
Abstract
Background:
The purpose of this study is to compare the efficacy and safety of extracorporeal shockwave lithotripsy (SWL), retrograde intrarenal surgery (RIRS), mini-percutaneous nephrolithotomy (mPNL), and standard-percutaneous nephrolithotomy (stPNL) for the treatment of 20–30 mm kidney stones.
Methods:
The records of 1197 patients (SWL = 149, RIRS = 205, mPNL = 525, and stPNL = 318) from 8 centers were reviewed retrospectively. Four procedures were compared for stone-free rates (SFRs), auxiliary treatment, and associated complications.
Results:
Initial SFRs were 43.6%, 54.6%, 86.7%, and 87.7% in SWL, RIRS, mPNL, and stPNL, respectively (P < .001), whereas the final SFRs were 71.8%, 80%, 90.5%, and 89.6% (P < .001). The rate of auxiliary treatment in the groups was 38.3%, 26.8%, 5%, and 4.4%, respectively (P < .001). The initial and final SFRs in the mPNL and stPNL groups were higher than those in SWL and RIRS groups (P < .001). The rate for auxiliary treatment was lower in the mPNL and stPNL groups (P < .001). The operation time was longer in the RIRS group (P = .005). According to the Clavien–Dindo classification, the complication rate in the SWL group was lower than that in the surgical approaches (P < .001); however, no statistical difference was detected between RIRS, mPNL, and stPNL groups. mPNL and stPNL had a higher success rate than RIRS or SWL for treating 20–30 mm kidney stones.
Conclusion:
In the treatment of 2–3 cm renal stones, RIRS and PNL were more effective than SWL to obtain a better SFR and less auxiliary treatment rate. Compared with RIRS, mPNL and stPNL provided a higher SFR with similar complication rates.
Introduction
Urolithiasis is the most common urological disease worldwide. Its prevalence varies between 1% and 20% depending on demographic changes. 1 Current treatment options include three procedures: extracorporeal shockwave lithotripsy (SWL), retrograde intrarenal surgery (RIRS), and percutaneous nephrolithotomy (PNL). Currently, European Urology Guidelines recommend PNL as first-line therapy for kidney stones >20 mm, while RIRS and SWL are considered second-line therapy. 2
SWL, which dates back to the 1980s, has the advantages of noninvasiveness, ease of use, low complication rates, low cost, and minimal or no anesthesia requirement; however, it is associated with a lower stone-free rate (SFR) and higher auxiliary treatment rate. 3 As a treatment choice, RIRS finds itself between PNL and SWL regarding treatment effectiveness and safety.
The functional developments of flexible ureteroscopes, disposable endourological surgical equipment, and lasers have led RIRS to become an effective surgical technique for larger (>20 mm) renal stones. 4 PNL is considered the “gold standard” treatment for renal stones >2 cm, with a success rate of >90%. 2 PNL complications are generally related to tract size. It has been reported that mini-PNL (mPNL; <20 Fr) with smaller tracts can be applied instead of standard-percutaneous nephrolithotomy (stPNL; >20 Fr) in clinical practice to reduce the complications of PNL. 5
Although there have been studies comparing SWL, RIRS, mPNL, and stPNL procedures for <20 mm stones before,3,6 studies comparing the four approaches for larger stones (>20 mm) are limited. This study aims to compare the success and complication rates of SWL, RIRS, mPNL, and stPNL for kidney stones between 20 and 30 mm in size.
Materials and Methods
Data of patients who underwent SWL, RIRS, mPNL, or stPNL for treatment of kidney stones with a size of 2–3 cm in 8 centers between January 2019 and December 2021 were analyzed retrospectively. Patients with congenital kidney and urinary tract anomalies and pediatric or pregnant patients were excluded from the study. The local ethical committee approved this study (the local ethical committee's registration number is 2022/306).
Patients were preoperatively tested, such as through routine laboratory work-up and imaging. In addition, any urinary tract infection with a positive urine culture was treated concerning the antibiogram. Intravenous second- or third-generation cephalosporins were applied as antibiotic prophylaxis during the induction of anesthesia.
Pretreatment stone size and location were assessed by computed tomography (CT) scan. Stone size was assigned by calculating the longest axis of the kidney stone visible on the CT scan. In cases with multiple stones, the sum of the diameters of all stones constituted the stone size. The preoperative parameters recorded for each patient were as follows: age, gender, body mass index (BMI), stone characteristics (stone size, opacity, density, side, and location), hydronephrosis grade, previous stone surgery, and preoperative JJ stent placement.
