
Abstract
Purposes:
We introduced a novel modified 2-cm single-port incision made by blunt separation minimizing intercostal muscle and nerve damage applied in video-assisted thoracoscopic surgery (VATS) segmentectomy, and compared it with the traditional single-port incision or the novel incision plus a 3-mm tiny port, aiming to explore a more minimally invasive single-port technique for VATS segmentectomy.
Materials and Methods:
We retrospectively analyzed the clinical data of 174 pulmonary ground glass nodule patients who received single-port VATS segmentectomy (54 modified 2-cm single port, 67 modified single port plus tiny port, and 53 traditional single port, respectively) in our medical center from May 2020 to December 2022. Three kinds of approaches were compared retrospectively, concerning their safety, feasibility, and postoperative pain.
Results:
There were no serious complications and mortality in either group. The blood loss, tube duration, and hospitalization time were comparable among the three groups (P > .05). The 2-cm single-port and 2-cm single-port plus tiny-port group were obviously more advantageous in the visual analog scores of postoperative pain, the wound numbness, incision healing and appearance than that in the traditional group (P < .05), while they were comparable. Notably, the operation time of the 2-cm plus tiny-port group was shorter than that of the 2-cm group (P < .05) and similar to the traditional single-port group.
Conclusions:
The 2-cm modified single-port applied for VATS segmentectomy is feasible and safe, and has obviously advantages in postoperative pain, numbness, and appearance of incision. With addition of tiny port, the convenience of the operation can be significantly increased without increasing pain. Our finding could provide a promising new incision mode for VATS segmentectomy.
Introduction
Lung cancer is the leading cause of cancer-related death worldwide. 1 With the implementation of chest computed tomography (CT) for lung cancer screening, more and more ground glass nodules (GGNs), which were the CT finding of early lung cancer, were detected; hence, the number and proportion of patients diagnosed with early-stage disease are increasing. 2 Surgical resection remains the only effective means of cure in the majority of patients with early-stage lung cancer, and segmentectomy is the optimal choice for lung cancer with GGNs.
Video-assisted thoracoscopic surgery (VATS) accounts for a major proportion of surgical approaches. 3 With the unremitting efforts of all thoracic surgeons, VATS has been evolved from multiple ports to single port.4–6 Single-port VATS lobectomy and segmentectomy have been rapidly adopted around the world since 2010.7,8 The incision size of the traditional single-port VATS lobectomy is usually 3–5 cm. However, the traditional single-port incision requires the chest wall and intercostal muscles to be cut by electrocautery, which could cause inevitable postoperative pain.
Theoretically, blunt separation causes less damage than electrocautery, for the latter induces extra thermal damage to muscles and nerves. Based on these, we developed a 2-cm modified incision technique for thoracoscopic surgery, which allows access to the thoracic cavity by blunt separation, thereby decreasing the size of the wounds and greatly reducing muscle and nerve injuries, and applied this technique in lobectomy. 9 However, we found that it was difficult to remove the pulmonary lobe from the 2-cm port sometimes. So we applied this technique in segmentectomy and achieved good results.
The 2-cm single port increases the operation difficulty and prolongs the operation time sometimes. Thus, we utilized a 3-mm tiny port, where a “pig tail” drainage tube was introduced postoperatively to place a 3-mm endoscopic instrument during operation, thereby increasing the convenience of the operation.
In this study, we retrospectively analyzed the clinical data of 174 pulmonary GGN patients who received single-port VATS segmentectomy (54 modified 2-cm single port, 67 modified single port plus tiny port, and 53 traditional single port, respectively) in our medical center from May 2020 to December 2022, aiming to explore a more reasonable incision mode for VATS segmentectomy for further minimal invasion.
Materials and Methods
Patients
We reviewed data of 174 patients who received single-port VATS segmentectomy in our center from May 2020 to May 2022, including 54 patients who underwent 2-cm modified single-port segmentectomy (modified group), 67 patients who underwent 2-cm modified single-port plus 3-mm tiny-port segmentectomy (modified plus group), and 53 patients who underwent traditional single-port segmentectomy (traditional group; Fig. 1). We started the 2-cm single-port and the 2-cm single-port plus 3-mm tiny-port surgical approaches in March 2019 and June 2019, respectively.
