
Abstract
Background:
Lateral lymph node dissection (LLND) is an effective treatment for metastatic lateral lymph nodes (LLNs) in lower rectal cancer, but with high complication rates due to a complicated procedure. This study aimed to introduce a new technique for LLND based on membrane anatomy to simplify the procedure and report short-term outcomes.
Methods:
Twenty-three patients with clinical stage II-III lower rectal cancer underwent three-dimensional (3D) laparoscopic total mesorectal excision (TME) plus LLND between July 2018 and December 2020. Demographic data, perioperative variables, and oncologic outcomes were recorded and analyzed. Complications were graded using the Clavien-Dindo (CD) score.
Results:
Based on the theory of “four fasciae and three spaces,” we proposed a fascia-to-space surgical approach to perform LLND. 3D laparoscopic TME plus LLND was performed successfully in all patients. The mean operating time was 172 minutes with a mean blood loss of 85 mL. Postoperative complications were present in 5 (17.4%) patients (CD I–II), including a case of urinary retention. The median number of harvested LLNs was 9, and positive LLNs were detected in 7 (30.4%) patients. After a median follow-up of 26.5 months, 2 (8.7%) patients developed liver metastases, but no local recurrence.
Conclusions:
Laparoscopic LLND based on membrane anatomy is a safe, feasible, and reproducible procedure and thus worthy of clinical promotion. Further studies with long-term follow-up in larger patient series are still required.
Introduction
Lateral lymph node (LLN) metastasis has been estimated to occur in 15%–30% of patients with lower rectal cancer and is a significant contributor to postoperative recurrence.1,2 Lateral lymph node dissection (LLND) is an effective operation for removing metastatic lymph nodes. 3 In Japan, total mesorectal excision (TME) plus LLND has become the standard surgical procedure for locally advanced lower rectal cancer. 4
However, the role of LLND still remains controversial in Western countries because of the complexity of this procedure and complications it induces.5,6 A Japanese clinical trial (JCOG0212) reported that even with the introduction of pelvic autonomic nerve preservation, the rate of urinary dysfunction following LLND could be as high as 59%. 7
In recent years, with the development of membrane anatomy in colorectal surgery, more and more surgeons have begun to investigate LLND based on membrane anatomy with the aim of improving precision and safety of the procedure.8,9 However, up to now, the detailed anatomy of fasciae and fascial spaces related to LLND has not been well described and therefore there is no established standard surgical procedure.
Based on years of experience in cadaveric dissections, we conducted an in-depth analysis of the membrane anatomy related to radical rectal cancer surgery10,11 and proposed the theory of “four fasciae and three spaces.” 12 Generally, the fascia propria of the rectum, urogenital fascia, vesicohypogastric fascia, and parietal fascia lie side by side in a medial–lateral direction and form three spaces (medial, middle, and lateral) around the rectum. Among them, the medial space corresponds to the resection area of TME and the middle and lateral spaces constitute the surgical field for LLND. 13
According to the theory, we developed a technique of laparoscopic LLND in two fascial spaces to simplify the surgical procedure (Fig. 1). In this study, we introduced the key elements of this procedure and reported its short-term outcomes.
Laparoscopic LLND in “two fascial spaces” based on membrane anatomy. LLND, lateral lymph node dissection.
Materials and Methods
Case–patient
This was a prospective cohort observational study that was conducted on patients who underwent 3D laparoscopic TME plus LLND at our hospital between July 2018 and December 2020.
The inclusion criteria were as follows: (1) patients aged between 18 and 75 years with no sex predominance; (2) pathologically confirmed rectal adenocarcinoma at clinical stage II/III; (3) the lower margin of the tumor located at or below the peritoneal reflection; (4) preoperative evaluation showing no urinary dysfunction; and (5) clinical suspicion of LLN metastasis based on magnetic resonance imaging evaluation. Specifically, LLNs >7 mm in the short-axis diameter before treatment were indicated for LLND, regardless of their response to neoadjuvant chemoradiation therapy (nCRT). 14
This study was approved by our local ethics committee (LL-2020-SCI-001) and performed in accordance with the Helsinki Declaration. 15 The trial was registered at the Chinese Clinical Trial Registry (ChiCTR2200061531), and written informed consent was obtained from all patients.
