
Abstract
Background:
In pancreatic cancer surgery, tumor violation of blood vessels is often considered a contraindication to surgery, especially laparoscopic surgery. We have completed 17 cases of major venous repair or reconstruction during laparoscopic pancreatic surgery, and we believe that this surgical method may be safe and feasible based on the skilled laparoscopic techniques.
Materials and Methods:
Between January 2014 and March 2022, a prospective cohort of 17 patients underwent major venous repair or reconstruction in our department. Among them, 15 cases underwent laparoscopic pancreaticoduodenectomy, 1 case underwent laparoscopic distal pancreatectomy, and 1 case underwent laparoscopic central pancreatectomy. In all of these cases, the pancreatic tumor invaded either portal veins (PV) or superior mesenteric veins. Given these clinical situations, 13 cases accepted laparoscopic venous resection and reconstruction, and 4 cases underwent venous repair.
Results:
Ten of 17 patients (58.8%) were male. The mean age was 67.1 (range 57–81). All patients' operations were successfully completed without transit to open. The average blocking time of venous resection and reconstruction was 30.1 (range 15–41) minutes and the average time of venous wedge resection and stitching was 24.0 (range 18–30) minutes. After surgeries, there were no complications such as PV stenosis, bleeding, thrombosis, and liver failure. Thirteen patients died within 2 years because of the tumor recurrence, and 4 patients are currently followed by outpatient visits, with no obvious signs of tumor recurrence.
Conclusion:
Studies have shown that the reconstruction or repair of the major veins under laparoscopic surgery is safe and effective. We recommended that surgeons need to have the basics of open surgery in case laparoscopic surgery cannot be continued, and have proficient laparoscopic surgery techniques combined with extensive training to achieve a learning curve for vascular anastomosis. Clinical Trial Registration number: KY2021SL152-01.
The pursuit of minimally invasive surgery is the current mainstream. The possibility of performing laparoscopic pancreaticoduodenectomy (LPD) is a sign for a surgeon who is good at a laparoscopic technique. However, many surgeons have to transit to open surgery when tumor violates the portal vein (PV) or superior mesenteric vein during LPD surgery. Laparoscopic venous resection and reconstruction is an uncomplicated but difficult procedure, and only a few reports have been issued.1–4 We carried out 17 cases of tumor invasion of the veins in laparoscopic surgery, of which 4 cases were venous wedge resection and stitching, and 13 cases were venous resection and reconstruction. In this regard, we summarize the relevant experience and believe that performing LPD/laparoscopic distal pancreatectomy (LDP)/laparoscopic central pancreatectomy (LCP) with venous resection and reconstruction may be safe and feasible, which may provide some advice for the acquisition of this surgical method in the learning curve.
Materials and Methods
Between January 2014 and March 2022, 17 patients were admitted to the hospital. Preoperative examinations of all patients included blood routine, urine routine, fecal routine, biochemic routine, clotting function, tumor markers, hepatitis B three-series plus pre-S1 antigen, pretransfusion testing, chest tablets, electrocardiogram, enhancement computed tomography (CT), and enhancement of magnetic resonance imaging and magnetic resonance cholangiopancreatography. Preoperative diagnosis included 13 cases of pancreatic head cancer, 1 case of the lower bile duct cancer, 1 case of the duodenal papilla cancer, 1 case of pancreatic tail cancer, and 1 case of pancreatic body cancer. In 17 patients, the tumor was prompted to cling to or wrap around the PV/superior mesenteric veins, but did not invade the superior mesenteric artery (SMA). No patients received chemotherapy before surgery.
Laparoscopic surgery exclusion criteria
Laparoscopic surgery exclusion criteria include patients combined with severe cardiovascular diseases using anticoagulant drugs, America Society of Anesthesiologists score ≥4 points, invasion of SMA, distant metastasis of tumors, and other patients who were unable to withstand the carbon dioxide (CO2) pneumoperitoneum surgery.
