
Abstract
Background:
Laparoscopic hepatectomy (LH) is considered a safe and feasible treatment for patients with hepatocellular carcinoma (HCC) in recent studies. However, in elderly patients, application of LH still remains controversial, and the outcomes of LH versus open hepatectomy (OH) have not been fully evaluated. Our objective is to compare the short- and long-term outcomes of LH with OH in elderly patients with HCC.
Materials and Methods:
All studies comparing LH and OH in elderly patients with HCC were systematically searched in the databases of PubMed, EmBase, and Web of Science. Statistical analysis was conducted using Review Manager 5.3 (Cochrane Collaboration, 2014). The last search was performed on March 20, 2022. Short-term outcomes include blood loss, operation time, blood transfusion, overall and major postoperative complications, mortality, hospital stay, tumor size, and surgical margin. Long-term outcomes include 1-, 3-, and 5-year overall survival (OS); 1-, 3-, and 5-year disease-free survival (DFS); and 1-, 3-, and 5-year recurrence-free survival (RFS).
Results:
Fourteen studies involving 1596 patients were included in this meta-analysis. The short-term outcomes of LH were a shorter postoperative hospital stay and fewer overall and major postoperative complications (all P < .00001). However, there were no significant differences in operation time, blood loss, blood transfusion rate, surgical margin, tumor size, and mortality. For the long-term outcomes, LH is comparable with OH in terms of 1-, 3-, and 5-year OS; 1-, 3-, and 5-year DFS; and 1-, 3-, and 5-year RFS.
Conclusions:
Compared with OH, LH is a safe and feasible treatment for elderly patients with HCC.
Introduction
With the increase in life span of the elderly population, the incidence of diseases is increasing; 92 diseases were identified as age related. 1 From 2006 to 2016, cancer cases increased by 28% worldwide, and an aging population contributed 17% to this change. 2 Hepatocellular carcinoma (HCC) is the sixth most common cancer and the second leading cause of cancer-related deaths. 3
Population aging was one of the factors that increased the cases of liver cancer from 732,000 in 2006 to 1 million in 2016. 2 Although a declining incidence of HCC was observed in some countries in recent years, for elderly patients, the incidence is still increasing. 4 Therefore, there is an urgent need for optimal management of elderly patients with HCC.
The treatment of HCC includes surgical resection, transplantation, ablation, transarterial chemoembolization, and tyrosine kinase inhibitors. 5 For resectable cases, surgical resection is still a first-line curative treatment for HCC. 6 For elderly patients, however, management of HCC is complex as no prospective studies and guidelines are currently available.
Controversies still remain regarding surgical liver resection for the elderly. First, elderly patients have more comorbidities, such as cardiovascular problems, diabetes mellitus, hypertension, and pulmonary diseases, which increase the risk of complications perioperatively. 7 Second, the function and structure of the liver change and the regenerative ability of liver cells declines in the elderly. 8 Third, life expectancy of the elderly is limited.
Considering these aspects, surgeons tend to adopt conservative treatments for elderly patients. In the past two decades, liver resection was applied in 12%–28% of young patients, while the range was 0%–14% in elderly patients 9 ; this rate was underestimated for management of elderly patients with HCC. Nonetheless, from studies reported in recent years, elderly patients can also benefit from liver resection.10,11
Since first described by Reich in 1991, 12 great progress has been made with laparoscopic hepatectomy (LH) in liver surgery in recent years. Compared with open hepatectomy (OH), LH shows encouraging outcomes perioperatively. However, potential disadvantages of laparoscopy have reduced the popularity of LH in elderly patients, such as the adverse effects of increased intra-abdominal pressure, incidence of postoperative complications, and uncertain prognosis of LH.9,13 In view of these concerns, conservative opinions still remain regarding application of LH in elderly patients.
Although outcomes have been reported in some article reviews about LH in elderly patients,14–17 the number of studies included were limited. Furthermore, besides HCC, tumors of other pathological types were also included in the literature, such as intrahepatic cholangiocarcinoma and metastatic tumor, which may result in different surgical outcomes; maybe for this reason, long-term outcomes were not evaluated in these studies. Therefore, the objective of our study is to evaluate the short- and long-term outcomes in elderly patients with HCC.