Key surgical procedure
The patient was placed in a modified lithotomy position under general anesthesia, and a five-trocar placement was utilized. LLND is performed following TME, with the choice of unilateral or bilateral LLND depending on the location of enlarged LLNs.
According to the theory of “four fasciae and three spaces,” the middle and lateral spaces formed by the urogenital fascia, vesicohypogastric fascia, and parietal fascia constitute the dissection plane for LLND.12,13 We proposed a fascia-to-space surgical approach to perform LLND (Fig. 1), and key surgical procedures were as follows:
Step 1: Separation of the urogenital fascia to expose the medial surface of the middle space. The urogenital fascia (i.e., visceral fascia) presents as a sandwich-like fascia sheath and extends posterolaterally to the rectum, containing the hypogastric nerves (HGNs), ureters, and genital vessels. Given the close anatomic relationship between the urogenital fascia and neural structures, separation of urogenital fascia actually covers the exposure of HGNs, pelvic plexus, and ureters.
Specifically, the separation of urogenital fascia extends anteriorly to the level of the vas deferens (male) or the round ligament of the uterus (female) and deeply into the exposure of the internal iliac vein (Fig. 2).
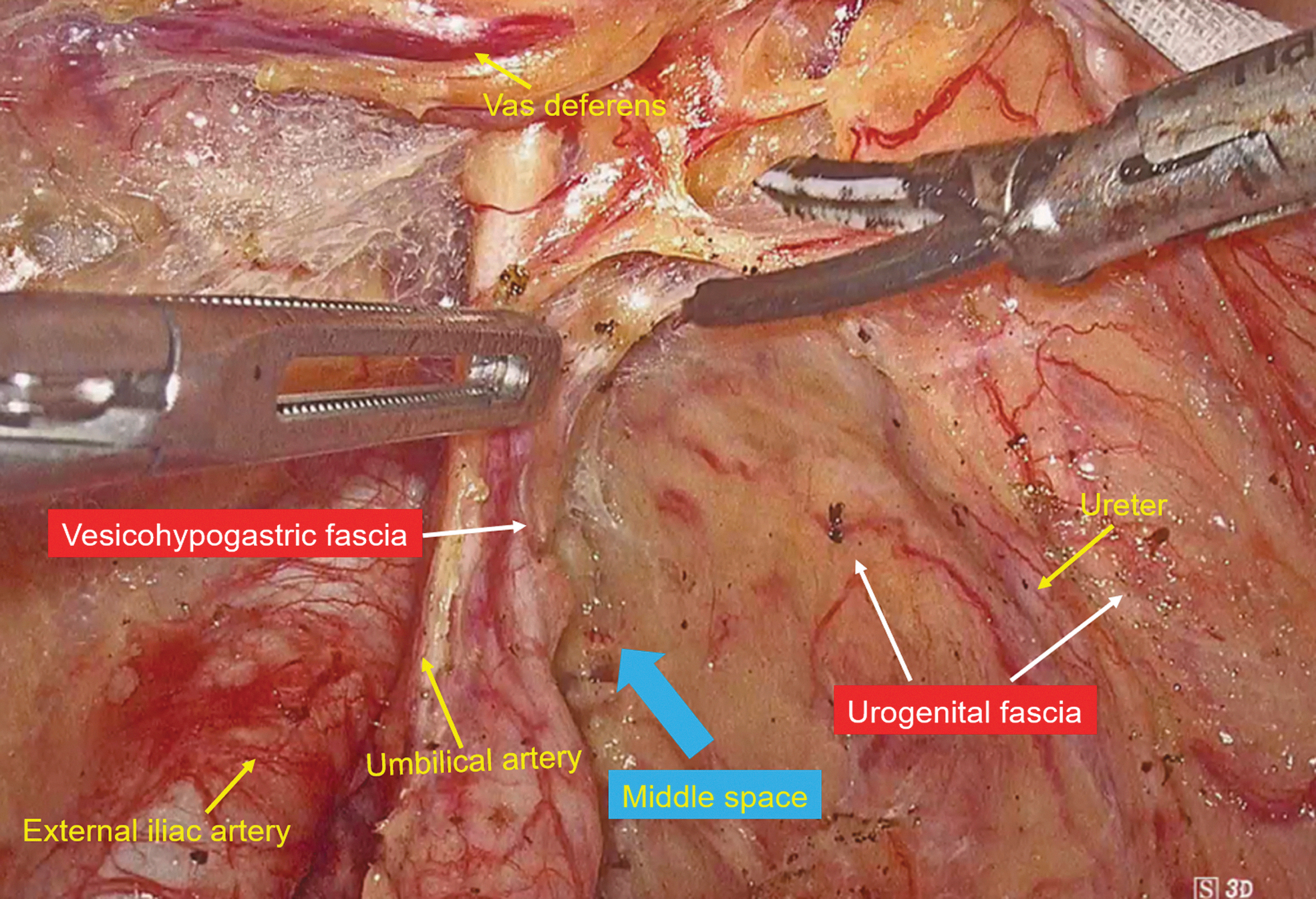
Separation of the urogenital fascia to expose the medial surface of the middle space.