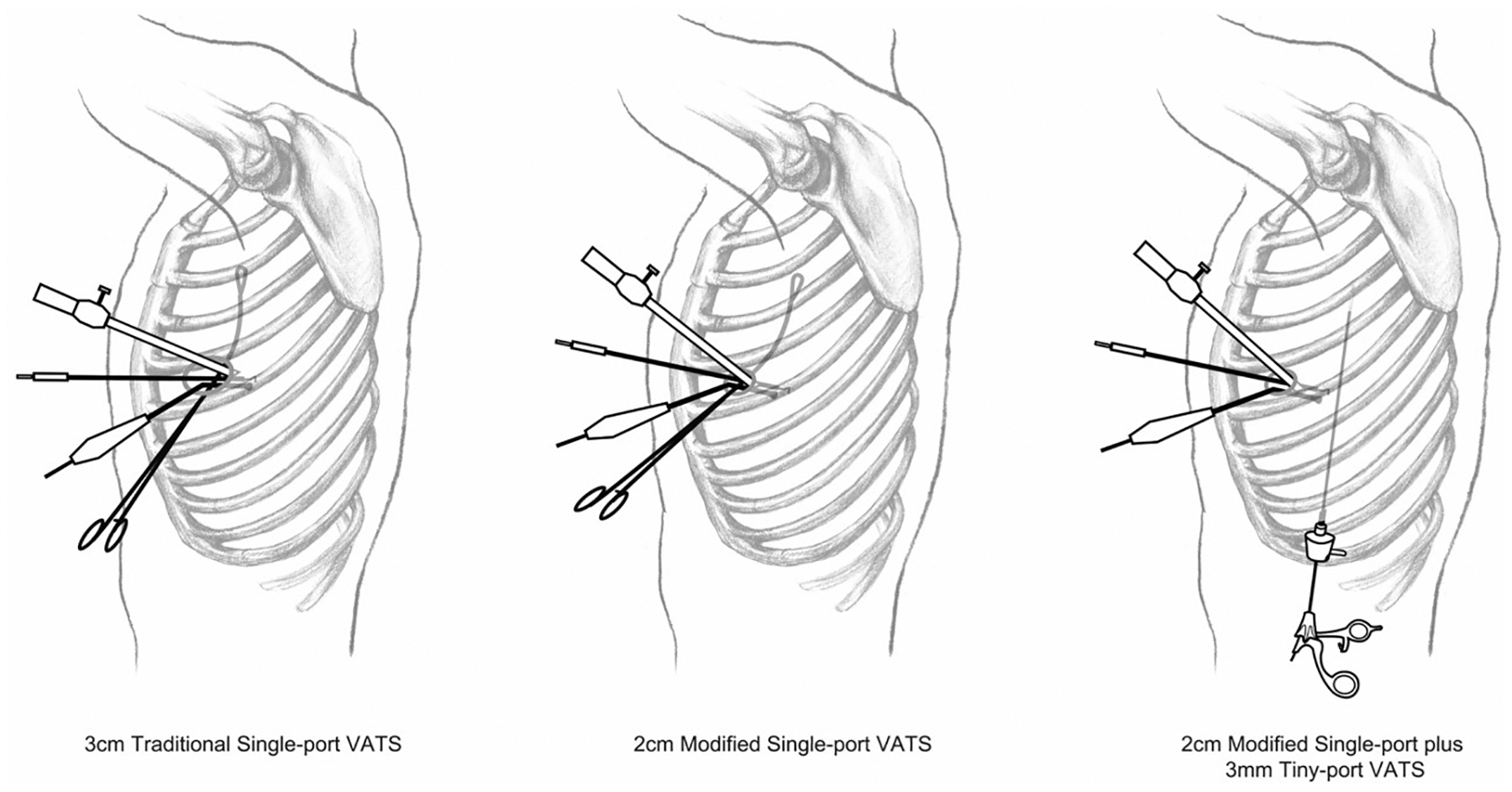
Procedures of single-port VATS segmentectomy. From left to right: 3-cm traditional single-port VATS, 2-cm modified single-port VATS, and 2-cm modified single-port plus 3-mm tiny-port VATS. VATS, video-assisted thoracoscopic surgery.
Before surgery, patients were fully informed about the advantages and disadvantages of the three surgical approaches. We followed the principle of respecting the patient's independent choice to decide which surgical procedure the patient would undergo. All operations were performed by the same medical team. This retrospective study was approved by the Renmin Hospital of Wuhan University review board. Each patient was treated in accordance with the ethical principles outlined in the Declaration of Helsinki. We obtained the consent of all patients.
The inclusion criteria included patients of age <70 years and >18 years; with pulmonary lesions involving GGNs of diameter <1 cm; with no obvious swollen lymph nodes in the chest; and with a preoperative clinical diagnosis of lung cancer with tumor node metastasis stage I. The exclusion criteria included patients with a history of chronic pain or mental illness; alcohol abuse, drug abuse; communication disorders; complete pleural adhesion, intolerance to one-lung ventilation, or severe thoracic deformities; who have received neoadjuvant chemotherapy or radiotherapy.