Materials and Methods
Ethical Statment
The research was completed in accordance with the Declaration of Helsinki revised in 2013.
Data sources and search strategy
This systematic review and meta-analysis was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). 18 Searches were conducted in the databases of PubMed, EmBase, and Web of Science.
Combinations of the following key words were used for searching: “laparoscopic hepatectomy,” “laparoscopic liver resection,” “minimal invasive hepatectomy,” “minimal invasive liver resection,” “open hepatectomy,” “open liver resection,” “hepatocellular carcinoma,” “liver cancer,” “elderly patients,” and “aged patients.”
Reference lists of the selected studies and relevant systematic reviews were also checked to identify studies that met our inclusion criteria. The last search was performed on March 20, 2022.
Study selection
Two authors (S.J. and D.Y.) screened the identified studies independently. The final decision of included studies was made by consensus of the two authors. Inclusion criteria for this meta-analysis were as follows: (1) studies related to the comparison between LH and OH in elderly patients with HCC; (2) studies with age cutoff for elderly patients set at ≥65 years or most patients aged ≥65 years; (3) studies reporting at least one of the outcomes of interest; and (4) studies with language restricted to English.
The exclusion criteria were as follows: (1) studies with no control group; (2) nonhuman studies, reviews, letters, abstracts, editorials, or case reports; (3) studies comparing elderly and nonelderly patients; (4) studies including patients with benign lesions or other types of malignant liver tumors; and (5) studies on repeat liver resection for recurrent cases.
Data extraction
Data extraction was conducted by two authors (S.J. and D.Y.) independently, and any discrepancies were resolved through discussion. The data of baseline characteristics extracted include the first author, region, study design, period, age, number of patients, and conversion.
Outcomes of interest include blood loss; operation time; overall and major postoperative complications; transfusion rate; mortality; hospital stay; tumor size; surgical margin; 1-, 3-, and 5-year overall survival (OS); 1-, 3-, and 5-year disease-free survival (DFS); and 1-, 3-, and 5-year recurrence-free survival (RFS). Major complication was defined as Clavien–Dindo grade ≥III or extracted from studies when it was reported directly.
Quality assessment
Quality assessment of the included studies was based on the Newcastle–Ottawa Scale (NOS), which consists of three sections: patient selection, comparability of the study, and assessment of the outcome. The total score ranged from 0 to 9. Studies with cumulative scores ≥7 were denoted as high-quality studies.
Statistical analyses
All statistical analyses were conducted using Review Manager 5.3 (Cochrane Collaboration, 2014). Continuous outcomes are expressed as medians and ranges or medians and interquartile ranges were converted to means and standard variances based on the method by Hozo et al. 19 Odds risk (OR) and weighted mean difference (WMD) were used for dichotomous and continuous variables, respectively; 95% confidence intervals (CIs) are reported for all results.
Heterogeneity was assessed using the value of the chi-square test and I2 .test. P < .10 and I2 > 50% represent the existence of significant heterogeneity among studies, and a random-effects model was applied for the data analysis. Otherwise, a fixed-effect model was used. Statistical significance for comparison was set at P < .05. The subgroup analysis was performed according to matched and nonmatched studies.
A sensitivity analysis was conducted to explore potential sources of heterogeneity by excluding one study in each turn to evaluate the effect on the overall pooled results. A funnel plot was used to assess publication bias.
Results
Study selection and characteristics
The study search strategies and results are shown in Figure 1. A total of 3249 studies were found in the primary literature search. After removing 2174 duplicates, 1075 articles were assessed by screening the titles and abstracts. Then, 1040 articles were excluded due to irrelevance. For the remaining 35 studies, 21 full-text studies were further removed according to our exclusion criteria.