The study was approved by the Ningbo Medical Treatment Center of Lihuili Hospital Ethics Committee. Written informed consent was obtained from the patients.
All methods were performed in accordance with the relevant guidelines and regulations.
Surgery technique
The patient was intubated in a supine position with a 20° head-up tilt. After undergoing tracheal intubation and induction of general anesthesia, a CO2 pneumoperitoneum was created through an open Veress-assisted technique. A 30° telescope was used to inspect the peritoneal cavity. Five trocars were used: a 10-mm telescope trocar in the midline above the umbilical incision; two cranially placed 5-mm ports in the left and right anterior axillary lines, and two cranially placed ports 5 mm to the left and 10 mm to the right of the rectus muscles at the level of the umbilicus (Fig. 1). Conventional LPD or LDP or LCP was performed. We performed venous resection and reconstruction if the tumor enveloped the veins, whereas, we performed the venous wedge resection and stitching (repair) if the tumor was confirmed to be an adhesion to the veins and could not be separated in surgery.
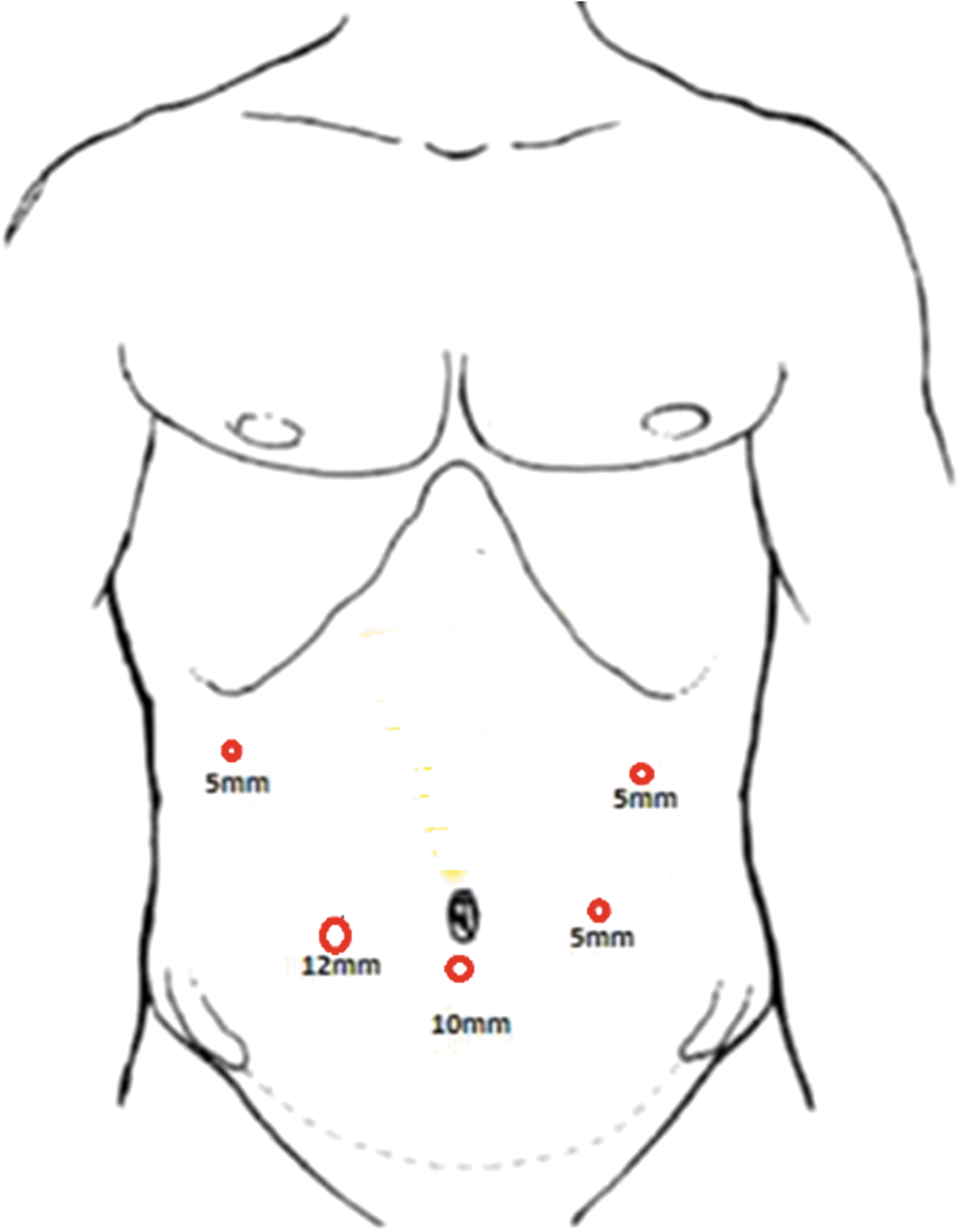
