in the ICG group and 62.6 ± 15.0 years in the WL group (P = .679). All preoperative data (i.e., sex, height, weight, body mass index, and previous abdominal surgery) resulted in homogeneity between the two groups (Table 1). All patients were not allergic to ICG, had no heart, lung, or liver insufficiency, no coagulation disturbance, and were tolerant of general anesthesia.
Patients' Demographics
Data are presented as n (%) or mean ± standard deviation.
BMI, body mass index; ICG, indocyanine green; WL, white light.
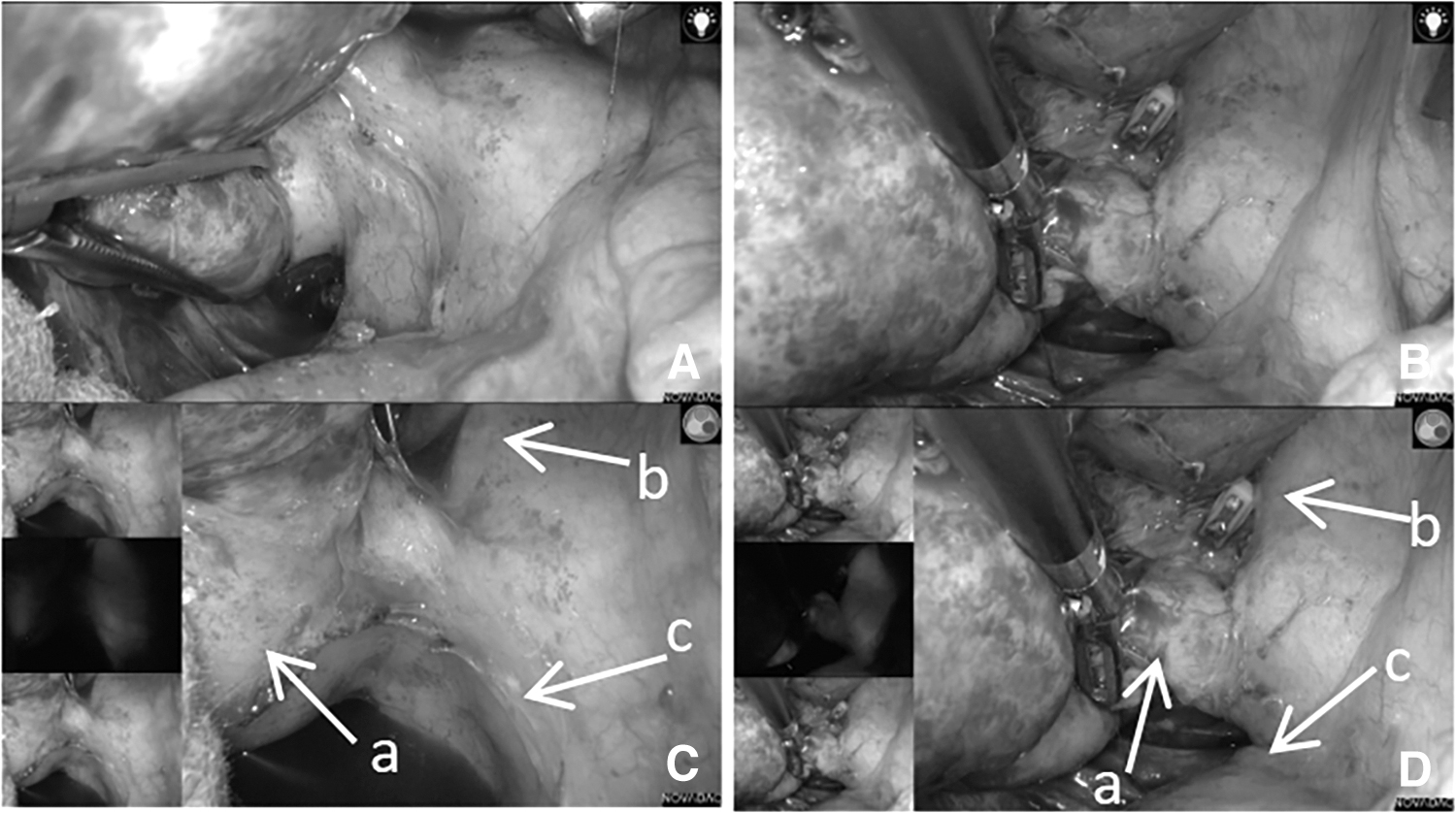
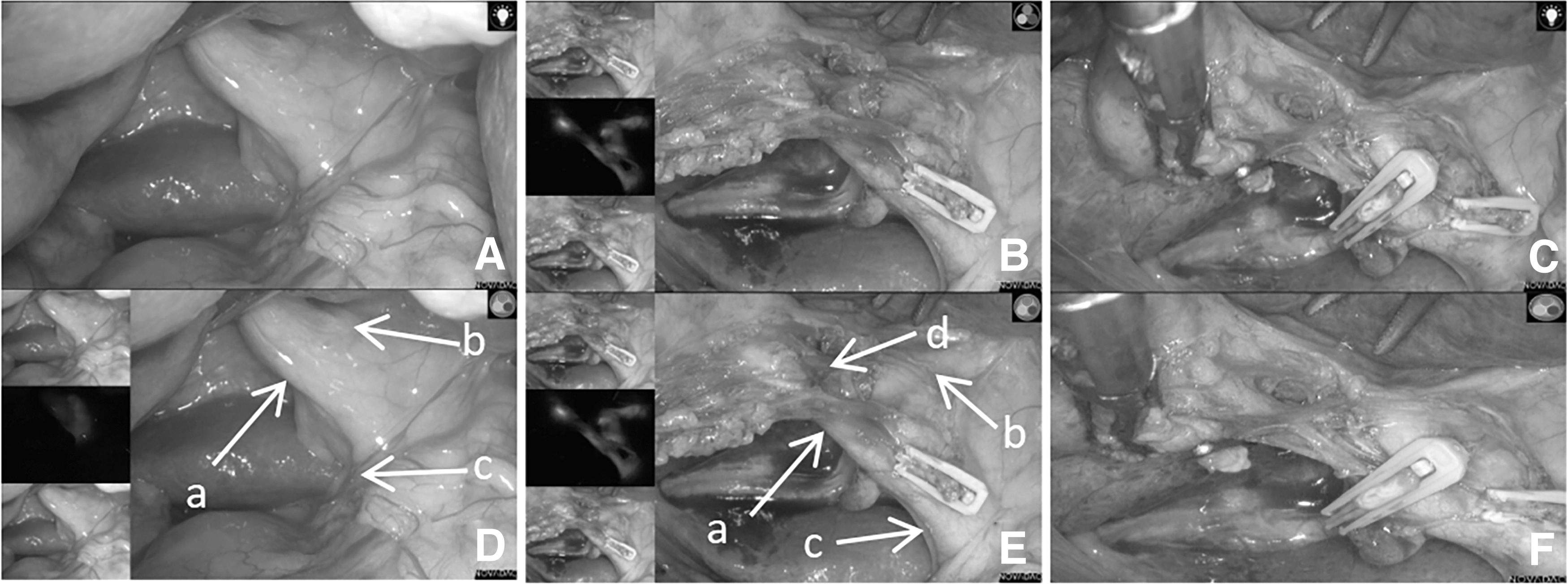
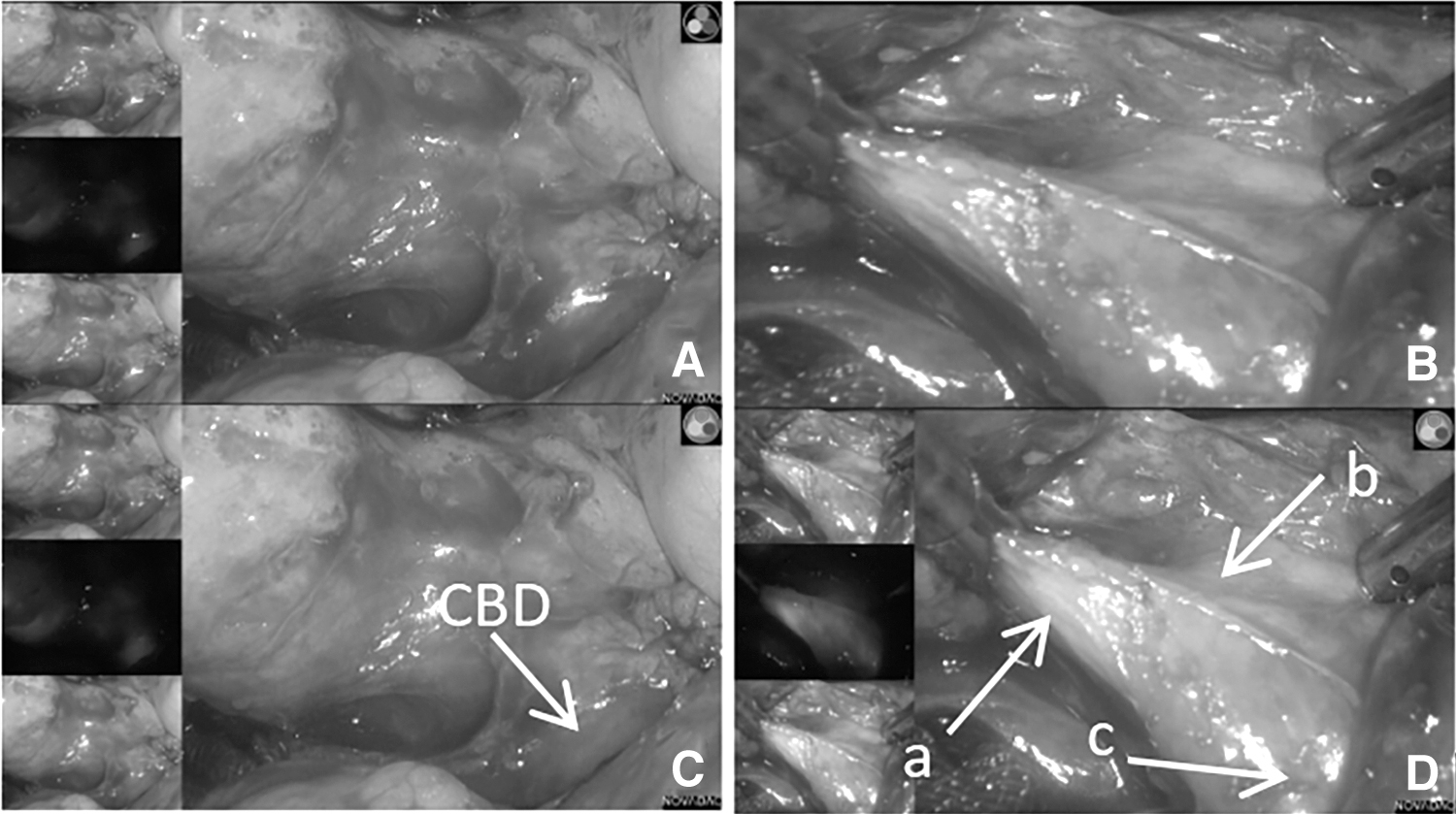
ICG group were all injected ICG through a PTGBD tube. After direct injection of ICG through the catheter, images of the