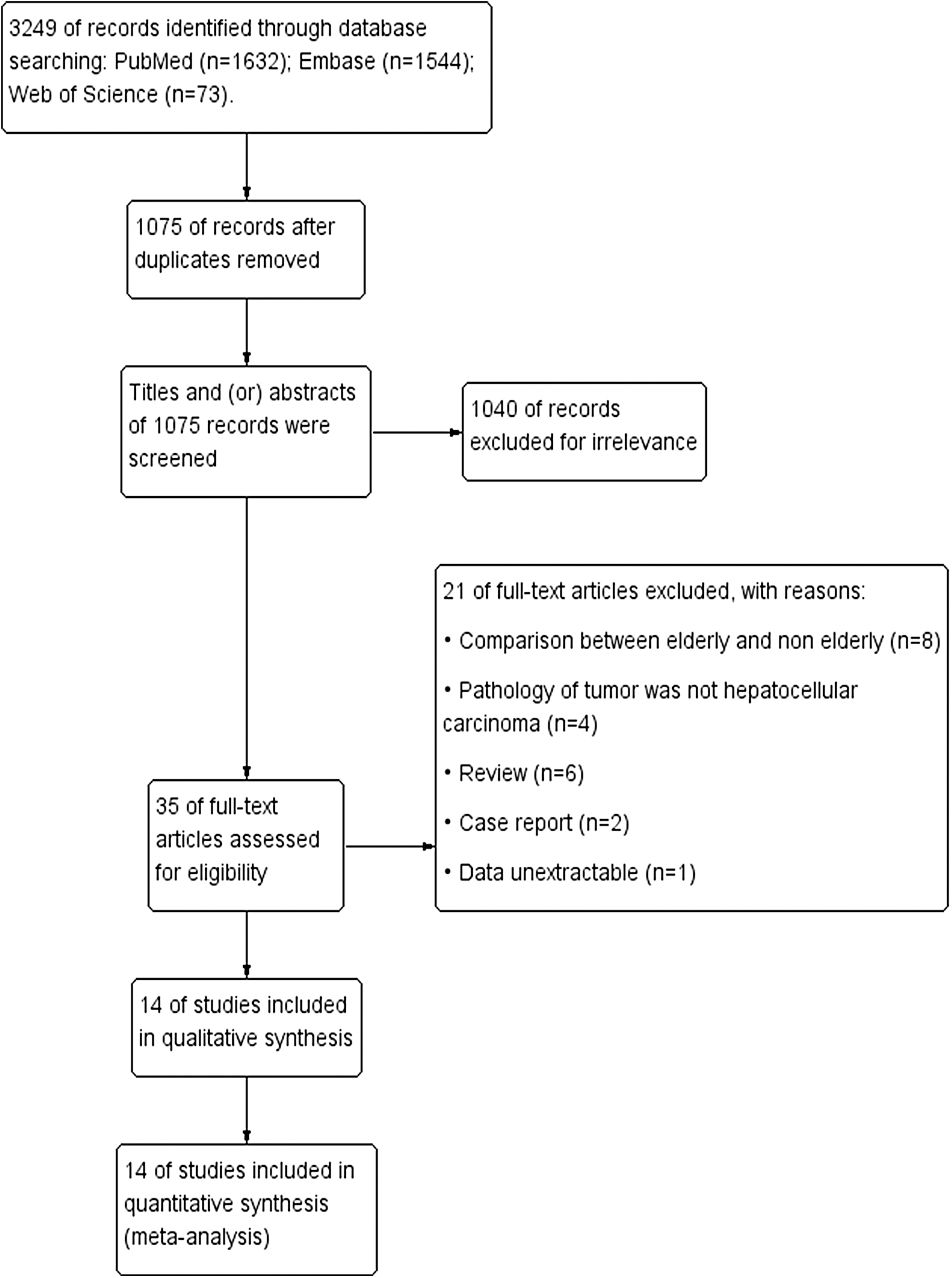
Flowchart of study inclusion.
Finally, 14 studies20–33 published between 2001 and 2022 met our inclusion criteria. Twelve studies were matched and two were nonmatched. In these studies, the age cutoff for elderly patients was set at ≥75 years (n = 2),20,27 ≥70 years (n = 5),21–24,29 and ≥65 years (n = 2).26,33 Five studies did not target elderly patients; however, the minimum age of patients was over 65 years in one study, 31 and in the other four studies,25,28,30,32 the mean age was >65 years, with small ranges or standard deviations, so most of the patients evaluated were over 65 years of age.
