
Abstract
Purpose:
Transvesicoscopic ureteral reimplantation (TVUR) for vesicoureteral reflux (VUR) is a technically demanding operation. The technical difficulty is further increased by previous failed endoscopic injection, which causes intense fibrosis around the ureter. In this study, we compared primary TVUR with TVUR after previous failed endoscopic injection for VUR.
Materials and Methods:
The records of all children undergoing TVUR by a single surgeon over a 4-year period were analyzed. The children were divided into group 1 (primary TVUR, n = 50) and group 2 (TVUR after previous failed endoscopic treatment of Dextranomer/Hyaluronic Acid, n = 7). Demographic, clinical, radiologic, operative and follow-up data were compared between the two groups. The results were analyzed by statistical software; Mann–Whitney test and Fisher's exact test were used where appropriate, and P < .05 was considered significant.
Results:
Both the groups were comparable with respect to age and mean VUR grade. The mean VUR grade was significantly higher in group 1 and mean operative time per ureter was significantly more for group 2 than group 1. The postoperative hospital stay, success of TVUR, and complications were not significantly different between the groups.
Conclusions:
To our knowledge, this is the first report of its kind. TVUR after previous failed endoscopic injection could be done safely with good success, but with longer operative time than primary TVUR even in expert hands. Hence, previous failed endoscopic injection is not a contraindication to TVUR.
Introduction
Ureteral reimplantation (UR) is the gold standard for correction of primary vesicoureteral reflux (VUR). The past two decades have seen increasing interest in minimally invasive reimplantation, with laparoscopic extravesical (conventional and robotic) and transvesicoscopic ureteral reimplantation (TVUR) reporting success over 93%–95%.1,2 Endoscopic treatment (ET) with dextranomer/hyaluronic acid (DxHA) injection is also a first-line treatment for primary VUR with reasonable success and minimal morbidity. 3 Unlike UR, ET has lower success,3,4 and persistent VUR after ET is an indication for secondary UR. Although the inflammation and scarring associated with prior ET may complicate the UR and create difficulty during the ureteral dissection 5 and may prolong the operative time, 6 several authors have reported successful open UR after prior failed ET.5–10
A few authors also reported successful minimally invasive reimplantation after failed ET11–14 ; to our knowledge, there are few reports comparing primary TVUR with secondary TVUR after failed ET. In this article, we review our experience with secondary TVUR after failed ET and compare it with primary TVUR.
Materials and Methods
An Institutional Review Board-approved retrospective review was performed for patients undergoing TVUR over a 4-year period, from May 2017 to April 2021. Of these, patients with secondary VUR, obstructed megaureter, ureters requiring tapering, ureterocele, bladder diverticula, or associated pelviureteric junction obstruction were excluded; patients without a follow-up imaging to assess success of surgery were also excluded. The patients included in this review were divided into two groups: group 1 consisted of patients without prior endoscopic injection, while patients with prior endoscopic injection were considered group 2. All children of group 2 received one attempt of ET with DxHA.
Data were collected on demographics, reflux grade, history of endoscopic injection, age at TVUR, and stent use. Primary outcomes were success of TVUR and postoperative complications. Secondary outcomes were duration of surgery and length of hospital stay. The various parameters were compared between both the groups. Statistical analysis was done using software; Student's t-test and Fisher's exact test were applied where appropriate, and a P < 0.05 was considered significant.