biliary system can be seen in fluorescence mode. Compared with the white light method, fluorescence mode provides a clearer biliary anatomic development in cases of severe intraperitoneal adhesion. Hartmann's sac can be immediately observed and used as a safety indicator for intraoperative anatomy. After the separation of adhesions under the guidance of fluorescence mode, the confluence of the entire bile duct and CBD can be seen. After further dissection, the anatomical structure of the cystic duct, common hepatic duct, and CBD were observed (Figs. 1–4). None of the 18 patients had iatrogenic BDI, no conversion to laparotomy, no postoperative biliary leakage, abdominal infection, and other complications.
Examples of biliary anatomy visualization using WL
Examples of biliary anatomy visualization using WL

Examples of biliary anatomy visualization using WL
Examples of biliary anatomy visualization using WL
Owing to severe gallbladder inflammation and lack of ICG assistance, 20 patients in the WL group could not identify the cystic duct, CBD, and common liver duct as quickly as the ICG group. There was no conversion to laparotomy in the WL group. Still, there were 3 cases of surgery-related complications, 1 case had biliary leakage combined with Klebsiella pneumoniae infection, 1 patient developed fever 10 days after discharge and was hospitalized again, 1 patient developed cystic fossa effusion and Enterococcus faecium infection after surgery, and all the 3 patients were eventually cured and discharged.