There were 1569 patients in total, 744 patients were in the laparoscopic group and 825 patients in the open group. The rate of conversion ranged from 0% to 28.1%. The baseline characteristics of included studies are presented in Table 1.
Baseline Characteristics of Included Studies
Median(range).
Mean ± SD.
Median (IQR).
Mean (95% CI).
CI, confidence interval; IQR, interquartile range; MR, matched retrospective; NA, not available; NOS, Newcastle–Ottawa Scale; R, retrospective.
Short-term outcomes
The operation time was reported in 13 studies.20–26,28–33 Pooled data suggested that there was no significant difference between the two groups (1259 patients, WMD = 8.86, 95% CI = −11.12 to 28.83, P = .38, Fig. 2a), and similar results can be observed in both matched and nonmatched studies. In addition, there remained a significant degree of heterogeneity (I 2 = 88%, P < .00001).
Forest plots and subgroup meta-analysis of the operation time
Thirteen studies20–22,24–33 reported blood loss, which revealed that there was no statistically significant difference in blood loss between LH and OH groups (1447 patients, WMD = −34.22, 95% CI = −146.61 to 78.18, P = .55, Fig. 2b), although nonmatched studies suggested less blood loss in the LH group; only two studies were included. Heterogeneity among the studies was high (I 2 = 95%, P < .00001).
The surgical margin was evaluated in six studies.21,24,26,30,31,33 The pooled data were all from matched studies, and there was no significant difference between the two groups (706 patients, WMD = −0.18, 95% CI = −0.60 to 0.25, P = .41, Fig. 2c). Heterogeneity was also high among studies (I 2 = 95%, P < .00001).