The position of trocars for LPD/LDP/LCP. LCP, laparoscopic central pancreatectomy; LDP, laparoscopic distal pancreatectomy; LPD, laparoscopic pancreaticoduodenectomy.
Reconstruction technique
The “two-point method” was used (Fig. 2). The 4-0 Prolene line was first stitched on the left and then pulled by the assistant, and then another 4-0 Prolene line was stitched but not knotted on the right side, also pulled by the assistant (Fig. 3A). Then the 4-0 Prolene line was stitched in the left back wall after a stitch, followed by a continuous stitch from left to right (local heparinization during the stitching process), which was not knotted after the stitch to the right, and was pulled by the assistant (Fig. 3B). The front wall was stitched to the right using the same method. After the stitching was completed, the venous vascular clip was released to fill it, and finally all right-side stitches were knotted (Fig. 3C); if there was local bleeding in the veins, it could be reinforced by additional stitching. Finally, the veins were observed after the stitching (Fig. 3D).
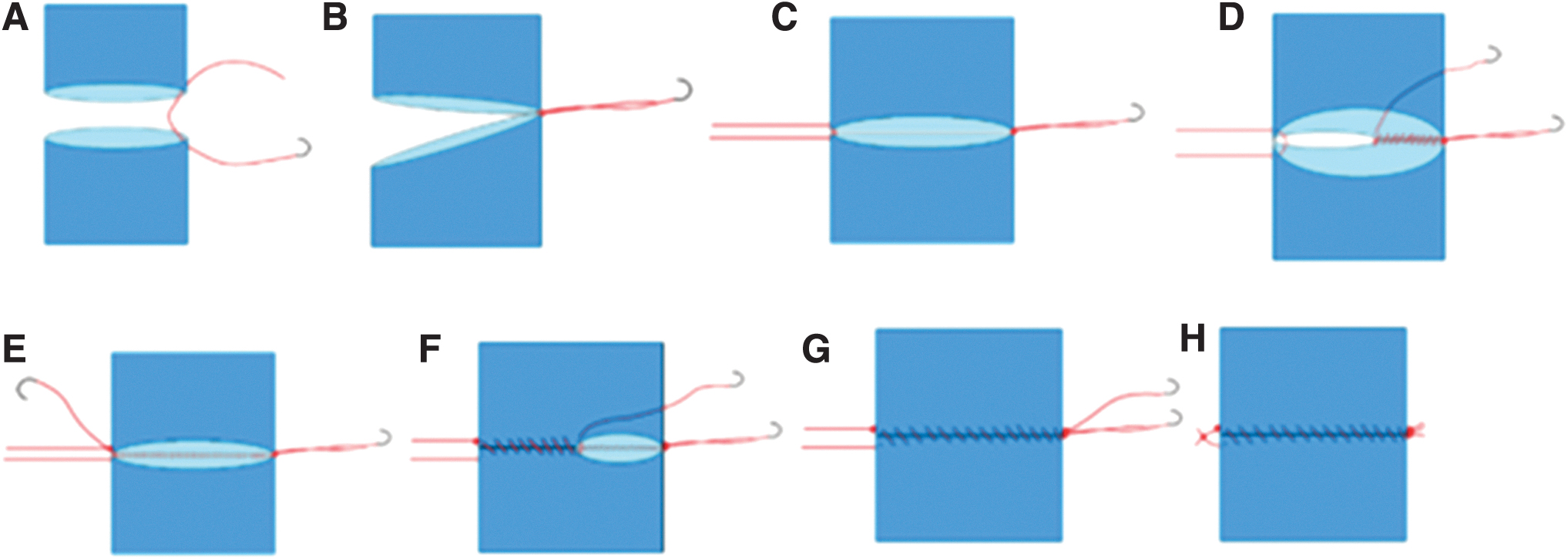
The “two-point method” of venous reconstruction.
