
Abstract
Purpose:
Dissecting and ligating the splenic artery is crucial for bleeding control during laparoscopic splenectomy (LS). However, for patients with portal hypertension from liver cirrhosis, it is difficult for identification and ligation because the splenic vessel is circuitous and dilated. The aim of this study was to describe a simple technique of constructing a tunnel behind the tail of the pancreas for occluding the splenic vessels during LS in patients with portal hypertension.
Materials and Methods:
The clinical data of 61 patients who underwent LS from April 2016 to January 2017 were retrospectively analyzed. In 27 patients, the tunnel construction (TC) behind the tail of the pancreas approach was performed owning to difficulty in dissecting and ligating the splenic artery (TC group), including 17 patients who received the TC method directly and 10 patients who received the TC method after trying to dissect the splenic artery. The remaining 34 patients underwent traditional ligating of the splenic artery (LA group). The peri- and postoperative outcomes of operative time, blood loss, conversion rate, postoperative oral diet intake, postoperative hospital stay, and postoperative complication rate of the two groups were analyzed. All the operations were completed by the same group of surgeons.
Results:
All 61 operations were successfully completed. Compared with patients in the LA group, patients in the TC group had less blood loss (120.37 ± 40.74 mL versus 162.65 ± 87.47 mL; t = −2.317, P = .024). There was no statistical difference of operative time, conversion rate, complication rate, postoperative hospital stays, and follow-up between the two groups.
Conclusions:
The technique of constructing a tunnel behind the tail of the pancreas for occluding the splenic vessels was effective and safe in those patients whose splenic artery was difficult to dissect and ligate.
Introduction
Since laparoscopic splenectomy (LS) was first reported in 1992, the technique has become a well-accepted procedure and gradually replaced traditional open splenectomy in most centers. 1 By now LS has become the standard approach for removing normal-sized spleens due to its advantages, which include smaller incisions, less trauma and pain, and quicker recovery.2–5 However, its application in patients with megalosplenia and portal hypertension remains controversial. Swollen spleen will occupy the space of the abdominal cavity, which increases the difficulty and risks of the laparoscopic surgery. The high risk of bleeding during such operations, mostly while managing the splenic pedicle, is the major obstacle.6–8
The European Association for Endoscopic Surgery (EAES) guidelines, 2 which has not been updated for over a decade in this field, still consider massive splenomegaly and portal hypertension secondary to cirrhosis, a contraindication to LS. However, with the development in laparoscopic instruments and the improvement of the skills and experience of surgeons, although it is still challenging, spleen size should no longer be considered the sole criterion for performing LS for patients with megalosplenia and portal hypertension.9,10
We have previously reported our technique of ligating the splenic pedicle en masse through the tunnel behind the spleen and the gap above the splenic pedicle during LS which can reduce the risks of bleeding when dissecting spleen pedicles.11,12 However, it is still difficult and challenging to ligate the splenic artery in patients with portal hypertension.13,14 To overcome this problem, we devised a simple vascular occlusion technique through the tunnel behind the tail of pancreas, which can produce equivalent results to the ligation of the splenic artery. In combination with ligation of the splenic artery first, this technique ensures bleeding control.
Patients and Methods
Ethical Statement
The Ethics Review Board of Wuhan Union Hospital approved this study.
Patients
Between April 2016 and January 2017, 61 consecutive patients with portal hypertension caused by cirrhosis underwent LS at the Hepatobiliary Surgery Center, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China. Of these, 27 patients' operations involved the tunnel construction (TC) behind the pancreatic tail technique (TC group). The remaining 34 patients underwent conventional ligation of the spleen artery (LA group). Preoperative imaging and laboratory examinations included computed tomography (CT) and/or magnetic resonance imaging (MRI), three-dimensional reconstruction, hepatitis B and C virus serologies, and other routine biochemical tests.
Selection criteria
All patients who underwent LS met the following inclusion criteria: (1) severe thrombocytopenia and or cytopenia due to hypersplenism (a platelet count <30 × 109/L or a white blood <30 × 109/L), (2) no serious organ damage, (3) no history of recurrent spontaneous bacterial peritonitis, (4) no history of abdominal surgery, and (5) liver function of Child–Pugh A or B.
TC group met one or more of the following inclusion criteria: (1) Splenic artery variation confirmed by preoperative three-dimensional reconstruction; (2) Easy bleeding when dissecting splenic arteries, which is rich in nourishing blood vessels; (3) Severe varicosity of splenic vessel, and (4) with the history of therapeutic splenic artery embolization.