There were no surgery-related complications in the ICG group, whereas there were 15% in the WL group, but there was no significant difference between the two groups (P = .232). Intraoperative blood loss was 10.0 ± 3.0 mL in the ICG group and 18.5 ± 10.6 mL in the WL group, which was statistically significant (P = .002). The operation duration was 85.9 ± 35.7 minutes in the ICG group and 126.6 ± 50.1 minutes in the WL group, which had a statistical difference (P = .006). The mean postoperative discharge time was not significantly different between the two groups (5.9 ± 3.3 days versus 9.2 ± 7.0 days, P = .074; Table 2).
Surgical Outcomes
Data are presented as n (%) or mean ± standard deviation.
ICG, indocyanine green; WL, white light.
Discussion
LC is the standard gold treatment for symptomatic cholelithiasis. LC can be fractious, even for experienced surgeons, when severe fibrosis and sclerosis at the Calot's triangle prohibit safe surgical dissection. It is reported that the incidence of BDI during LC is 0.08%–0.4%,15–17 but in the difficult gallbladder it is 16%. 18 PTGBD is traditionally regarded as a safe and effective operation for acute cholecystitis. The Tokyo Guidelines 2018 recommend it as a standard gallbladder drainage method for critically ill patients or patients who cannot receive emergency LC. 14 Some studies have shown various surgical difficulties in LC after PTGBD, including a high conversion rate to laparotomy, long operation time, and a large amount of blood loss during operation. 19 Most of the patients in this study are of advanced age, poor general condition, recurrent cholecystitis, severe edema, and adhesion around the gallbladder.
Patients with acute cholecystitis who take anticoagulants for a long time are usually elderly or complicated with cardio-cerebrovascular diseases. There is still a greater risk of emergency LC under general anesthesia, and there is a greater possibility of conversion to laparotomy. In contrast, the risk of trauma and bleeding in emergency PTGBD is relatively tiny. After the publication of the guidelines, delayed LC after PTGBD was reported to produce better outcomes than emergent LC.20,21 Our center placed the PTGBD tube for >4 weeks, to reduce the pressure of the biliary tract, reduce the inflammation and edema around the gallbladder, making it easier to directly illuminate the bile duct, thus reducing the time of intraoperative dissection of peripheral adhesion, reducing intraoperative bleeding, and reducing the incidence of intraoperative BDI.
In this study, the extrahepatic biliary system was successfully developed by trans-PTGBD ICG injection, reducing the operation difficulty. After injection, the gallbladder was first developed. Owing to the relatively low anatomic position of the gallbladder ampulla and cystic duct, the fluorescence intensity of the gallbladder ampulla and cystic duct increased gradually. In the difficult laparoscopic biliary surgery with severe biliary adhesion and unclear anatomy, good development of anatomical signs can significantly shorten the duration of surgery, and reduce intraoperative blood loss and the risk of biliary tract injury. The average time of surgery in the WL group was 126.6 minutes, similar to what Ashfaq considered “difficult gallbladder” surgery to be >120 minutes. In comparison, in the ICG group, it was 87.4 minutes, significantly shorter. 2 This proves that the ICG injection through the PTGBD tube can help quickly identify the Calot's triangle during surgery and complete the operation.
There is no need to worry about the effect of ICG on the liver function of the patients. The precise time of fluorescein imaging during the operation can be prolonged by changing the patient's position after injection or adding a small amount of ICG through the catheter. Because ICG directly enters the bile duct, the cystic artery will not be developed. Therefore, the cystic artery and the cystic duct can be indirectly distinguished under fluorescence light (Figs. 2 and 3). They will be clipped with absorbable clips and cut with scissors, reducing intraoperative bleeding. So it was demonstrated that the intraoperative blood loss in the ICG group is less than that in the WL group.