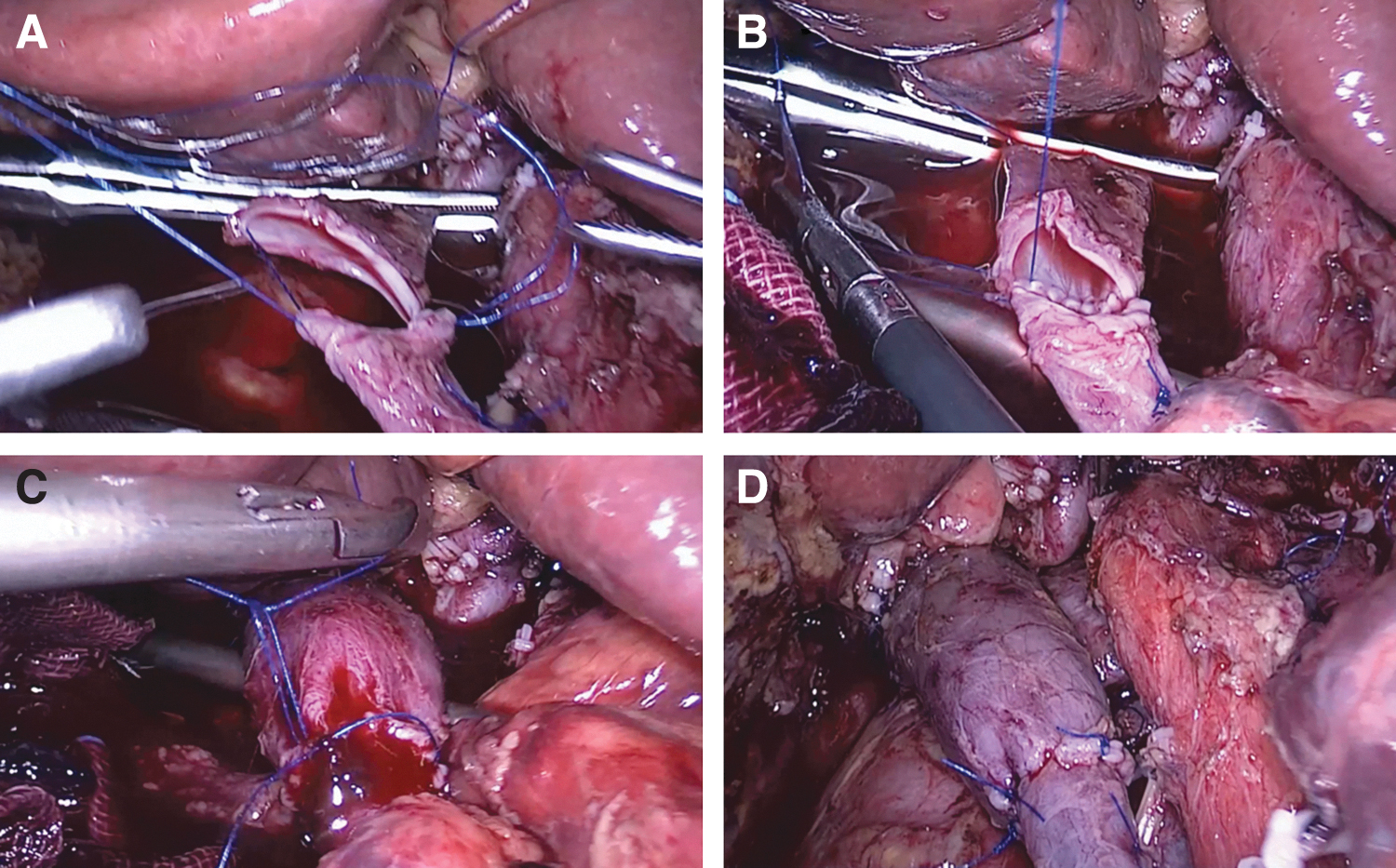
Major laparoscopic venous reconstruction.