Study and operative methods
Each patient's clinical history was collected carefully before surgery. All patients underwent routine blood tests, liver and kidney function tests, arterial blood gas analyses, pulmonary function tests, bronchofiberscopy, electrocardiograms, echocardiography tests, and other examinations. No severe lung or heart disease was found in any of the patients before surgery. Head magnetic resonance imaging (MRI), chest and abdominal CT, and emission CT bone scans were also performed routinely to exclude distant metastasis. There were no contraindications to surgery. Before and after the operation, nurses provided pamphlets and verbal education to the patients, and coughing training was carried out routinely before the operation.
Surgery was performed under combined intravenous and inhalation anesthesia with double-lumen tracheal intubation and selective one-lung ventilation. After successful anesthesia and intubation, all patients received VATS segmentectomy and lymph node sampling.
The modified single-port VATS segmentectomy procedures were performed as previously described. 9 In brief, a 2-cm skin incision was made in the fourth or fifth intercostal spaces of the axillary midlines, and the subcutaneous tissue, the fibers of serratus anterior muscle, and the intercostal muscle were bluntly split apart by a curved kelly clamp (Fig. 2).
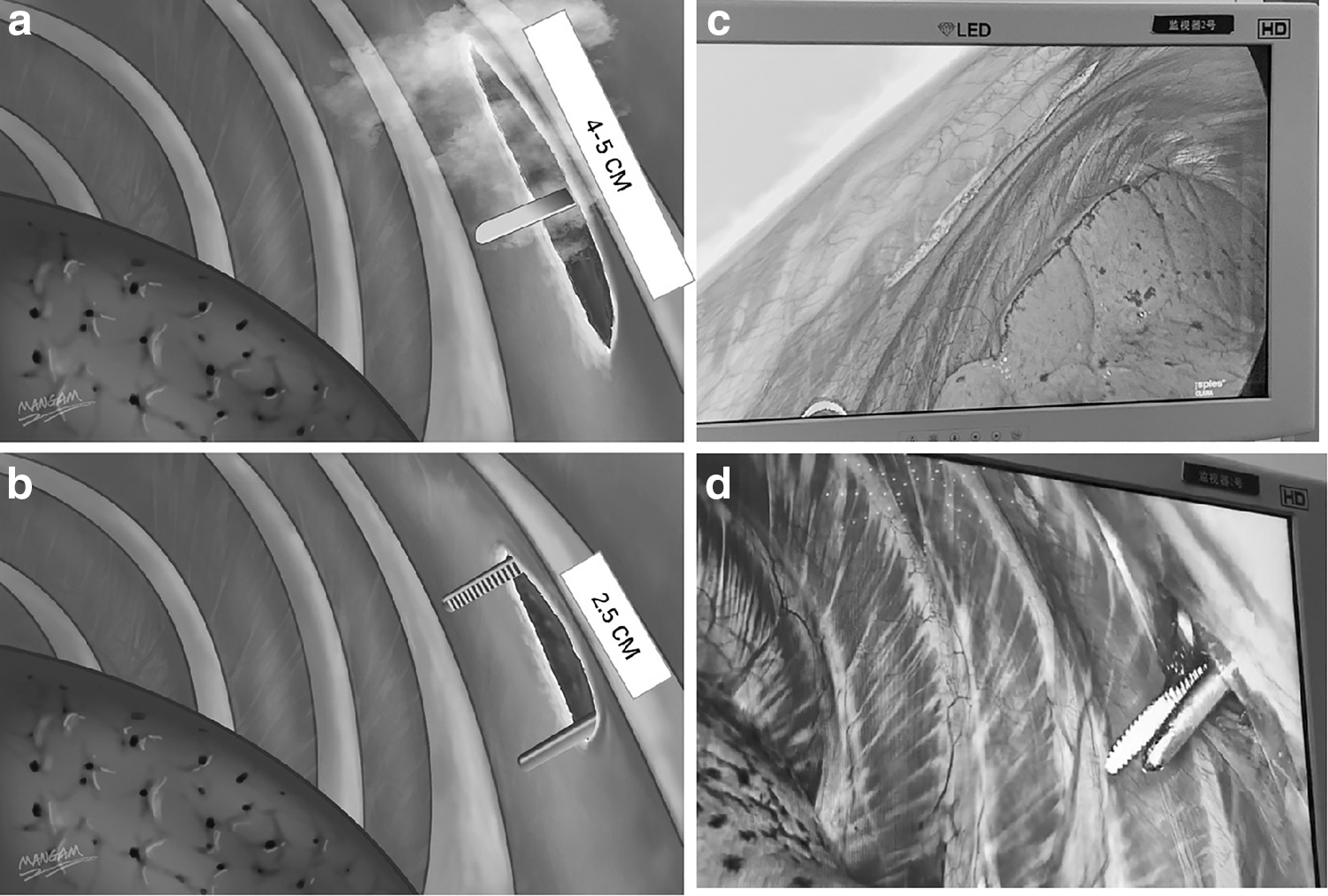
Two different approaches of making single-port incision of VATS:
When the clamp separated into the thoracic cavity, a plastic wound protector (NouDe Jiangxi China) was placed to distract the incision to form an average 2.5 × 1.5-cm port for operation. Usually, there were four instruments in the single port, including a 10-mm HD thoracoscopy (Karl Storz, Tuttlingen, Germany), a 5-mm double joint oval forceps, a 4-mm aspirator, and a 4-mm electric hook (Fig. 1).