ICG is a relatively safe dye, which can show fluorescence after being processed by a particular receiving device. It has been reported that the risk of adverse reactions to ICG injection is minimal, mainly when the injection dose is >0.5 mg/kg, which is ∼0.003%. 22 In this study, the concentration of ICG injection was 2.5 mg/mL, and 3–5 mL was generally injected. This dose is far less than the dose range of adverse reactions. The application of ICG in LC is still inconclusive. Studies have reported that preoperative injection from the elbow vein can obtain good liver and biliary tract.23,24 But owing to the accumulation of the liver during the operation, the fluorescence imaging of the gallbladder and biliary tract is affected by liver fluorescence. This narrows the recognition of Calot's triangle and biliary anatomy, especially when the Calot's triangle and surrounding tissues and organs are densely adhered; the liver's interference is more prominent.
There are also reports of successful cases of intraoperative ICG injection through the gallbladder, but some patients also have leakage of ICG at the puncture point.25,26 In the case of fluorophore leakage, all observations and estimations were biased and unreliable. In this study, ICG was injected directly into the gallbladder through a catheter during the operation, which can perform real-time fluorescence imaging of the biliary tract safely and conveniently. It can avoid the interference of liver fluorescence background effectively.
In other centers, subtotal cholecystectomy is performed for the difficult gallbladder to avoid BDI. 27 When the Calot's triangle's structures cannot be recognized and the crucial sight of safety cannot be attained, LSC removes some of the difficult gallbladder. Still, this technique has a high incidence of postoperative complications, including bile leakage, residual stones, recurrent symptoms of gallstones, and reoperation.28–30 The most common complication was postoperative bile leak, which occurred in 10.6% of patients, according to Henneman D's systematic review. 30
What's more, if subtotal cholecystectomy needs secondary surgery, it would increase the likelihood of adhesiolysis, bile duct exploration, and intensive care unit admission and may require conversion to an open procedure. 31 In our study, there were no postoperative problems with the LSC and no need for additional surgery. The entire gallbladder was removed in the ICG group, all procedures were successful, no intraoperative or postoperative complications occurred, and no secondary surgery was performed. In the WL group, there were 15% (3/20) more surgery-related complications than in the ICG group, but the difference was not statistically significant, which was similar to Jin H's study. 32
As is known, fluorescent cholangiography has not been shown to identify CBD stones effectively. Therefore, it should not substitute for traditional contrast X-ray cholangiography in cases concerned with CBD obstruction. All 5 choledocholithiasis patients had acute cholecystitis as their primary clinical symptom. For at least one of the following reasons, these patients were not suitable for endoscopic retrograde cholangiopancreatography (ERCP): large bile duct stones (diameter >15 mm), intrahepatic bile duct stones, bile duct stones for which imaging could not confirm, duodenal diverticulum, or esophageal-gastric varices. However, PTGBD can reduce the pressure in the biliary system, alleviate the patient's discomfort, and reduce local inflammation. LCBDE plus cholecystectomy, as opposed to ERCP plus LC for choledocholithiasis, can protect the Oddi's sphincter to prevent reflux of duodenal contents. 33
In our center, holmium laser lithotripsy can be used to treat CBD stones that is big or impacted. 34 So we chose the single-stage laparoscopic bile duct clearance. There were no surgery-related complications in both groups. The duration of cholecystectomy in the ICG group was shorter than WL group, but fluorescence had no advantage in the treatment of common bile duct stones.
Conclusions
We believe that ICG fluorescence cholangiography has good clinical value in difficult gallbladder. Intraoperative ICG fluorescence cholangiography can significantly improve the visualization of bile duct structure, avoid iatrogenic BDI, reduce surgery-related complications and intraoperative blood loss, and shorten the duration of surgery.
Footnotes
Acknowledgment
The authors thank the operation team involved in the surgical field of Hangzhou Hospital of Traditional Chinese Medicine, affiliated to Zhejiang Chinese Medicine University.
Authors' Contributions
H.H.: Conceptualization, Funding acquisition, Supervision, Writing—review and editing.
D.D.: Methodology, Data curation, Data analysis, Writing—original draft.
Z.W.: Methodology, Writing—original draft.
Y.X.: Data curation, Data analysis.
Z.N.: Data interpretation, Literature search.
X.L.: Data interpretation, Literature search.
H.J.: Literature search.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by a grant from the Natural Science Foundation of Zhejiang Provincial (Grant No.2021KY927).