This retrospective study was conducted according to the principles of the Declaration of Helsinki. The Ethics Review Board of Wuhan Union Hospital approved this study.
Operative procedures
Patients were placed in the right lateral recumbent position with their heads at a 30°angle. The intrabdominal pressure was maintained at 12 mmHg. The positions of the five trocars are shown in Figure 1.
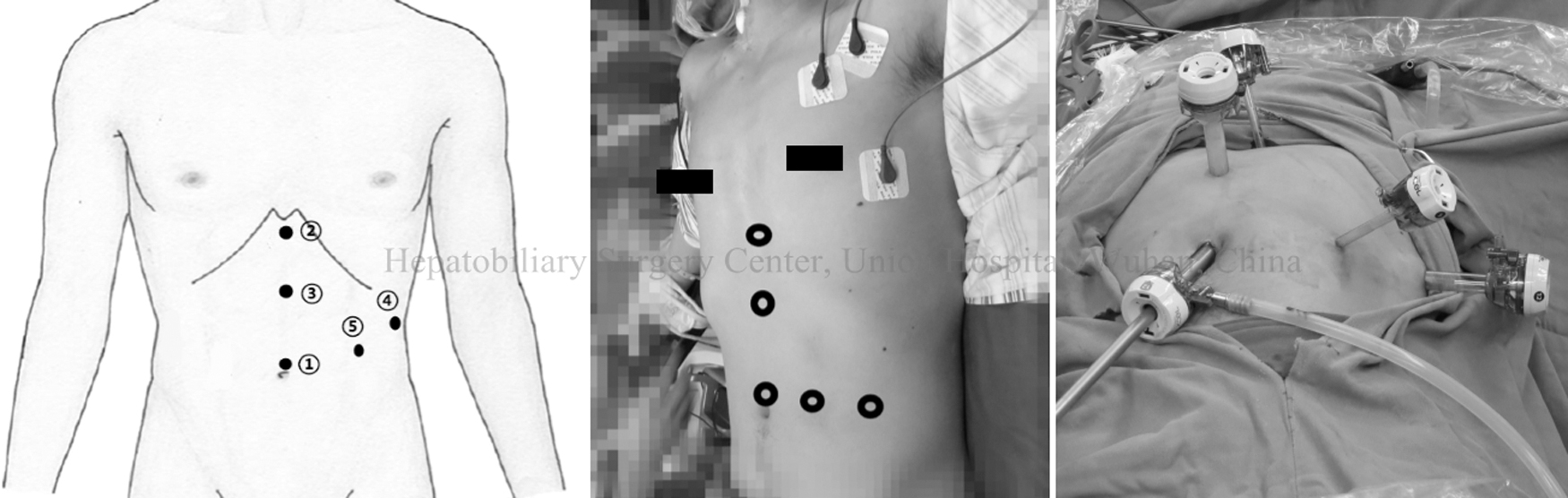
Trocar sites. ① above the navel (10 mm); ② below the xiphoid process (12 mm); ③ between the previously mentioned two location (5 mm); ④ below the left rib margin (lower edge of the spleen) and along the anterior axillary line (5 mm); ⑤ between the first and fourth location (12 mm).
At the start of the operation, the splenic artery was dissected and ligated with a clamp in patients in the LA group. While in the TC group, a tunnel was constructed behind the tail of pancreas with a Goldfinger dissector (Kangji Medical, Hangzhou, Zhejiang; Fig. 2a). To construct the tunnel, the transverse mesocolon was dissected near the pancreas's lower edge (Fig. 2b). The Goldfinger dissector was then inserted into the space behind the tail of the pancreas and a tape was pulled through the tunnel to occlude the splenic artery and vein, which was then able to control the splenic artery and vein (Fig. 2c). Another tunnel was then created behind the splenic pedicle (Fig. 3b) by passing the Goldfinger dissector through the gap above the splenic pedicle (Fig. 3a).8,9 An EC60A laparoscopic linear vascular stapler (Johnson, New Brunswick, NJ, USA) was then used to divide the splenic pedicle en bloc (Fig. 3d). Finally, the spleen was placed in a retrieval bag and morcellated for removal through a 2 cm incision above the navel.