Step 2: Separation of the obturator fascia to expose the lateral surface of the lateral space. The obturator fascia is the part of the parietal fascia covering the obturator muscle and its separation is performed along the external iliac vessels. This process allows removal of external iliac lymph nodes (#293), common iliac lymph nodes (#273), and abdominal aortic bifurcation lymph nodes (#280).
During the #293 dissection, special attention should be paid to protection of the genitofemoral nerve, which runs along the inner edge of the psoas major muscle and divides into genital and femoral branches before entering the internal inguinal ring (Fig. 3).

Separation of the obturator fascia to expose the lateral surface of the lateral space.
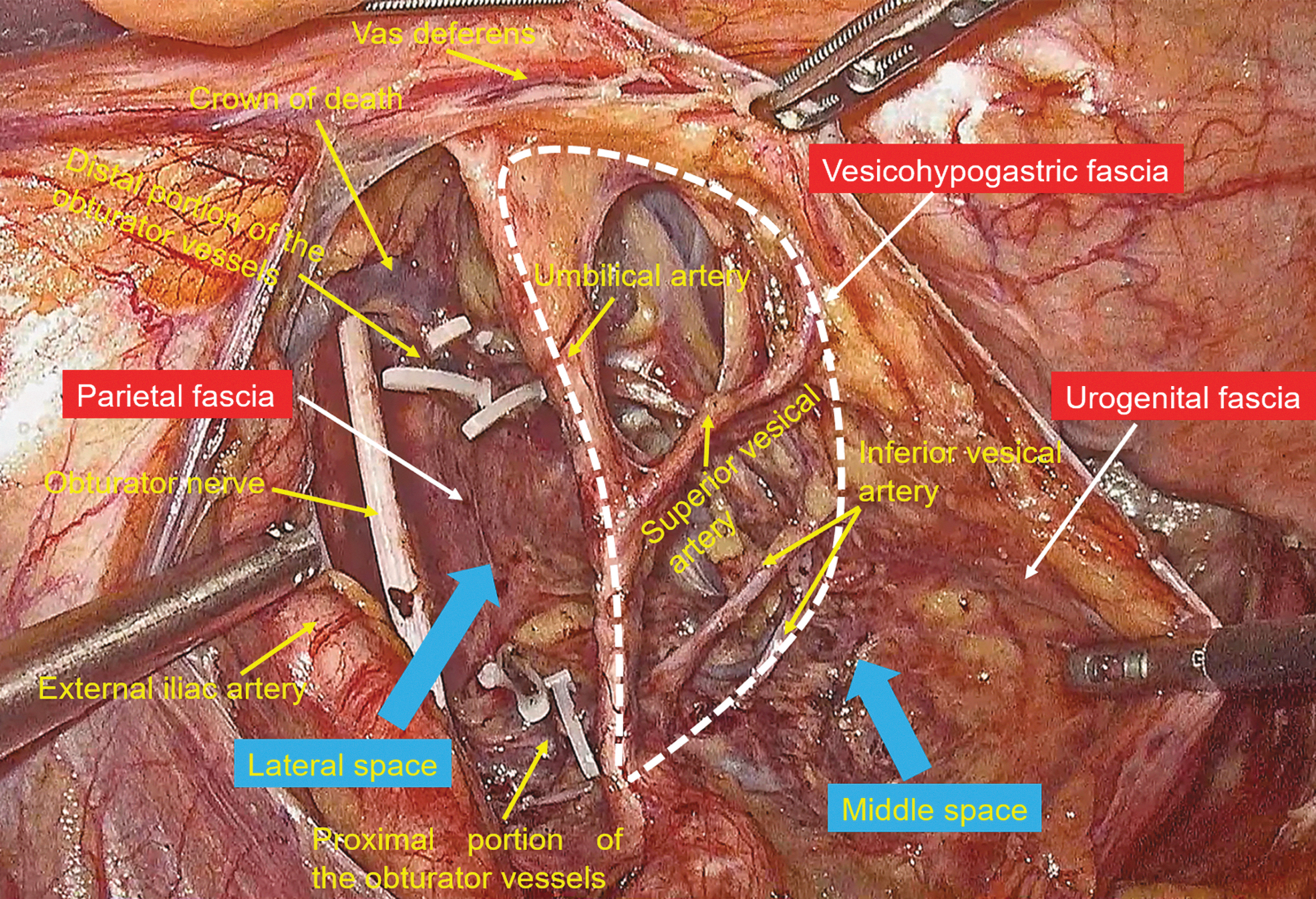
Step 3: Separation of the vesicohypogastric fascia to expose the medial surface of the lateral space. The vesicohypogastric fascia is a triangle-shaped fascia bounded by the umbilical artery, the tendinous arch of the pelvic fascia, and the bladder sidewall. The urogenital fascia and vesicohypogastric fasciae blend with each other in the tendinous arch of the pelvic fascia and present as a “V” shape.
The umbilical artery is the first branch of the internal iliac artery and is an important anatomical landmark for separation of the vesicohypogastric fascia. The separation is performed along the lateral side of the branches of the internal iliac vessels until the bladder sidewall is reached (Fig. 4).

Separation of the vesicohypogastric fascia to expose the medial surface of the lateral space.
Step 4: Lymph node dissection in the lateral space. According to the principle of membrane anatomy, space dissection is performed following the establishment of fascia planes. The lateral space lies between the vesicohypogastric fascia and parietal fascia and is where the obturator lymph nodes (#283) are located. In addition to #283, removal of lateral sacral lymph nodes (#260) can also be done in this space.
Due to establishment of the vesicohypogastric fascia plane, the lateral space mostly contains not only the neural structures but also the obturator artery and vein. Therefore, space dissection mainly includes three steps: proximal and distal ligation of obturator vessels, release of the obturator nerve, and exposure of the sacral plexus.
Step 5: Lymph node dissection in the middle space. The middle space is located between the urogenital fascia and vesicohypogastric fascia. The anterior trunks of internal iliac vessels and most of their branches run in this space, including the uterine artery, middle rectal artery, and superficial and deep uterine veins. Therefore, the middle space dissection is actually dissection of internal iliac vessels. To completely remove the internal iliac lymph nodes (#263) and median sacral lymph nodes (#270) in this space, the vesicohypogastric fascia is dissected during this process.