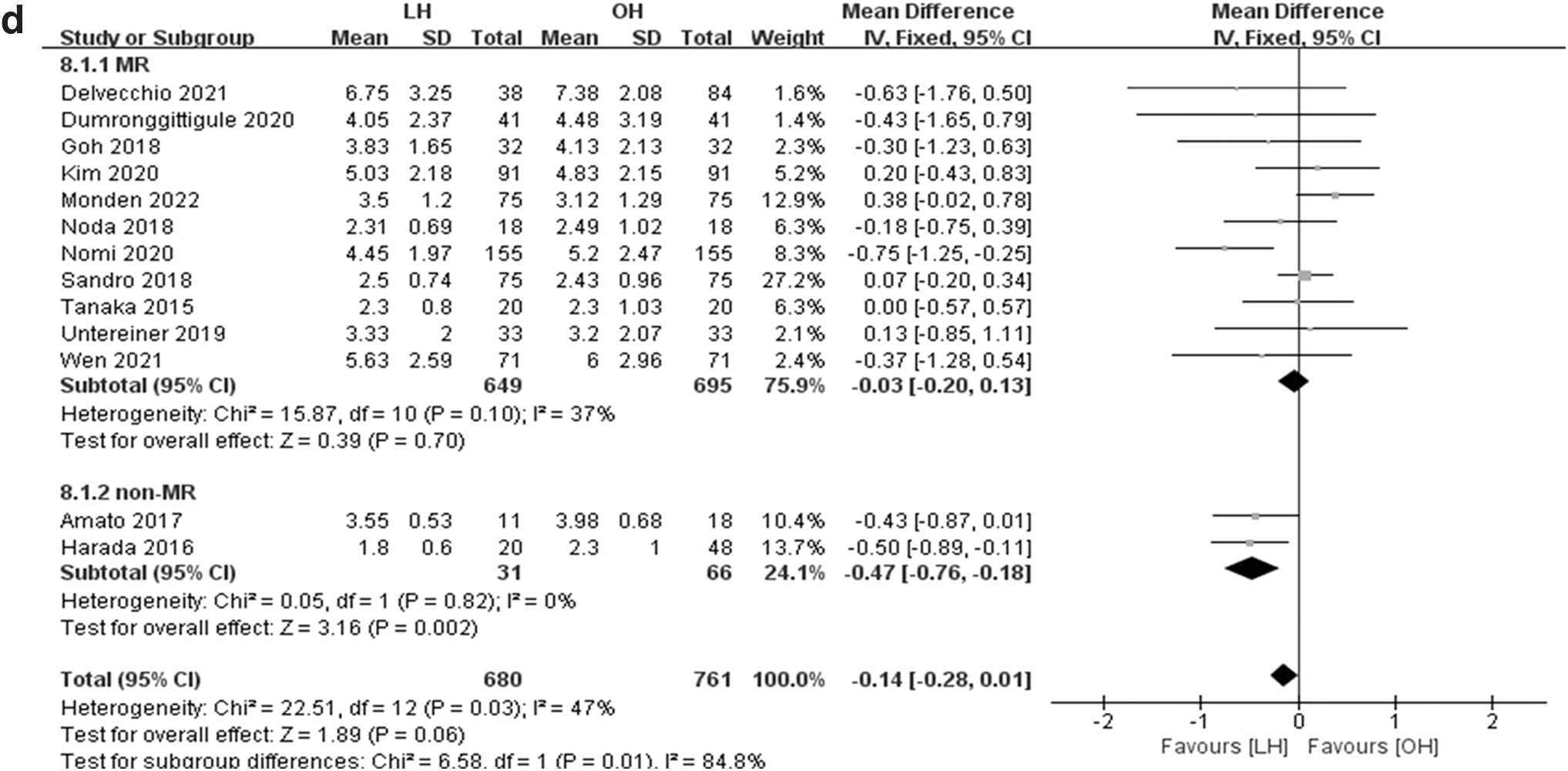
The tumor size was reported in 13 studies.20,22–33 Pooled data suggested that there was no significant difference in tumor size between the two groups (1441 patients, WMD = −0.14, 95% CI = −0.28 to 0.01, P = .06, Fig. 2d), and there was low heterogeneity among the studies (I 2 = 47%, P = .03), although the nonmatched group revealed a smaller tumor size in the LH group; only two studies were included.
There were 10 studies that reported on blood transfusion.22–27,29,30,32,33 No significant difference was observed in blood transfusion between the two groups (1336 patients, OR = 0.67, 95% CI = 0.40–1.12, P = .12, Fig. 3a).
Forest plots and subgroup meta-analysis of blood transfusion
Twelve studies reported overall postoperative complications.20–25,27,28,30–33 The result showed that there were fewer overall postoperative complications in the LH group (1237 patients, OR = 0.38, 95% CI = 0.29–0.49, P < .00001, Fig. 3b), and the subgroup analysis also presented a similar result.
Twelve studies reported major postoperative complications.20–25,27,29–33 The result showed that there were fewer major postoperative complications in the LH group (1351 patients, OR = 0.40, 95% CI = 0.28–0.58, P < .00001, Fig. 3c), although a different result was observed in nonmatched studies; there were only two studies in this group.
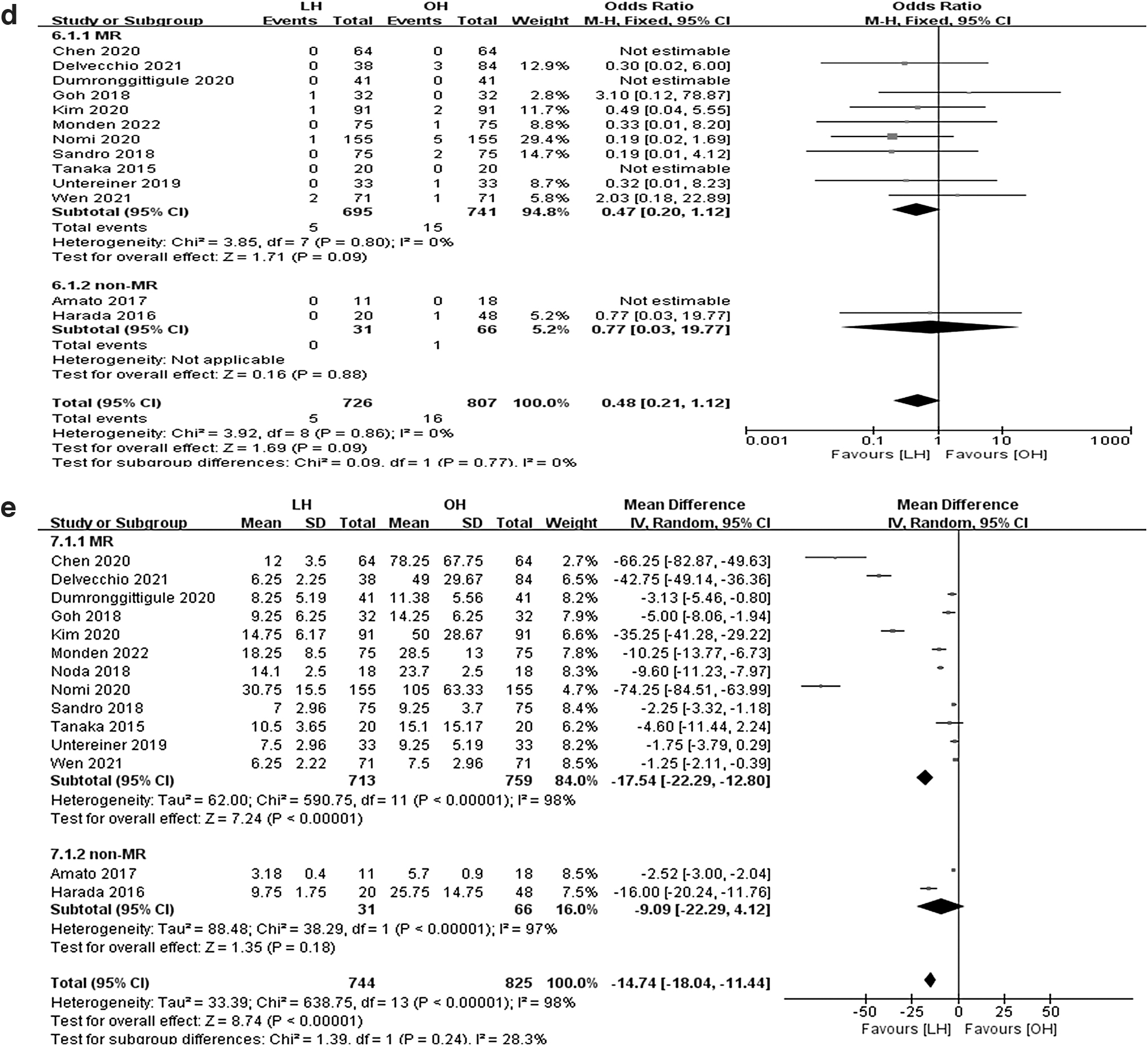