Surgical technique
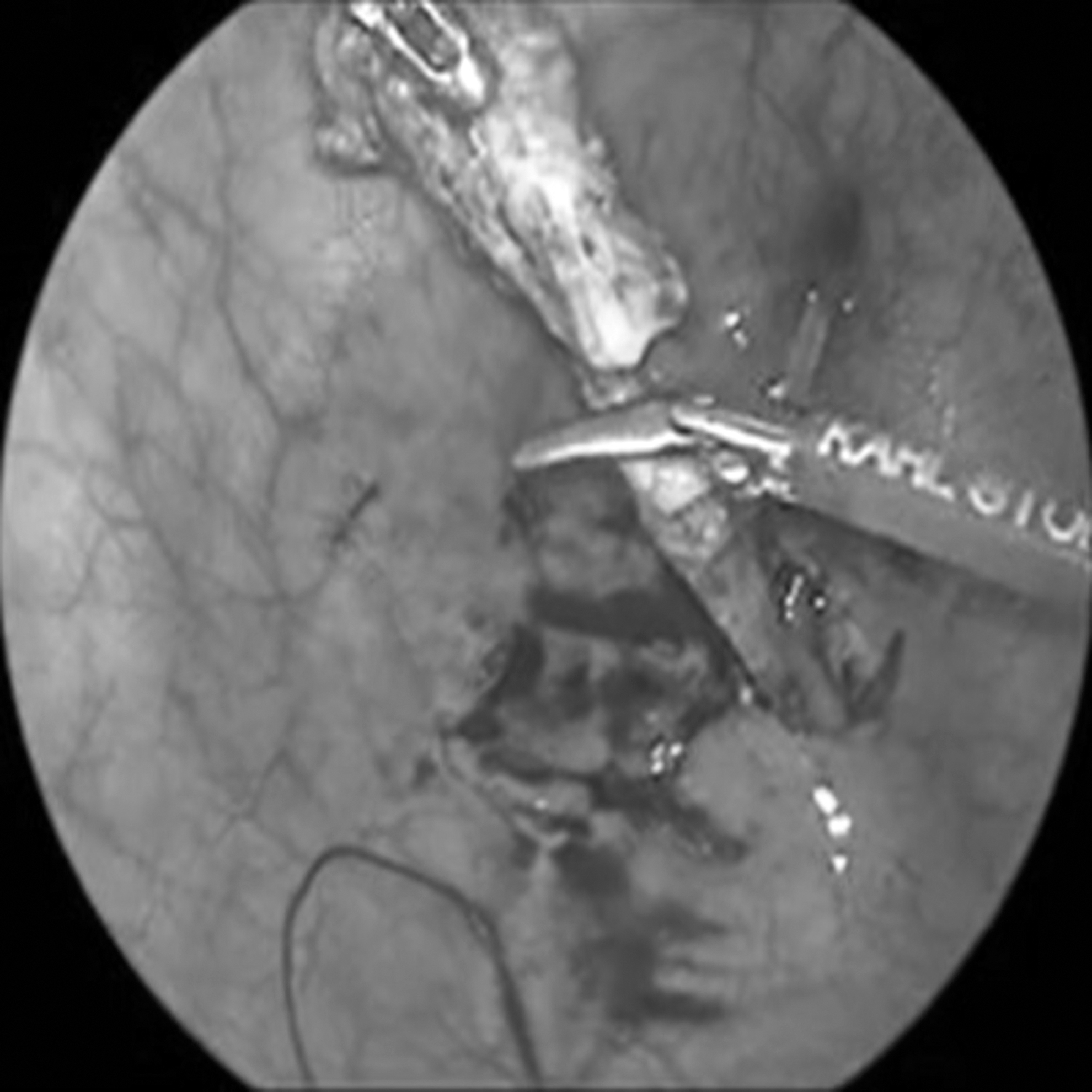
TVUR was performed with three ports; the technique was similar to the standard technique described earlier for vesicoscopic Cohen reimplantation,11,15 with very few minor variations. Similar techniques of port placement, reimplantation, and port closure were used in all children of both groups. In group 2, extra care was taken not to injure the wall of the ureter while mobilizing it; once the DxHA material was identified within the ureteral or bladder wall, the pseudocapsule encasing it was opened and the DxHA material was removed by applying pressure and suction (Fig. 1). The distal portion of the ureter was resected (Fig. 2) (unlike in group 1 where the distal ureter was typically retained in most cases) before reimplantation (Figs. 3 and 4).

Evacuation of subureteral DxHA. DxHA, dextranomer/hyaluronic acid.
Resection of terminal end of dissected ureter.

Creation of submucosal tunnel.

Vesicoscopic image after completion of neocystoureterostomy. White arrow denotes anastomosis; black single arrow—repair of mucosal defect at the site of previous ureteric orifice; black double arrow—resected distal ureter.