Data collection and follow-up
Clinical data were prospectively documented from patients' medical records, including demographic characteristics (age, sex, and body–mass index [BMI]), pathological features (tumor stage, number of LLNs, and resection margin), and perioperative variables (operating time, blood loss, length of hospital stay, and postoperative complications).
Tumor was staged according to the eighth edition of the American Joint Committee on Cancer (AJCC) Manual for Staging of Cancer. Complications were defined as any deviation from the normal postoperative course occurring within 30 days of surgery and graded according to the Clavien-Dindo (CD) classification. 16
All patients underwent regular follow-up evaluation for at least 18 months after surgery to assess for tumor recurrence, including physical examination, serum tumor markers, chest X-ray, abdominopelvic computed tomography scan, and colonoscopy. In addition, urinary function was evaluated by measurement of residual urine volume preoperatively and 7–14 days postoperatively. The residual urine volume was generally measured by catheterization or ultrasound, and values >50 mL were considered as urinary dysfunction. 17
Results
Patient characteristics and perioperative outcomes
A total of 23 (17 males and 6 females) patients with lower rectal cancer were included in this study, with a mean age of 59 ± 6.8 years. The BMI was 25.2 ± 1.4 and 21.4 ± 0.6 in males and females, respectively. Of these, 9 patients received neoadjuvant chemoradiation therapy before surgery and 6 of them (66.7%) had a reduction in LLN size after treatment. The 3D laparoscopic TME plus LLND was successfully performed in all patients without conversion to laparotomy, including 21 cases of unilateral and 2 cases of bilateral LLND.
The mean operating time and blood loss for LLND were 172 ± 47 minutes and 85 ± 22 mL, respectively. The mean postoperative hospital stay was 10 ± 3.6 days, and there were no perioperative deaths.
Postoperative complications
The overall postoperative complication rate was 17.4% (5/23), including a case of small bowel obstruction (CD grade II), a case of lymph leakage (CD grade II), a case of urinary dysfunction (CD grade II), and a case of lower limb pain (CD grade I). These patients recovered after conservative treatment without surgical intervention.
It was noted that all patients had no obvious urinary dysfunction preoperatively, with a median residual urine volume of <50 mL, and the urinary catheter was generally removed on the fourth postoperative day after bladder exercise. However, 1 (4.3%) patient suffered from urinary retention with postvoid residual urine volume of 220 mL and intermittent catheterization was performed for one more week.
Oncologic outcomes
Postoperative pathology showed that 8 cases were at stage II and 15 cases were at stage III. The resection margins were all negative, and a minimum distance of 1 cm distally was maintained. The median number of harvested mesenteric lymph nodes and LLNs was 13 (range 11–18) and 9 (range 6–12), respectively. LLN metastases were present in 7 (30.4%) patients, and all positive LLNs were internal iliac lymph nodes (#263) and/or obturator lymph nodes (#283). Among them, 6 patients had both mesenteric lymph nodes and LLN metastases, and 1 had only LLN metastases.
During the median follow-up period of 26.5 months (range 18–36 months), 2 (8.7%) patients developed liver metastases and received further treatment, but no anastomotic recurrence or regional lymph node metastasis was observed.
Discussion
The Japanese Guidelines for the Treatment of Colorectal Cancer in 2019 stated that for patients with T3–T4 lower rectal cancer, LLND can enhance local control and reduce distant spread, leading to an improved 5-year overall survival rate. 18 However, because of the complicated procedure and high complication rate, LLND has so far not been widely used in clinical practice.6,19 Therefore, establishment of a simple, safe, and reproducible surgical procedure is key to popularizing its application.
According to the Japanese Classification of Colorectal Cancer (Version 9), the extent of LLNs was sorted as iliac artery series and numbered as #263, #273, #283, #293, #260, #270, and #280. 20 Clinical studies have demonstrated that LLN metastases are mainly confined to the internal iliac lymph nodes (#263) and obturator lymph nodes (#283), and the incidence of metastasis in other sites was only 7.7%, 19 which was also confirmed in our study.