Repair technique
The PV was clamped with a blood vessel clip after the laparoscopic scissors cutoff the infringing veins and tissues (Fig. 4A), followed by continuous stitching by a 4-0 Prolene line from one side to the other side. Then continuous stitching to the original side for knots, and finally the veins were observed after the stitching (Fig. 4B, C).

Major laparoscopic venous repair.
Statistical analysis
Data were analyzed using SPSS for Windows version 20 (IBM Ltd., Armonk, NY, USA). Qualitative variables were analyzed by calculating absolute and relative frequencies and were compared with the χ 2 test. Quantitative variables were expressed as mean or median and standard deviation and compared with the Student's t-test. Statistical significance was considered for P < .05.
Results
A total of 17 patients were included in the study, including 10 males and 7 females, with an average age of 67.1 (range 57–81). A total of 4 patients underwent venous wedge resection and suturing (2 LPD surgeries, 1 LCP surgery, 1 LDP surgery), and 13 patients underwent venous resection and reconstruction (all LPD surgeries).
All operations were successfully completed without transition to open surgery. The average surgery time was 495.9 minutes (range, 260–965 minutes), and the average estimated intraoperative bleeding volume was 378.9 mL (range, 100–1200 mL). A total of 9 patients received intraoperative blood transfusion, with an average volume of 600 mL (range, 200–1900 mL). In venous wedge resection and suturing surgeries, the mean venous blocking time was 24 minutes (range, 18–30 minutes). In venous resection and reconstruction surgeries, the mean venous blocking time was 30.1 minutes (range 15–41 minutes), and the mean length of venous resection was 2.75 cm (range, 1.5–4 cm).
We evaluated the PV with bedside ultrasound on each day 1–4 postoperatively and with an enhanced CT on day 5postoperatively, without venous stenosis, bleeding, thrombosis, and liver failure. The average length of hospital stay was 20.7 days (range, 13–56 days), without perioperative period, and death 30 days after discharge.
The average maximum tumor size was 3.8 cm (range 2.0–7.0 cm) by detecting postoperative pathological samples. The tumor style is as shown in Table 1. Thirteen cases of tumor are pancreatic ductal adenocarcinoma, 1 case is duodenal papillary carcinoma, 1 case is undifferentiated cancer, 1 case is the common bile duct adenocarcinoma, and 1 case is pancreatic neuroendocrine carcinoma.
Perioperative Data of Patients
ALB, albumin; ALT, alanine aminotransferase; AST, aspertate aminotransferase; BMI, body mass index; F, female; LCP, laparoscopic central pancreatectomy; LDP, laparoscopic distal pancreatectomy; LPD, laparoscopic pancreaticoduodenectomy; M, male; PLT, platelet; PT, prothrombin time; PV, portal veins; SMV, superior mesenteric veins; TBil, total bilirubin.