In both groups, double-J stents were used on a case-to-case basis; typically, most unilateral reimplantations were not stented, while in most bilateral cases, at least one ureter (usually the better functioning kidney) received internal stenting. The bladder was drained by a urethral Foley catheter of appropriate size for 36–48 hours after the surgery, after which it was removed, and the child was discharged home. When used, the double-J stent was removed after 3–4 weeks by cystoscopy.
The children were followed in the outpatient clinic at 1 month after surgery for stent removal and for an ultrasonogram. A voiding cystourethrogram (VCUG) (or direct radionuclide cystogram [DRCG] in girls) was performed 3–6 months after the operation to assess the success of surgery, which was defined as the complete resolution of VUR. Continuous antibiotic prophylaxis was continued until the cure of VUR was confirmed.
Results
During the study period, 98 patients underwent TVUR by a single surgeon (V.V.S.). Thirty-seven patients were excluded either for lack of postoperative follow-up imaging for VUR (n = 19) or because they had other associated congenital or acquired urologic conditions (n = 18), as specified in the Materials and Methods section. Thus, 61 patients (39 boys) with follow-up and postoperative imaging were included in the final analysis, 51 in group 1 (94 ureters) and 10 in group 2 (17 ureters) (Table 1).
Summary Table
ET, endoscopic treatment; F, female; M, male; TVUR, transvesicoscopic ureteral reimplantation; UTI, urinary tract infection; VUR, vesicoureteral reflux.
In all 61 patients, TVUR was successfully completed without any open conversions. The mean patient age was comparable in both groups. The mean reflux grade was higher in group 1 than group 2 (P < .001). The mean operative time per ureter (includes the time taken for ureteral dissection, mobilization, and reimplantation) was significantly longer (P < .001) in group 2 (53.1 ± 5.9 minutes) than group 1 (42.6 ± 6.9 minutes). The median postoperative hospital stay was 2 days in both groups. Double-J stent was used in 62 ureters of group 1 and 11 ureters of group 2. Urinary tract infection (UTI) was the main postoperative complication (group 1: 7/51, 13.7% versus group 2: 2/10, 20%; P = .600), which occurred in the first 2–4 weeks after surgery and was seen mostly in children receiving a double-J stent. There was no UTI after stent removal in any patient.
Postoperative VCUG/DRCG was obtained at a median 4 months (3–6 months) after TVUR. Follow-up imaging demonstrated complete VUR resolution in 90/94 (95.7%) ureters in group 1 and 16/17 (94.1%) ureters in group 2 (P = .644). In the 5 ureters (4 group 1, 1 group 2) with persistent VUR, the reflux was only low grade (grades 1–2), hence they were followed-up only by observation. At a median follow-up of 2 years (6 months to 4 years), all children are asymptomatic, without any evidence of UTI or worsening hydronephrosis on the ultrasound.
Discussion
To our knowledge, this is the first report of its kind, comparing the outcomes of TVUR for primary VUR in children with and without prior ET. Although open Cohen UR was found by several authors to be feasible, safe, and successful after prior ET,5–8 there is no consensus in the existing literature whether prior unsuccessful ET affected the performance and results of subsequent TVUR. A few authors11–13 reported successful TVUR after prior ET; Jayanthi 11 reported that of 182 consecutive TVUR operations, 15 patients had previous failed ET with DxHA. They observed that prior ET did not render the ureteral dissection more difficult; the pseudocapsule was opened to remove the implant, but no attempt was made to excise the pseudocapsule. No comparative operative time for this subgroup was mentioned in that report.