On the basis of the theory of “four fasciae and three spaces,” we proposed a fascia-to-space surgical approach to perform LLND. 12 Specifically, we first dissect the urogenital fascia, vesicohypogastric fascia, and parietal fascia to build the fascial planes and develop fascial spaces, and this process allows the removal of #293, #273, and #280. Then, we perform space dissection to remove #263 and #270 in the middle space and #283 and #260 in the lateral space. 13
Thereby, our proposed surgical procedure can successfully finish the LD2 or LD3 dissection according to the LLN status recommended by the Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines. 21 Our preliminary experience showed that it significantly improved surgical safety while ensuring oncologic outcomes, with the advantages of easy identification of the surgical plane and clear location of nerves and vessels.
The middle space corresponds to the Latzko's pararectal space 22 in the traditional anatomy. The contents of this space are mainly blood vessels, and the branches of the internal iliac artery have certain distinguishing characteristics (Fig. 5). The umbilical artery is the first branch of the internal iliac artery and often shares a common trunk with the superior vesical artery, with a constant anatomical location. The vessels crossing above and below the ureter are the uterine artery and deep uterine vein, respectively. The vesical veins mainly course laterally along the bladder, uterus, or vagina in a sagittal plane.

The internal iliac vessels and most of their branches run in the middle space.
Both the inferior gluteal artery and internal pudendal artery enter the lesser sciatic foramen eventually, and the latter is also called the terminal branch of the internal iliac artery. The inferior vesical artery is the site where the internal iliac lymph nodes are prone to metastasis. It is the last branch of the internal iliac artery and located above the infra-piriformis foramen and is therefore deemed as the distal end of vessel dissection.
In addition, it is very important to accurately locate the internal iliac vein in LLND as its bleeding can be tricky. After extensive cadaveric dissection and surgical observation, we determined that the internal iliac vein was located between the inferior gluteal artery and the internal pudendal artery (Fig. 6), which can act as a useful anatomical landmark in surgery. 13