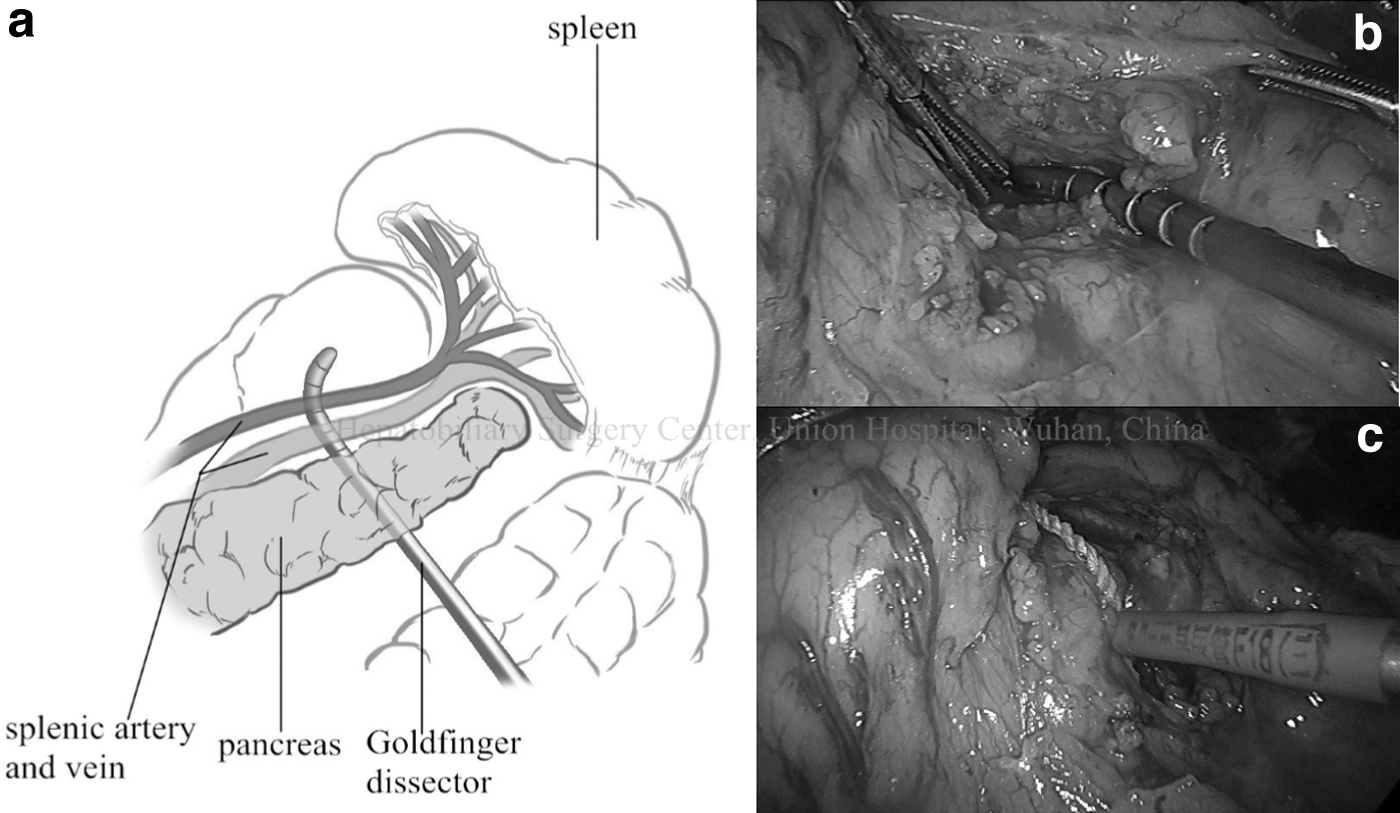
Building the tunnel behind the tail of pancreas to ligate splenic artery and vein.