We recorded intra- and postoperative parameters, including hemoglobin (Hb) decrease, Cre change, operative time, initial stone-free status, auxiliary treatment, and final stone-free status. The choice of treatment modality depended on the patient's or surgeon's preference. Postoperative complications were assessed using the Clavien–Dindo grading system.
The piezoelectric lithotripter (Wolf PiezoLith 3000 Richard Wolf GmBH, Knittlingen, Germany) device was used in all SWL patients. Ureteral access sheath placement (UAS) failed in some cases of RIRS. In these cases, the ureteral orifice was dilated with a balloon dilating catheter. The ureterorenoscope was passed over the guidewire when dilation failed. The devices used during the RIRS were Medilas H Solvo (Dornier MedTech, Wessling, Germany) (30 W), VersaPulse PowerSuite P20 (Lumenis, San Jose, CA) (20 W), and Litho (Quanta System, Milan, Italy) (30 W).
Dust or chipping techniques were applied with Holmium: YAG laser (Ho: YAG) according to the characteristics of the stone and the surgeon's preference. The power of the holmium laser was set at 10–15 W to 0.4–1.5 J and 5–20 Hz. When applying the dusting technique, power was maintained by increasing the speed and lowering the frequency. During RIRS, dusting and chipping techniques were performed with a laser setting of 0.4–0.6 J × 20 Hz and 1–1.5 J × 8–10 Hz, respectively.
Laser settings in mPNL were generally 1.5–2 J to 10 Hz. For tract dilatation, depending on availability, balloon dilators, metal, or amplatz up to 20 Fr- (≤20 Fr) were used in mPNL. Ho: YAG laser was used for stone fragmentation. Generally, 24 Fr, less frequently, 26 Fr Amplatz dilators were used in stPNL for tract dilatation. Fragmentation of the stone was accomplished using a pneumatic, ultrasonic, or combined pneumatic–ultrasonic lithotripter. All mPNL cases were performed in the supine position, and stPNL cases were performed in the prone position.
The success rate after the intervention was assessed by stone-free and freedom from reintervention rates. We set initial SFRs for each treatment method as the primary endpoint. All patients were evaluated with noncontrast CT at 1 month postoperatively. Procedure success was defined as stone free or the presence of ≤4 mm fragments. Auxiliary treatment for residual stones was recorded during follow-up. Auxiliary treatment rates and final SFRs were chosen as the secondary endpoint.
All statistical analyses were performed with SPSS 25.0.0.1 software (IBM Corp., Armonk, NY). The one-way analysis of variance followed by Bonferroni's post hoc test, the Kruskal–Wallis test, the Mann–Whitney U, and chi-squared tests was used to compare treatment modalities. The normal distribution assumption for continuous variables was analyzed with the Shapiro–Wilk test. A value of P < .05 was considered statistically significant.
Results
Demographic and operative outcomes
Of the 1197 patients included in our study, SWL was performed in 149 (12.4%) patients, RIRS was performed in 205 (17.1%) patients, mPNL was performed in 525 (43.9%) patients, and 318 (26.6%) patients underwent stPNL. The study population comprised of 669 males (55.9%) and 528 females (44.1%). The mean age of the patients was 49.8 ± 13.9. Clinical and operative characteristics of the patients concerning treatment groups are summarized in Table 1.
Demographic and Clinical Data of the Patients with Respect to Treatment Arms
BMI, body mass index; Hb, hemoglobin; mPNL, mini-percutaneous nephrolithotomy; RIRS, retrograde intrarenal surgery; stPNL, standard-percutaneous nephrolithotomy; SWL, extracorporeal shockwave lithotripsy.
Patients in each group were similar in age, gender, BMI, stone characteristics (except for density), hydronephrosis grade, and previous stone surgery; preoperative JJ stent placement was more prevalent in SWL and RIRS groups (P < .001). The mean stone size was 23.7 ± 3.2 mm, 23.8 ± 3.4 mm, 24 ± 3.5 mm, and 24.1 ± 3.2 mm, respectively, with no significant difference (P = .479).
In the SWL group, 7.4% of patients underwent pre-SWL JJ ureteric stenting. The mean number of sessions per stone was 3.4 ± 1.1. UAS was used in 182/205 (88.8%) of RIRS cases. Operation time for the RIRS group was significantly longer than that for mPNL- and stPNL-treated patients (P = .005). The Hb decrease of SWL, RIRS, mPNL, and stPNL patients was 0.1 ± 0.2, 0.3 ± 0.6, 1.1 ± 0.8, and 1.4 ± 0.7, respectively (P = .001). The increase in creatinine was higher in stPNL patients than in SWL and RIRS patients (P = .003).