We divided the patients who underwent LPD with venous resection and reconstruction surgery into two groups (Table 2): the first group includes 5 cases and the other group includes 8 cases. We found that the two groups of patients were not statistically significant in terms of general data, operation time, intraoperative blood loss, tumor size, and postoperative hospital stay, but there was statistical significance in terms of venous blocking time (36.2 minutes versus 26.3 minutes, P = .007).
Comparison of Perioperative Data in Two Groups of Patients with Venous resection and Reconstruction Surgery
Bold value indicates the blocking time of the two groups was statistically significant.
ALB, albumin; ALT, alanine aminotransferase; AST, aspertate aminotransferase; BMI, body mass index; PLT, platelet; PT, prothrombin time; TBil, total bilirubin.
All patients got outpatient review of blood routine, biochemic, tumor markers weekly during chemotherapy, and monthly review of full abdominal enhancement CT. Thirteen patients died within 2 years because of the recurrence of the tumor, while 4 patients are currently followed up as outpatients without signs of tumor recurrence.
Discussion
Surgery is recognized as the only possible method of cure for pancreatic cancer, and the purpose of vascular resection is to obtain a R0 resection. 3 Fortner first reported in 1973 the use of regional pancreatic excision to expand the range of lymph node, and combined removal of tumor-invasive blood vessels for the treatment of difficult-to-remove pancreatic cancer. More and more experts now support the feasibility and safety of intravenous resection and reconstruction in Pancreaticoduodenectomy (PD) surgery,5,6 which can increase the R0 resection rate. The tumor previously considered nonremovable can be removed, which increases the possibility of cure. With the progress of surgical technology and comprehensive treatment, the perioperative prognosis of patients who were combined with venous resection and reconstruction PD surgery is good, and the long-term prognosis of some patients is similar to that of patients with conventional PD surgery.7,8 Ishikawa 9 found that even if the tumor and veins can be separated, cancer cells may remain in the vein wall, which can lead to postoperative metastasis.
To achieve R0 excision, researchers believe that regardless of vascular invasion, for a complete R0 excision, under the premise of ensuring surgical safety, preventive intravenous resection and reconstruction should be performed during surgery. 8 Our limited experience is that wedge resection of veins may be a better option, for surgery is simpler than venous resection and reconstruction, and does not require the blocking of veins. Of course, intraoperative freezing pathology is needed to confirm the removed venous wall with no residual tumor cells, otherwise the resection and reconstruction of veins are required. In this study, we only decided to perform venous resection and reconstruction or repair surgery for patients whose tumors clearly invaded veins (i.e., the tumors could not be separated from veins during surgery). Patients whose tumors could be separated from veins were excluded from this study. In 4 cases of venous repair patients, intraoperative frozen pathology was performed on the venous margins, which were negative. Therefore, we did not decide to do further venous resection and reconstruction.
The major venous resection and reconstruction in LPD was first reported by Professor Kendrick and Sclabas 10 in 2011, who believed that it was safe and feasible. Since then, the number of experts have published related reports. We have tried venous resection and reconstruction under LPD since 2014, 11 we believe that as long as laparoscopic technology reaches a certain level, LPD and open surgery may have similar indications. However, without a wealth of PD experience and the basic skills of stitching under laparoscopy, blind attempts are forbidden. Preoperative multidisciplinary treatment also has a key role for patients treatment, such as careful reviews and studies of the relevant imaging data, accurate evaluation of the relationship between tumor range and surrounding blood vessels, as well as lymph nodes, and distant metastasis with the imaging department, which helps surgeons to prepare for the surgery following. As for nonremovable tumor, we can get gastroenterology departments help for obtaining the pathology by ultrasound endoscopic puncture and then combine with chemotherapy department to lower the tumor stage.