Mortality was reported in 13 studies.20–27,29–33 The outcome suggested that there was no significant difference between the two groups in mortality (1533 patients, OR = 0.48, 95% CI = 0.21–1.12, P = .09, Fig. 3d).
The duration of hospital stay was reported in 14 studies.20–33 Patients in the laparoscopic group had a shorter postoperative hospital stay (1569 patients, WMD = −14.74, 95% CI = −18.04 to −11.44, P < .00001, Fig. 3e), although a significant statistical difference was not observed in nonmatched studies. In addition, there also remains a significant degree of heterogeneity among the studies (I 2 = 98%, P < .00001).
Long-term outcomes
For long-term outcomes, pooled data revealed that there were no statistical differences in 1-year OS22,23,26,28,31 (462 patients, OR = 1.02, 95% CI = 0.37 to 2.81, P = .97, Fig. 4a), 3-year OS22,23,26,28,30–32 (678 patients, OR = 1.41, 95% CI = 0.89 to 2.24, P = .14, Fig. 4b), 5-year OS21–23,26,28,31 (590 patients, OR = 1.19, 95% CI = 0.80–1.78, P = .38, Fig. 4c), 1-year DFS23,26,28,31 (380 patients, OR = 0.69, 95% CI = 0.42–1.13, P = .14, Fig. 4d), 3-year DFS23,26,28,31 (380 patients, OR = 0.92, 95% CI = 0.59–1.41, P = .69, Fig. 4e), 5-year DFS21,23,26,28 (468 patients, OR = 0.70, 95% CI = 0.48–1.02, P = .07, Fig. 4f), 1-year RFS22,25 (150 patients, OR = 1.15, 95% CI = 0.53–2.49, P = .72, Fig. 4g), 3-year RFS22,25,30,32 (366 patients, OR = 1.06, 95% CI = 0.69–1.61, P = .80, Fig. 4h), and 5-year RFS22,25 (150 patients, OR = 1.01, 95% CI = 0.34–3.02, P = .98, Fig. 4i) between the LH and OH groups.