Success rates
The initial SFRs were 43.6%, 54.6%, 86.7%, and 87.7% in SWL, RIRS, mPNL, and stPNL, respectively (P < .001). However, the retreatment rate for auxiliary procedures was significantly less in those patients undergoing mPNL and stPNL than in those undergoing SWL and RIRS treatment (P < .001). The rates of auxiliary treatments applied after primary treatment approaches are demonstrated in Figure 1. RIRS was the most common auxiliary treatment in all four groups. The final SFRs after auxiliary procedures were 71.8%, 80%, 90.5%, and 89.6% in SWL, RIRS, mPNL, and stPNL, respectively (P < .001). Overall, initial and final SFRs were lower, and auxiliary treatment rates were higher in the SWL and RIRS groups (Table 2). There was no statistical difference between the mPNL and stPNL groups regarding SFRs and the need for auxiliary treatment.
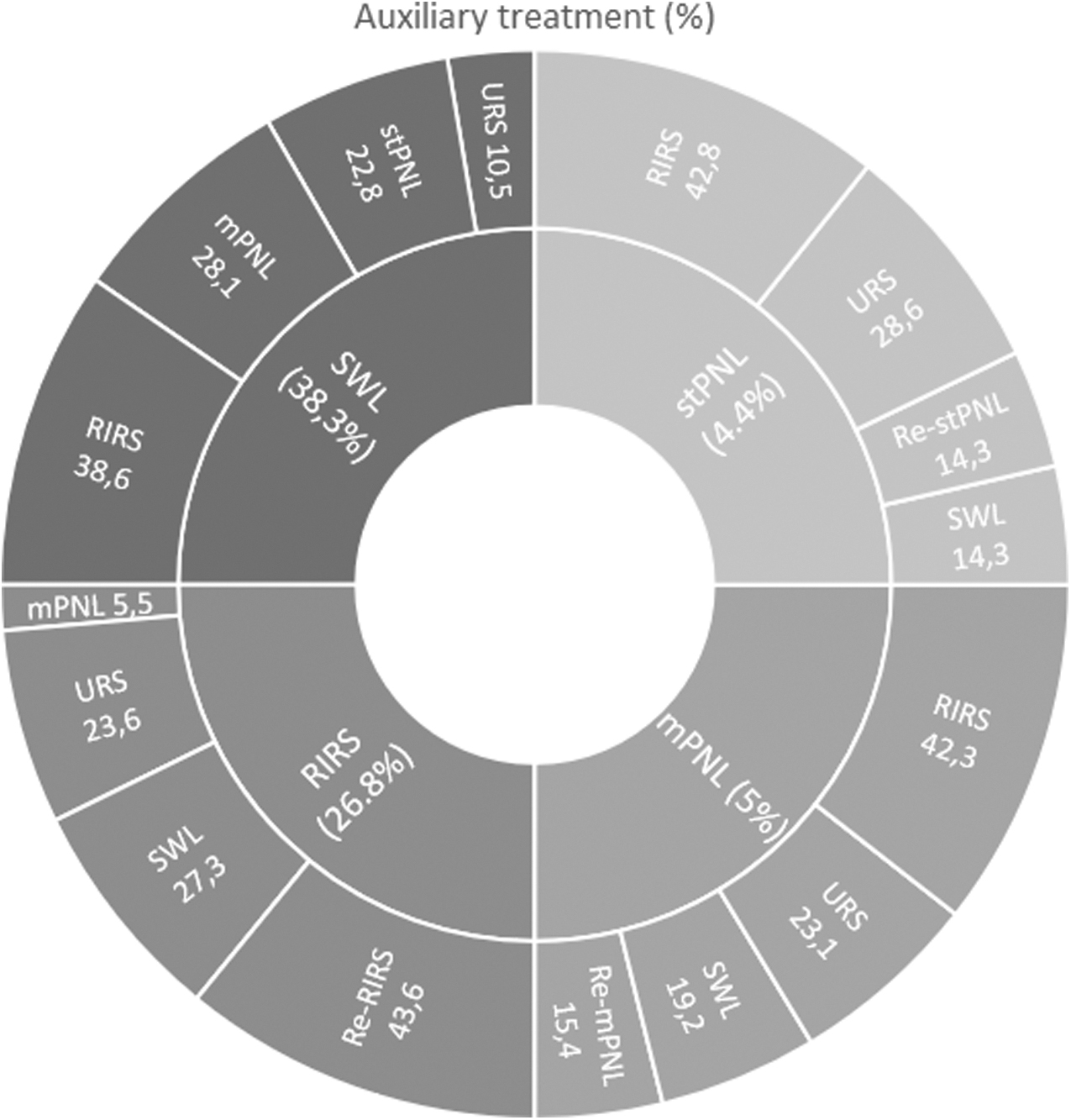
The distribution of patients according to auxiliary treatment. mPNL, mini-percutaneous nephrolithotomy; RIRS, retrograde intrarenal surgery; stPNL, standard-percutaneous nephrolithotomy; SWL, extracorporeal shockwave lithotripsy.