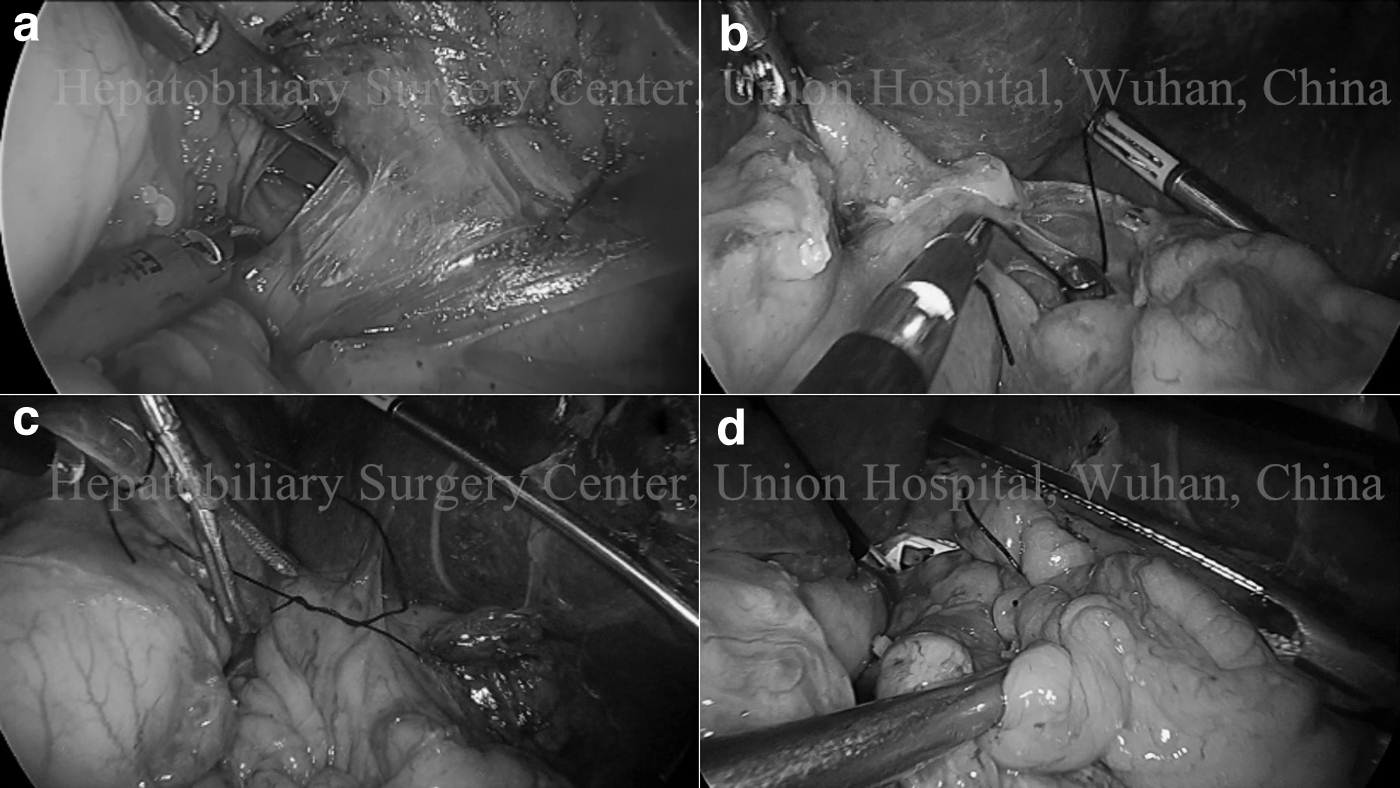
Create another tunnel behind splenic pedicle by Goldfinger Dissector and divide the splenic pedicle.
Follow-up
All patients were examined every 3 months during the first postoperative year of follow-up. In the second year, the patients were examined every 6 months. Liver function tests, routine blood tests, and portal venous ultrasound (or CT) were performed during the follow-up examinations. Hepatitis B/C serological markers and quantitative virus tests were also performed in patients with chronic viral hepatitis. In patients with portal vein thrombosis or recurrence of upper gastrointestinal bleeding, an individualized therapy plan was put in place based on the patient's condition. The patients were followed by telephone, and the WeChat application up until October 2017.
Data collection
The following outcome variables were analyzed: intraoperative blood loss, operation time, postoperative complications, time of postoperative oral diet intake, postoperative hospital stay, occurrence of portal vein thrombosis, and recurrence of upper gastrointestinal bleeding.