Forest plots of 1-year OS
Sensitivity analysis, publication bias, and subgroup analysis
A sensitivity analysis was conducted by excluding one study in each turn to evaluate the effect on the overall pooled results; however, the heterogeneity was not substantially reduced.
Publication bias was evaluated based on funnel plots of perioperative outcomes (Fig. 5). There was no evidence of bias for operation time, blood loss, tumor size, overall complications, major complications, and mortality. However, the funnel plot for hospital stay showed some degree of bias, which may be due to different discharge criteria between centers.

The funnel plot of operation time
The subgroup analysis was based on matched and nonmatched studies. We found that the pooled outcomes of matched studies were in line with that of total pooled outcomes. However, in the nonmatched group, less blood loss, smaller tumor size, and no statistical differences in severe complications and hospital stay were reported for LH. Considering the limited studies included in the nonmatched group, these outcomes should be interpreted with caution.
Discussion
Aging is associated with increased oxidative stress, heightened inflammatory response, and deteriorating immunity. 34 The structure and function of the liver change gradually with aging, such as decrease in liver mass and hepatic blood flow and dysfunction in synthesis and metabolism of liver cells. 35 The generation capacity of liver cells weakens and recovery of liver function is delayed when exposed to injuries.8,36
Meanwhile, comorbidities increase in this process. In addition, considering the limited life expectancy, liver resection in elderly patients remains controversial. Therefore, we conducted this review and meta-analysis to evaluate the safety and feasibility of LH for HCC in elderly patients.
With development of laparoscopic equipment and accumulation of surgeons' experience, LH has achieved great progress and shown encouraging results perioperatively, such as the tendency toward decrease in blood loss, conversion rate, and complications.37,38 A longer operation time was reported for LH in the beginning. 39
However, a comparable operation time between LH and OH has been presented in recent years.14–16 Tsai et al reported a shorter operation time for LH in their study. However, it was only observed in cases with early TNM stage of HCC. 40 In our study, a significant difference in operation time was not found between the two groups.
Actually, the outcome of operation time was not consistent among studies comparing LH with OH. This may be due to differences in the range of resection, location of tumor, learning curve, center volumes, and surgeons' experience, especially the range of liver resection. A shorter operation time for LH was observed in partial resection of the liver, whereas in the case of major liver resection, LH is not superior to OH in operation time.41,42
Hemorrhage is one of the main reasons for conversion in LH. 43 Considering the abundant blood supply in the liver, efficacious control of bleeding is key to the success of LH. Studies found that blood loss and transfusion were associated with increased postoperative complications and had a negative impact on long-term prognosis of patients undergoing hepatectomy.44–46
LH is considered with the advantages of bleeding control in some aspects, such as the hemostatic effect of high intraperitoneal pressure caused by carbon dioxide, high clarity, and magnified effect of laparoscopy, which allowed surgeons to better identify intrahepatic blood vessels.39,47,48 The development of laparoscopic devices in stanching bleeding may also play an important role in controlling bleeding. Less blood loss and a lower transfusion rate were reported in studies in recent years.14,16,17,49
However, in our study, blood loss and transfusion rates showed no significant difference between the two groups. It is worth noting that blood loss in LH may be underestimated. Studies indicated that traditional means of calculating blood loss by summing up the intraoperation suction fluid and gauze weight values may be inaccurate, as fluids cannot be suctioned fully because of the limited workspace in LH. On calculating the blood volume and change in hematocrit levels, there was no evidence in favor of LH for less blood loss than OH.50,51
To avoid touching the tumor, achieving a safe surgical margin in the condition of laparoscopic surgery was once a matter of concern. In line with previous studies, laparoscopic techniques have achieved surgical margins that are comparable with those of open liver resection.48,52 Enough surgical margin can be obtained by laparoscopic ultrasonic and imaging assessment perioperatively, such as indocyanine green fluorescence imaging. 53
A study revealed that patients with smaller tumor size were more likely to be submitted to LH 54 ; in our literature, however, a significant difference was not found in tumor size, and with low heterogeneity among studies, this may be because most of the studies included in our study were matched.