Choi et al. 12 have found that complex LPDs can be performed since the 100th case. According to our single-center experience, if we want to perform LPD with venous resection and reconstruction, we can begin with open surgery with venous resection and reconstruction, then transit to venous wedge resection and stitching under LPD, then practice in animal experiments, and finally perform LPD with venous resection and reconstruction. Before we decided to do LPD, we first tried the PV resection and reconstruction of the pig, because the experimental pig did not have a tumor, so the PV of a pig could be repeated several times until the PV could not be anastomosed due to excessive tension. In this article, after comparing the PV blocking time of the first 5 cases and the last 8 cases, we found that there were statistical differences (p = 0.007). So, we believe that the learning curve of LPD with venous resection and reconstruction surgery is 5 cases. Of course, it should be mentioned that this learning curve is for a surgeon with extensive laparoscopic experience. For novice surgeons, this learning curve may be longer.
Our experience for venous resection and reconstruction under LPD is: (1) When blocking veins, we choose to use a larger blood vessel blocking clip, so that the clip will not easily slide intraoperatively, and the operation will be convenient during stitching. (2) We control the needle pitch between 0.5 and 1.0 mm. If the pitch is too narrow it might cause the veins to narrow. If the pitch is too long, it might cause the matching mouth bleeding. We control the stitching margin between 1 and 2 mm, too short may cause the venous stenosis, too long may cause the high anastomotic pressure. (3) During the stitching process, the assistant needs to heparinize the anastomosis to prevent venous thrombosis. (4) A skilled team is needed. (5) Some experts suggested that the blocking time should be controlled within 60 minutes, and some suggested that the time of blocking should be within 30 minutes.7,13 Our average blocking time was 30.1 minutes, and during the operation, no small intestine ischemia or necrosis was observed, and no signs of liver failure were evident afterward. After all, only good laparoscopic technology can shorten the time of venous anastomosis.
(6) There are reports 14 suggesting that even venous defects up to 7–8 cm can still be directly anastomosed, while most experts currently believe that <4 cm is appropriate. For more than 4 cm may require additional artificial blood vessels, 2 so the full evaluation of preoperative imaging is particularly important. (7) For patients who have had a period of chemotherapy before surgery, we recommend careful use of venous resection and reconstruction under laparoscopy, because those patients have more fragile tissues, and severe adhesion during surgery. Laparoscopic surgery very easily leads to venous damage and hemorrhage during surgery. In this study, none of the patients received neoadjuvant chemotherapy because we had no confidence because of the risks of surgery after chemotherapy for such a complex procedure.
In conventional LPD surgery, lymph node dissection was performed in accordance with International Study Group of Pancreatic Surgery (ISGPS) guidelines for No. 5, 6, 8a, 12b1, 12b2, 12c, 13a, 13b, 14a, 14b, 17a, and 17b groups. For patients with tumor invasion of veins, we routinely increase lymph node dissection in No. 8p, 12p, and 14p groups to ensure the detection rate of positive lymph nodes. However, increasing lymph node dissection for patients' prognosis and complications is not the focus of this study, and we will conduct further research on this in the future.
Conclusion
To sum up, pancreatic cancer with major venous invasion is no longer a contraindication for laparoscopic surgery. To achieve the R0 resection, it is safe and feasible for a skilled surgical team with a lot of practice and training to perform laparoscopic venous resection, repair, and reconstruction. However, the surgical significance is not very relevant in this small sample size. For further validation, prospective large samples are needed.
Footnotes
Acknowledgment
The authors thank Dr. Yi-lei Mao and Dr. Cai-de Lu for their help in preparing and writing of the article.
Authors' Contributions
J.Z., B.C., and Haixiang Mao wrote the main article. X.Z., H.W., and D.Y. prepared Figures 1–![]() . H.L. contributed to the funding support. All authors reviewed the article.
. H.L. contributed to the funding support. All authors reviewed the article.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Ethics Committee of Ningbo Medical Center Lihuili Hospital (Approval No. KY2021SL152–01). All the patients provided written informed consent.
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was financially supported by the Ningbo Clinical Medicine Research Center Project (Grant No. 2019A21003) and Major Special Science and Technology Project of Ningbo City (Grant No. 2022Z128).