Preoperative three-dimensional CT bronchography and angiography was performed before anatomical segmentectomy, which could reveal the anatomical structures and variations of the segmental bronchi/vessels and locate the pulmonary nodules for surgery planning. The vessels of pulmonary segment were ligated by silk and ultrasonic scalpel, bronchi and intersegmental border were transected by endo-stapler.
The intersegmental border was determined by clamping target segmental bronchi and inflating the pulmonary rather than inflation–deflation method. Hence, the target segment was deflation, which would be easier to remove than the inflatable one from the 2-cm port. Sampling of N1 and N2 station lymph nodes and intraoperative frozen section was routinely performed. Finally, the pulmonary segment was removed in a bag. After surgery, the muscles around the incision that without cautery could elastically retract.
In the modified plus group, a 3-mm endoscopic grasping forceps (Aesculap Germany) was placed in the 3-mm tiny port where a “pig tail” (8F) drainage tube would be placed after the operation. In this way, there were only three instruments in the 2-cm port. It could optimize surgery process and reduce the incision injury from squeezing by instruments. With the assistance of the 3-mm endoscopic grasping forceps, it was more convenient to dissect the segmental vessels and bronchus.
In the traditional group, the single-port incision was made as usual by electrocautery. The procedure of segmentectomy was similar to that of the modified single-port VATS.
After the operation, all patients were placed with a 26# chest tube in the single port and a pig tail (8F) drainage tube at the eighth intercostal space of posterior axillary line for drainage.
Main outcome measures
The following indicators were collected in all patients: operation time, intraoperative blood loss, chest tube duration, hospitalization time, postoperative pathology, incision seepage, poor healing, whether underwent intraoperative conversion to thoracotomy, whether underwent perioperative unplanned reoperation, whether received remedial analgesia. The degree of pain was evaluated at 9 a.m. from the first day after operation until third postoperative day, and then the degree of pain and wound numbness were evaluated 3 months postoperatively.
The degree of pain was assessed by a visual analog score (VAS), with a score of 0 indicating no pain and a score of 100 indicating the most severe pain possible. 10 The higher the VAS score, the more severe the pain. Wound numbness was defined as dull and reduced sensitivity around the skin incision after the operation.
Statistical analysis
Variables with normal and abnormal distributions were presented as mean ± standard deviation and median (range), respectively. All statistical analyses were performed using SPSS 22.0 statistical software (SPSS Inc., Chicago, IL, USA). A single-factor analysis of variance test was used for comparisons of body mass index (BMI; normal distribution variables) among the three groups.
The patient characteristics (gender, history of cigarette, and so on) and other categorical variables among the three groups were compared using the Pearson chi-square test or Fisher's exact test, and the Kruskal–Wallis test was used for abnormal distribution variables (age, operation time, and so on). The Least Significant Difference test was used for post hoc analysis. A P < .05 indicated a significant difference.
Results
In total, 174 patients successfully received single-port VATS segmentectomy, and had no serious complications and perioperative death. There were no significant statistical differences among the three groups in age, gender, BMI, smoking history, drinking history, using of sedatives, diabetes mellitus history, and preoperative sleep quality (all P > .05; Table 1).
Distribution of General Characteristics
BMI, body mass index.