Statistical analyses
All analyses were performed with SPSS 17.0 software (IBM Corp, Armonk, NY, USA). Numerical data were expressed as
Results
The TC group included 19 men and 8 women with ages ranging from 39 to 70 years (55.19 ± 9.53 years). Liver function was Child–Pugh A in 21(77.8%) and Child–Pugh B in 6 (22.2%). Liver cirrhosis was caused by hepatitis B virus infection in 21 patients, hepatitis C virus infection in 3, alcohol in 2, and schistosome in 1. The mean spleen length was 25.86 ± 4.12 cm (measured with either CT or MRI). In the LA group, there were 22 men and 12 women with ages ranging from 25 to 74 years (53.24 ± 10.05 years). Liver function was Child–Pugh A in 28 (82.4% and Child–Pugh B in 6 [17.6%]). Liver cirrhosis was caused by hepatitis B virus infection in 27 patients, hepatitis C virus infection in 3, alcohol in 3, and schistosome in 1. The mean spleen length was 24.81 ± 5.16 cm (measured with either CT or MRI). There were no significant differences in demographic data between two groups (Table 1).
Patient Demographics and Clinical Data
Values are expressed as mean ± SD or number (percentage).
Student's t-test except.
χ 2 test.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; HBV, hepatitis B virus; HCV, hepatitis C virus; LA, ligating of the splenic artery; SD, standard deviation; TC, tunnel construction.
All 61 operations were successfully completed without the need for conversion. Of these 27 patients in the TC group, the splenic artery was difficult to dissect: (1) the splenic artery arises from the superior mesenteric artery, 1 patient; (2) easy bleeding when dissecting the splenic artery, 10 patients; (3) preoperative examination revealed severe varicosity of splenic vessels, 10 patients, and (4) splenic artery embolization before surgery (4–27 months before surgery), 6 patients. Three of the 6 patients in the fourth situation also had severe varicosity of splenic vessels, and we classify them in the fourth situation. In situation of one, three, and four, we choose the TC method directly, whereas, if it was easy bleeding when we tried to dissect the splenic artery, we switch to the TC method as well. Compared with patients in the LA group, patients in the TC group had less blood loss (120.37 ± 40.74 mL versus 162.65 ± 87.47 mL; t = −2.317, P = .024).
There was no statistically significant differences in operative time (80.55 ± 12.31 minutes versus 74.41 ± 14.94 minutes, t = 1.721, P = .09), postoperative oral diet intake (3.44 ± 1.28 days versus 3.18 ± 1.27 days, t = 0.817, P = .417), postoperative hospital stay (6.41 ± 1.89 days versus 7.12 ± 2.13 days, t = −1.360, P = .179), and postoperative complications between the two groups (25.9% versus 29.4%, χ 2 = 0.091, P = 0.763). Postoperative complications occurred in 7 patients in the TC group (pleural effusion in 3, deep vein thrombosis [DVT] in 1, ascites in 1, and pneumonia in 2) and 10 in the LA group (pleural effusion in 1, DVT in 4, ascites in 4, and pneumonia in 1). All cases of pleural effusion were Grade I according to the Clavien–Dindo classification 15 and resolved without special treatment. All incidences of DVT, ascites, and pneumonia (Grade II) resolved after receiving medical treatment (Table 2).
Intraoperative Data and Postoperative Data
Values are expressed as mean ± SD or number (percentage).
Student's t-test except.
χ 2 test.
LA, ligating of the splenic artery; SD, standard deviation; TC, tunnel construction.
Out of 27 patients in the TC group, 26 (96.3%) were followed up for 10–15 months (12.37 ± 1.50months). In the LA group, 31/34 patients (91.2%) were followed up for 9–16 months (12.68 ± 1.93months). Variceal rebleeding occurred in 2 patients in the TC group and 1 in the LA group. One patient received a liver transplant, 1 underwent emergency endoscopic hemostasis while on the waiting list, and 1 died at home before reaching a hospital. Portal vein thrombosis occurred in 3 patients in the TC group and 5 in the LA group, all of whom received oral medication treatment (warfarin in 2, and rivaroxaban in 6; Table 3).
Follow-Up Data
Values are expressed as mean ± SD or number (percentage).
χ 2 test except.
Student's t-test.
LA, ligating of the splenic artery; SD, standard deviation; TC, tunnel construction.
Discussion
Hypersplenism is a common complication in patients with portal hypertension due to liver cirrhosis, and it has a greater risk of bleeding when the platelet count is <30 × 109/L.16,17 Different from the traditional view, LS for liver cirrhosis and portal hypertension is now considered safe, effective, and minimally invasive.7,18–20 In addition, Yamamoto et al. reported that LS may potentially improve liver function at 1 year after surgery in patients with Child–Pugh class B cirrhosis. 21 In patients with megalosplenia, the dilated splenic vessels could easily rupture leading to uncontrollable massive hemorrhage. Therefore, manipulating the splenic pedicle in these patients is extremely risky.22,23 We had previously reported a novel method for performing LS successfully in patients with megalosplenia based on constructing a tunnel behind the splenic pedicle, penetrating through the gap above it, to allow division of the pedicle en bloc.11,12 Ligation of the splenic arteries is considered to be crucial for bleeding control during LS by blocking blood flow to the spleen. 24
Furthermore, it can cause the spleen to shrink, facilitating its resection. However, the ligation of splenic arteries is still challenging and risky in patients with portal hypertension, so an alternative technique for controlling the splenic vessels is needed especially for patients in whom the ligation is difficult and easy bleeding.