Results and Complications for Bonferroni-Corrected Post Hoc Tests
Hb, hemoglobin; mPNL, mini-percutaneous nephrolithotomy; RIRS, retrograde intrarenal surgery; stPNL, standard-percutaneous nephrolithotomy; SWL, extracorporeal shockwave lithotripsy.
Complication rates
The complication rates for all approaches were also higher compared with SWL. Overall complications were observed among 8 (5.4%) patients in SWL group, 39 (19%) patients in RIRS group, 89 (17%) patients in mPNL group, and 58 (18.2%) in stPNL group (P = .002) (Table 2).
Discussion
Although the successful and safe management of moderate-sized calculi (1–2 cm) has been well established with clear indications, optimal treatment of larger renal stones (>2 cm) continues to constitute a challenge for practising endourologists. Related to this issue, although PNL has been effectively applied as the preferred treatment modality for these stones in all parts of the world, not all patients are suitable for the percutaneous approach.
Despite its highly effective outcomes, particularly in one session, the more invasive nature of the percutaneous approach with well-known possible severe complications such as bleeding and infection constituted significant disadvantages due to safety concerns. As a result, the miniaturization concept gained popularity, resulting in the widespread use of less invasive smaller access sheaths and instruments.
Management of larger stones with standard large track sized (20–30 Fr) PNL provided significantly higher SFRs in a single session when compared with other modalities such as SWL and RIRS.7,8 However, associated morbidities have led endourologists to seek alternative treatment options with less morbidity. Following the clinical introduction of “Miniaturization” in endourology, urologists aimed to achieve similar success rates with reduced complications. It was thought that the complication rates might decrease with the decrease in dilatation diameter. For this purpose, small-sized instruments have been used through smaller diameter sheaths to reduce the size of the damage in the kidney parenchyma.
Accordingly, suitable sizes of various endoscopes have been used for stone disintegration and removal with the access sheaths sizing from 11 to 20 Fr in minimally invasive percutaneous approach.9,10 Although miniaturized systems have been used in the management of smaller stones in the beginning, based on the safe and practical application, the mPNL technique began to be applied in larger and multiple calculi with successful and safe outcomes.11,12
mPNL procedure can establish similar SFRs with stPNL while decreasing the complication rates. 13 Our study found no difference in mPNL compared with stPNL in terms of initial and final stone-free status, need for additional treatment, and complication rates. However, it was noteworthy that Clavien grade 3–4 complications were higher in stPNL. Similar to our study, Zeng et al stated that mPNL could achieve noninferior SFR outcomes with fewer complication rates than stPNL. 11 Conversely, Elsheemy et al reported that there was a significant difference in favor of stPNL in SFR in multiple stones or large stone burden (>2 cm2). 14
On the contrary, based on the above-mentioned safety-based limitations of PNL, together with technological advances and the increasing experience in clinical practice, “Flexible ureteroscopy (fURS)” has been used as a valuable alternative in the management of upper urinary tract stones with its more effective and safer outcomes. RIRS was recommended as a primary option for stones <2 cm by the EAU guidelines. 2 However, nowadays, it can also be used to treat larger stones with the advancements in the technology of scopes, lasers, and disposables.15,16
Despite comparable stone-free and complication rates, particularly in medium-sized stones (<20 mm), published data have demonstrated relatively low SFRs along with the need for additional sessions for RIRS compared with PCNL for larger (>20 mm) calculi. 17 Breda and colleagues reported an SFR of 93% after an average of 2.3 sessions of RIRS for single intrarenal stones with a diameter of 20–25 mm. 18 Considering SWL and RIRS failures in symptomatic lower pole stones, super-mini percutaneous nephrolithotomy (SMP) may be a safe and efficient auxiliary option after these methods. 19
Moreover, holmium laser lithotripsy's effective and safe utilization yielded better outcomes than SWL for moderate-sized kidney stones (10–20 mm). 6 However, studies focusing on the management of larger stones (>20 mm) with RIRS monotherapy did clearly show that SFRs will depend on the operator's experience, which may require staged procedures.20,21 Last but not least, SWL has also been applied for stones >20 mm and although limited, reported data in the literature revealed significantly lower SFRs after the application of several sessions. 22