Marte et al. 12 reported that 8 of 19 ureters were subjected to ET before TVUR (2 prior ET injections in 4 ureters); TVUR was successful in all of them. Although the authors reported the operative time in each case, other confounding factors such as ureteral tailoring in some cases do not permit precise time comparison between the groups. Emir et al. 13 reported prior ET in 3 of 17 ureters that underwent TVUR, but did not comment on the operative difficulty or outcome in this group. In contrast, Lau et al. 16 reported TVUR in 31 patients, 4 of whom required open conversion. Three of 4 children that required conversion had prior DxHA injection, and the authors observed that the DxHA injected around the ureteric orifice previously resulted in severe adhesion and fibrosis, making distal ureter dissection difficult and thus required a conversion to open surgery. With these findings, the authors went on to suggest that TVUR may therefore be recommended as the first line treatment in patients with high-grade reflux owing to the increased operative difficulty and risks after previous endoscopic injection treatment. 16 In the present study, we found that TVUR was feasible, safe, and successful after prior failed ET, but it took significantly longer time to mobilize and reimplant the post-ET ureters.
In the present report, group 2 (post-ET) had significantly lower VUR grade than group 1. In our practice, ET is offered as the first-line treatment in grades 2–4 VUR requiring antireflux procedure, while children with grade 5 VUR are offered TVUR as the first line treatment. Thus, the mean VUR grade was significantly lower in group 2 than group 1. Other authors also reported similar policy of management of VUR according to the grade of reflux. Chung et al. 17 compared ET versus TVUR for first-line management of primary VUR. They stated that patients with lower grades VUR were offered DxHA and those with more severe VUR were offered reimplantation as the primary treatment of choice, which resulted in a higher mean VUR grade in the TVUR group.
Similarly, Friedlander et al. 7 examined the effect of ET on subsequent open Cohen UR and observed that the post-ET group had lower grades of VUR. In the present report also, group 2 had lower mean VUR grade, but despite lower VUR grade, the post-ET ureters took significantly longer operative time for TVUR.
Although most authors recommend ET for lower grades of VUR, the success of ET is still significantly inferior to UR, with about 20%–25% children with grades 2–4 VUR requiring repeat antireflux procedures after the first ET.3,4,17,18 The findings of the present report demonstrate that despite prior injection of DxHA, TVUR could be safely and successfully performed without increasing the postoperative bladder catheterization time or hospital stay. Thus, we continue to offer ET as the first-line treatment for grades 2–4 VUR, and reassure the parents that should the ET fail, the child could still undergo TVUR as a secondary procedure with good results and without an increased morbidity for the child.
There may be several reasons for the longer operative time in the post-ET group found in the present study. Primarily, the fibrosis and inflammatory pseudocapsule formation induced by the ET may render the ureteral dissection difficult. Unlike open UR where the assistant could help the surgeon with retraction and dissection, there are no additional hands to help the surgeon in TVUR, so any fibrosis and inflammation would render the ureteral dissection more time-consuming. Further, in these patients, it has been our policy to resect and remove the distal portion of the ureter, which was affected by the prior ET; hence, more extensive ureteral mobilization was required to gain adequate intravesical ureteral length for successful reimplantation. This additional length of ureteral mobilization might also have added to the increased operative time.
In this series, postoperative UTI occurred only in those patients who had double-J stent. Double-J stent is a known risk factor for UTI. The incidence of UTI in our series was comparable to other large series of children receiving double-J stent for urologic surgery. 19
The current study was limited by the retrospective nature of the design. In addition, there were smaller numbers of ureters in group 2 (with prior ET) compared to group 1. Further, although the groups were matched for age, the mean VUR grade was significantly different in both groups. In the present study, all children of group 2 had only a single prior injection of ET; it is possible that multiple injections may render later reimplantation more difficult and more time consuming, as has been observed by other authors 6 for open UR. Similarly, the technique of injection for ET may influence the degree of fibrosis and the subsequent difficulty during open UR; 5 as some of our cases were referred after prior ET done elsewhere, so the technique of DxHA injection was not clear in all cases.
To our knowledge, this is the first report of its kind. TVUR after previous failed endoscopic injection could be done safely with good success, but with longer operative time than primary TVUR even in expert hands. Hence, previous failed endoscopic injection is not a contraindication to TVUR.
Footnotes
Authors' Contributions
V.V.S.C.: Conceptualization (lead); writing—original draft (lead); formal analysis (lead); and writing—review and editing (equal), R.S.: review and editing (equal), K.K.J.: review and editing (equal).
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.