Perioperative unplanned reoperation had no significant difference among the three groups. One patient in the modified group converted to double-port VATS, and 1 patient in each modified and modified plus group converted to thoracotomy (Table 2). There was no significant difference in blood loss among the three groups (P > .05). Notably, the operation time of the modified group was longer than that of the modified plus group and the traditional group (P < .05; Table 2).
Distribution of Surgical Characteristics
Changing approaches in operation refer to conversion to open thoracotomy or double-port VATS.
AAH, atypical adenomatous hyperplasia; Mia, minimally invasive adenocarcinoma; Tis, tumor in situ; VATS, video-assisted thoracoscopic surgery.
The total dose of sufentanil used within 72 hours, VAS scores on the first 3 days and the third month after surgery were lower in the modified and modified plus group than in the traditional group (P < .05), while they were comparable between the modified and the modified plus group (P > .05). In addition, the wound numbness 3 months after surgery was significantly less in the modified and modified plus group than in the traditional group (P < .05). The percentage of receiving remedial analgesia had no significant difference among the three groups (P > .05) (Table 3).
Postoperative Pain
When patients
VAS, visual analog score.
There were four cases of poor incision healing in the traditional group, but none in the modified and the modified plus group (P < .05). The tube duration and hospitalization time were comparable among the three groups (P > .05; Table 4).
Rehabilitation Index
When patients
Discussion
When making the traditional single port with electrocautery, it will inevitably damage intercostal nerve, and thus cause postoperative pain. To avoid intercostal nerve injury, subxiphoid incision is applied in VATS, but it is quite different in surgical route from traditional VATS and not widely accepted in pulmonary surgery. The modified 2-cm single port minimizes intercostal muscle and nerve damage, thereby reducing the size of the wounds and postoperative pain. 9
The surgical route was similar to the traditional single port, so it was more acceptable. However, it increases the operation difficulty and prolongs the operation time. The pulmonary lobe is very difficult to remove from chest cavity in the 2-cm single port. Thus, this single port seems to be more suitable for segmentectomy.
In the study, we applied this technique in segmentectomy or added a tiny port to reduce the difficulty of operation. According to our data, the 2-cm single-port incision had obvious advantages over traditional single-port incision in terms of less trauma and postoperative pain, and disadvantages in terms of poor convenience and costing longer operation time. Considering all the patients' need to place a “pig tail” drainage tube in eighth intercostal after operation, we used the tiny port to place a grasping forceps to help for traction and exposure during operation.
As expected, the 3-mm tiny port increased the convenience of the operation and significantly shortened the operation time. Notably, we found that adding the 3-mm tiny port did not increase postoperative pain. In addition, none of the modified group had complications of incision healing, while four cases (7.8%) of the traditional group had poor incision healing. The reason may be the muscles by blunt separation was less injured and would be more likely to retract automatically after surgery.
For GGN lung cancer, segmentectomy is the preferred surgical method. Overall, the operation through 2-cm single port is more difficult, so we should simplify the surgical procedures. In this study, we did not dissect intrasegmental veins and separated the intersegmental boarder by endostapler, while the targeted segment was deflated, which would be easier to remove from the 2-cm port than the inflated one.
In the 2-cm single port, segment of upper lobe and dorsal segment resection were simpler, while the basal segmentectomy was more difficult. The 3-mm tiny port would be very helpful in difficult situation. In line with the findings, we have routinely performed VATS using the 2-cm single-port method, including lung wedge resection, lung segment resection, and lobectomy surgery (suitable cases). When encountering difficult conditions such as pleural cavity adhesion and pulmonary fissure dysplasia during the operation, we will not hesitate to add the 3-mm tiny port to simplify the surgical operation.
Therefore, the three types of incisions were all suitable for VATS to implement segmentectomy for GGN lung cancer. Notably, the 2-cm modified incision was more advantageous in terms of postoperative pain and neat incisional appearance. When assisted with the tiny port, it significantly increased the convenience of surgery without increasing postoperative pain.
Conclusion
In conclusion, the 2-cm modified single port is a good novel approach to perform segmentectomy, and plus 3-mm tiny port significantly decreases the operation difficulty and time, and does not increase the postoperative pain and wound numbness. Thus, when difficult conditions are encountered during surgery, it is necessary to choose the 2-cm modified single-port plus 3-mm tiny-port surgical approach. We believe that this surgical method will be a promising new option for VATS segmentectomy.
Footnotes
Acknowledgment
The authors thank Wen Jing Han (MANGAM) from Wuhan University Press Co., Ltd for help in picture production.
Data Availability
The data that support the findings of the study are available from the corresponding author upon reasonable request.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by “the Fundamental Research Funds for the Central Universities” (2042022kf1094).