A published study showed that mortality and morbidity rates were 0%–42.9% and 9%–51%, respectively, in elderly patients with HCC after hepatectomy. 55 Although complications were considered more common in elderly patients, especially severe complications after traditional liver resection, 7 studies and meta-analyses have shown a comparable and even declining incidence of complications in recent years, especially with the laparoscopic approach.14–16,56
Similarly, our study showed that LH achieved not only fewer overall complications but also fewer major complications, with no statistical difference in mortality. This may be attributed to advances in perioperative management and advantages of laparoscopic surgery, such as a smaller incision and reduced inflammatory and stress responses. 57
Just as many previous studies have reported, the hospital stay was shorter in the LH group in our study. This was apart from less invasiveness, reduced pain, early recovery of gastrointestinal function, and fewer postoperative complications with LH.52,58,59
The prognosis of LH is still uncertain. Studies have found comparable long-term prognosis with OH and LH in patients with HCC.54,60,61 In addition, some studies indicate that LH may potentially provide better prognosis.62,63 Compared with the traditional open approach, laparoscopic surgery has the advantages of decreasing circulating tumor cells, perioperative stress, and manipulation of the tumor, which have positive effects of reducing the risk of tumor growth, recurrence, and metastasis.64–66
Age is one of the risk factors for the prognosis of HCC. 9 Considering the incidence of postoperative complications and long-term prognosis, surgical liver resection in elderly patients was applied with caution. Comparisons between LH and OH in elderly patients have been reported in previous studies; however, the long-term outcomes of the two groups were not evaluated.14–17
From studies reported in recent years, the prognosis of liver resection in elderly patients is found to be acceptable.67,68 In our study, the pooled results indicated that there were no significant statistical differences in OS, DFS, and RFS between the two groups. Studies suggested that the prognosis of LH in elderly patients and younger patients also showed no significant difference.69,70 Unfortunately, these studies are retrospective.
Furthermore, the prognosis can be influenced by pathological stage, vessel invasion, cirrhosis, tumor number, blood flow occlusion, and postoperative complications.71,72 Thus, the outcomes of prognosis still need randomized controlled trials for further confirmation.
There are some limitations that should be acknowledged in our study. First, owing to the different levels of socioeconomic and medical development, the definition of elderly varied worldwide, ranging from 60 to 80 years of age. 9 The cutoff used to define the age of elderly patients was different in the studies that we included, which may introduce bias and heterogeneity among studies.
Second, all of the studies included in our meta-analysis were retrospective; although most studies were matched, a randomized controlled trial was absent, and this may have led to some degree of selection bias.
Third, significant heterogeneity existed in the operation time, blood loss, hospital stay, and surgical margin; although we conducted sensitivity and subgroup analyses, significant reduction in heterogeneity was not observed. This may be due to the differences in hospital volumes, laparoscopy devices, definitions of outcomes, and different stages of learning curves for surgeons.
In conclusion, this study provides the evidence that compared with OH, elderly patients with HCC can benefit from LH with fewer postoperative complications and shorter hospital stay. Furthermore, the prognosis was comparable between the two methods. LH is safe and feasible for liver resection in elderly patients with HCC. Considering that the studies included are retrospective, randomized controlled trials are needed to confirm the results of our study.
Footnotes
Acknowledgment
The authors thank all the members in their department for their suggestions.
Authors' Contributions
S.J. was involved in conceptualization, data curation, formal analysis, investigation, and writing.
D.Y. was involved in data curation, formal analysis, and investigation.
H.H. was involved in methodology.
H.S. was involved in software.
Y.S. was involved in visualization.
L.Z. was involved in resources.
Z.W. was involved in supervision.
Q.G. was involved in project administration.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.