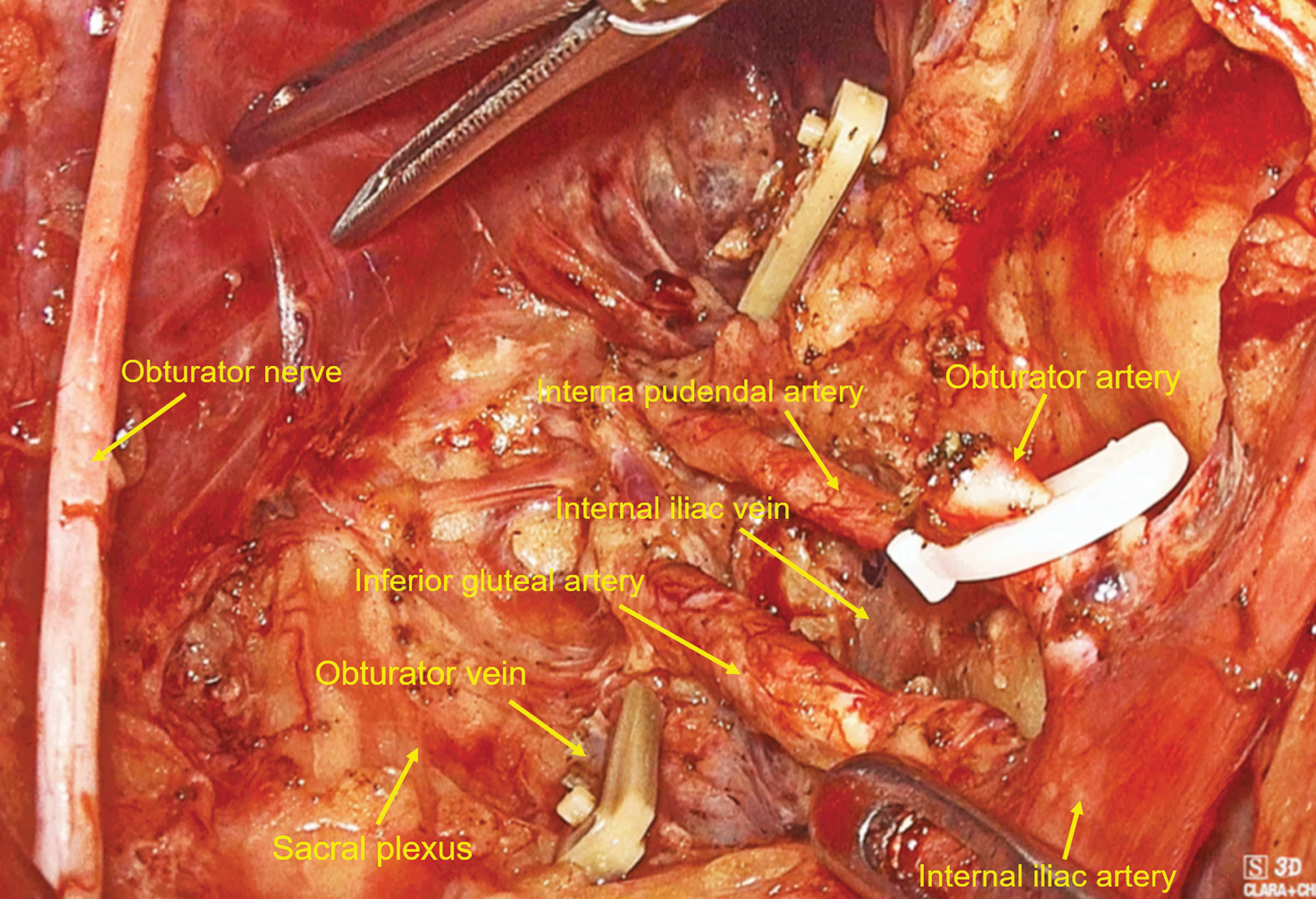
The internal iliac vein lies between the inferior gluteal artery and the internal pudendal artery.
The lateral space corresponds to the paravesical space 23 in the traditional anatomy and mainly contains neural structures (including the lumbosacral trunk, sciatic plexus, obturator nerve, and sciatic nerve) in addition to the obturator vessels. The lateral space dissection can begin with cleaning of superior inguinal lymph nodes, which although not included in LLND, is conducive to exposure of the obturator nerve and vessels.
When ligating the distal end of the obturator vessel, special attention should be paid to the lateral corona mortis (also known as crown of death) and medial vesical veins to avoid accidental bleeding. The sacral plexus is located ventrally to the piriformis muscle and covered with the parietal fascia (i.e., piriformis fascia).
The sacral plexus constitutes the dorsal boundary of obturator lymph node dissection in the lateral space. In addition, the dorsal penile nerve emanates from the pudendal nerve, the branches of the sacral plexus. As a result, it is another key structure that needs to be identified and adequately protected in LLND.
Our anatomical study showed that the sacral plexus was usually located below the origin of the obturator artery from the internal iliac artery (Fig. 6).
Conclusions
In conclusion, our short-term outcomes showed that laparoscopic LLND based on membrane anatomy is a safe and effective procedure for treatment of locally advanced lower rectal cancer. This technique is feasible and reproducible and thus worthy of clinical promotion.
However, further studies with larger sample sizes and longitudinal follow-up are still needed to strengthen the promising evidence.
Patient Consent
All study participants, or their legal guardians, provided informed written consent before study enrollment.
Ethical Approval
This study was reviewed and approved by the Yangpu Hospital Institutional Review Board (LL-2020-SCI-001).
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the National Natural Science Foundation of China under grant 81874201; Shanghai Pujiang Program under grant 21PJD066; Science and Technology Commission of Shanghai Municipality under grant 20Y11908300; and Shanghai Municipal Health Commission under grant 202040122.