Pringle's maneuver is considered to be the classical approach for reducing bleeding during liver parenchymal transection by clamping the inflow vessels through the space behind the hepatoduodenal ligament. 25 With this technique in mind, we set out to develop a similar approach for controlling the splenic artery. There is an avascular space behind the tail of pancreas over which the splenic artery courses slightly above the pancreas.13,14 A tape crossing through this tunnel dissected from the space can ligate the artery and vein en masse. For patients in which splenic arteries cannot be identified and ligated, this method can provide effective arterial occlusion. Besides, it can also control the uncontrollable massive hemorrhage while dissecting the splenic vessels by constricting the tape, thus avoiding conversion. Furthermore, this maneuver also allows for the splenic veins to be effectively controlled.
In our experience, constructing the tunnel was feasible and simply performed in all patients in the TC group, and the mean intraoperative blood loss volume of the TC group was less. We considered this to be a result of occluding the splenic vessels in advance without dissecting the splenic artery. Compared with other five studies from China that included patients with portal hypertension and liver cirrhosis undergoing LS,26–30 the blood loss volume of TC group had no significant difference with their results (120.37 ± 40.74 versus 150 ± 110, 150.6 ± 130.4, 162 ± 126 and 150 ± 146.1, P > .05, versus 70.3 ± 36.9, P < .05). However, it is important to note that the length of spleen in these studies is lesser than ours (25.86 ± 4.12 cm versus 22.4–23.9 cm, standard deviation not acquired). This also seems to indicate that, for a spleen of the same size, our technique could reduce intraoperative blood loss. There were no statistically significant differences in the operation time, postoperative oral diet intake, postoperative hospital stays, and postoperative complications between the two groups.
In addition, no cases of postoperative pancreatic fistula occurred. The tunnel was constructed with blunt dissection using the Goldfinger dissector, which should not damage the pancreas as it passes through the natural space behind it. On the other hand, long-term follow-up did not demonstrate any significant differences in outcomes between the two groups. Based on the aforementioned results, our TC approach has demonstrated comparable results to traditional splenic artery ligation.
Portal vein system thrombosis (PVST) has been reported as a frequent and could be a life-threatening complication in patients with advanced cirrhosis. PVST is more frequent after LS than open splenectomy, 31 but rarely reported after LS in spleen rupture or hematologic diseases, which might be related to the pathophysiological features of portal hypertension such as increased plasma viscosity, recovery of coagulation function, and sharply elevated platelets.32,33 In our study, 11.5% and 16.1% patients were diagnosed of PVST during the follow-up in TC group and LA group, respectively, for a total of 15%, and it is relatively low compared with the prevalence of 5%–37.7% reported in other studies. 34 After standard anticoagulant therapy, these patients showed obvious improvement without aggravation. In our experience, early postoperative prophylactic anticoagulation and physical prevention could effectively reduce the perioperative and postoperative incidence of PVST.
Our study has several limitations. It is a retrospective analysis and the sample size was relatively small. In addition, the study lacked complete follow-up data. To further prove and generalize this technique, larger sample sizes and prospective studies are needed.
In conclusion, the TC technique is a safe and simple method for controlling bleeding during LS as effectively as traditional splenic artery ligation, and even better for those patients whose splenic artery was difficult to dissect. Among the method's advantages are utilization of the natural avascular space behind the pancreas, the ability to occlude the splenic artery and vein en masse with a tape through the tunnel, and avoiding the risk of bleeding while attempting to identify and ligate aberrant splenic arteries.
Footnotes
Authors' Contributions
Y.C. and G.C.: study conception and design and drafting of article.
Q.Q.: analysis and interpretation of data and acquisition of data.
Y.T. and T.W.: acquisition of data and critical revision of article.
C.W.: study conception and design and critical revision of article.
Ethics Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Institutional and/or National Research Committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.