Higher energy settings and lower frequency settings [(0.6–1 J) × (6–15 Hz)] are commonly used for fragmentation. Baskets are frequently required to remove calculi after fragmentation. Dusting is a technique that uses lower energy settings and higher frequency settings [(0.2–0.4 J) × (50–80 Hz)]. Dusting does not leave large calculi behind and avoids the need of basket usage. 23 Another study demonstrated that dusting reduced laser fiber tip degradation and stone retropulsion. 24 Besides, although it is advocated that “Moses effect” technology reduces stone retropulsion, solid clinical evidence of actual improvement in surgical outcomes is still missing. 25
The Thulium Fiber Laser (TFL) offers an alternative laser energy source to the Holmium laser. TFL appears to be a more effective treatment option with similar safety in RIRS and PNL compared with holmium laser.26,27 However, this is still a controversial topic today.
SWL is a valuable option available to manage kidney stones. The primary purpose of managing urinary system stones is to minimize the associated complications by leaving no residual fragments. Limitation of SWL procedure is the possibility of potential residual fragments causing adverse clinical outcomes. However, despite the lower SFR and higher retreatment rates, SWL remains a treatment option for urinary tract stones due to its noninvasive nature. The overall success of SWL in the literature is variable, and ranges from 46% to 91%.
Although the success rate after a single session is related to stone and patient-related parameters, it is low. The average number of sessions required for the stone-free treatment ranges from 1.6 to 2.2.28,29 In our patients, the initial SFR was 43.6%, with a mean of 3.4 SWL sessions after SWL. This rate was significantly lower than that for surgical approaches.
Nowadays, SFR is an important target in managing renal stone disease, and the surgical method to be selected for kidney stone treatment depends primarily on stone size and localization. When treating kidney stones with SWL, it is known that SFRs depend upon stone burden, varied characteristics of the stone and patient, and preoperative renal anatomy. 28 Khalil et al 22 reported that SFRs of <1 cm, 1.1–2 cm, and >2 cm stones in patients undergoing SWL were 50.2%, 39.6%, and 10.2%. The authors also noted that the number of SWL sessions increased with increasing stone size and density.22,29
In 2018, Waqas and colleagues 30 divided patients with kidney stones (stones between 5 and 20 millimeters) into three groups based on Hounsfield units (a measure of density on CT scans). These groups were: less than 500 HU, 500 to 1000 HU, and greater than 1000 HU, and they had success rates of 93.8%, 62.7%, and 24.5% respectively. The researchers also found that the stone's attenuation value, the skin-to-stone distance, and the location of the stone were all independent factors that could predict the success rate of the treatment.
The major drawback of our trial is its retrospective nature. However, considering the limited number of comparative studies on the four minimally invasive treatments of 20–30 mm kidney stones, we believe that our findings will contribute enough to the existing knowledge in the literature.
Conclusion
In this study, we aimed to evaluate the efficacy of different treatment alternatives (SWL, RIRS, mPNL, and stPNL) in managing relatively large (20–30 mm) stones. Our results demonstrated that when compared with SWL and RIRS, mPNL and stPNL showed significantly better treatment outcomes regarding higher stone-free and fewer reintervention rates.
Footnotes
Ethical Approval
This is a retrospective analysis based on electronic medical record data obtained from several centers in Turkey. According to the requirements of the ethics committee of Ankara University, informed consent can be exempted after the anonymization of medical record data.
Data Availability
All datasets used and analyzed during this study are available from the corresponding author on reasonable request.
Authors' Contributions
K.S. and B.B. contributed to protocol/project development and data analysis. M.A.I., M.A.K., and Y.Y. assisted with data collection or management, article writing/editing. S.G. carried out article writing/editing. T.T. and S.V. contributed to data analysis, data collection or management. M.I.G. assisted with protocol/project development and article writing/editing. M.C.K. contributed to protocol/project development, data collection or management. M.B. and O.G. performed data collection or management. C.S. assisted with protocol/project development. All authors read and approved the final version of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.