
Abstract
Introduction:
Esophageal atresia (EA) is a rare defect in the continuity of the esophagus, with the absent portion forming an upper and lower segment. Despite both thoracoscopic and conventional open repair (OR) techniques being well established worldwide, the literature remains unclear as to the comparison of surgical outcomes and efficacy of each procedure.
Aim:
To conduct a systematic review to determine which technique for EA repair, thoracoscopic or open, has the better outcome.
Methods:
A Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) compliant literature search returned 14 full text articles for analysis of demographic information and surgical outcomes.
Results:
Major comorbidities were more likely in the OR group (P < .05) with all other surgical outcomes comparable between the two groups.
Conclusion:
Overall, this systematic review highlights that the surgical outcomes of patients undergoing thoracoscopic repair for EA are comparable with those of the conventional OR.
Introduction
Esophageal atresia (EA) is a congenital abnormality, occurring in ∼1 in 4500 live births, 1 defined as a defect in the continuity of the esophagus, with the absent portion forming an upper and lower segment. 2 Till et al. describe EA as a spectrum, with variations in length of the atresia, as well as formations of tracheoesophageal fistula, each with their own surgical complexities. 2 In addition to this, EA is commonly associated with other birth defects and abnormalities, forming part of the VACTERL association. 3
The first successful repairs of EA were conducted and published by Haight in 1941, 4 where a conventional open repair (OR) of EA generally consists of posterolateral right extra pleural thoracotomy, providing good visualization of the defect for repair. 2 In recent years, the surgical techniques for the repair of EA and associated tracheoesophageal fistulas have evolved, with the introduction of thoracoscopic repair (TR) by Lobe et al. in 1999. 5 TR is performed under general anesthesia but utilizes ports and thoracoscopic instruments to complete the repair, with the right lung collapsed to provide access to the area of atresia. 6
Despite both thoracoscopic and conventional OR techniques being well established worldwide, the literature remains unclear as to the differences in surgical outcomes and efficacy of each procedure. With 24 years since the introduction of thoracoscopic EA repair, this systematic review aims to collate and analyze worldwide published literature to determine which technique for EA repair, thoracoscopic or open, has the better outcome.
Methods
A literature search was carried out through Medline and EMBASE by 2 independent reviewers, searching for terms including “open repair,” “thoracotomy,” “thoracoscopic repair,” and “oesophageal atresia”/“esophageal atresia,” to ensure studies with American English spelling would also be included. No publication date limit was applied. Exclusion criteria included literature not in English, not relevant to the study, conference abstracts, case reports, and systematic reviews. Abstracts and full texts were reviewed manually by both reviewers and inclusion of publications was agreed. Data extracted from each article included first author, publication year, study design, sample size, demographics of the study population, peri- and postoperative complications, and surgical outcomes.
This systematic review strictly followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to establish the articles to be used, with the process detailed in Figure 1.
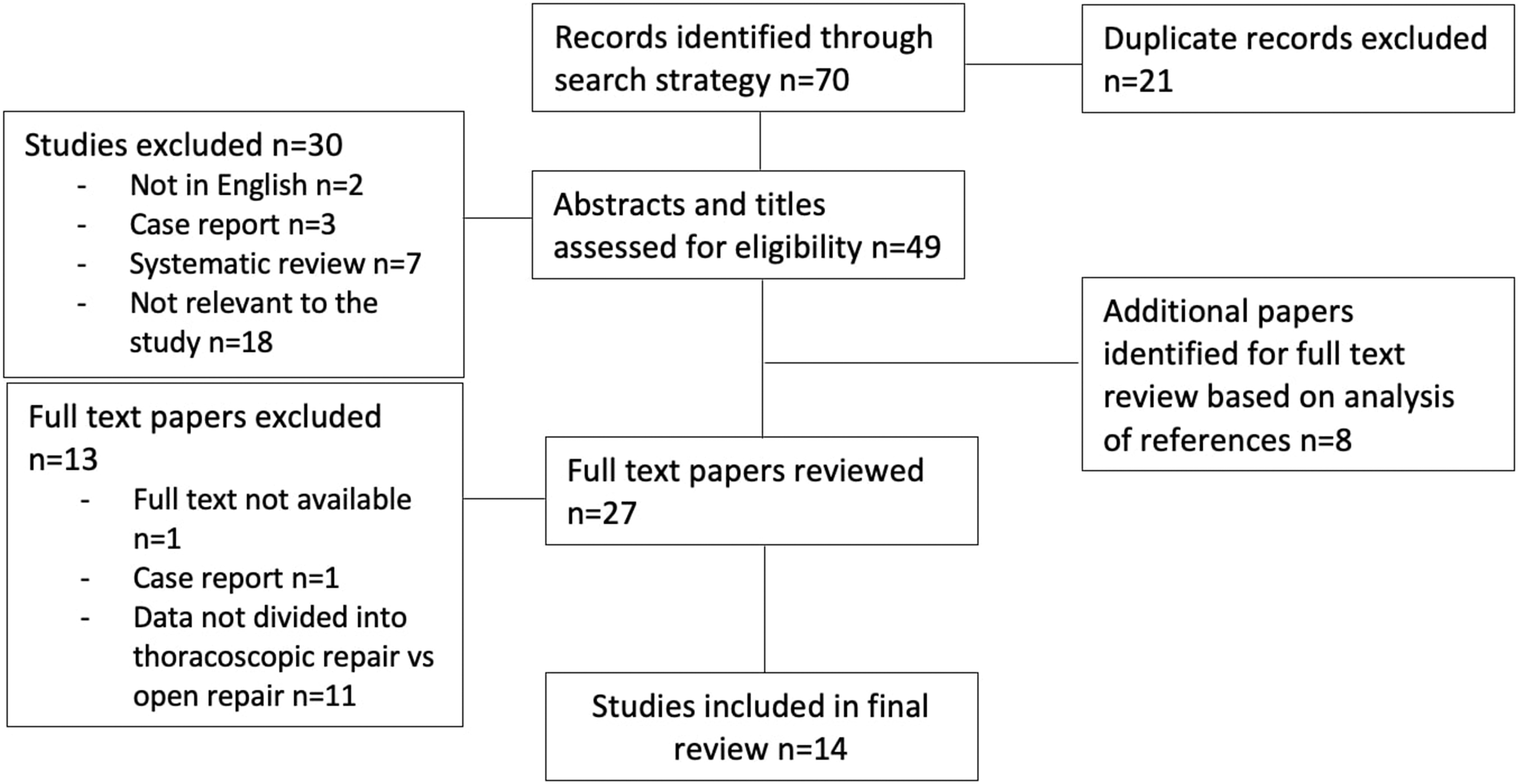
PRISMA flow diagram summarizing the selection and exclusion criteria of published literature on open repair and thoracoscopic repair of esophageal atresia. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
A total of 70 records were identified from the literature search, with 21 records excluded due to duplication. Forty-nine abstracts were assessed for suitability. Thirty studies were excluded due to relevance, case reports, systematic reviews, and not in English. In total, 27 articles were reviewed for full text, including 8 articles identified from references for full text analysis. After exclusion of 13 full texts, 14 articles remained for inclusion in the final systematic review.
Results
Original data were extracted from the 14 articles, Table 1 details the demographic data of the study populations. A total of 1432 patients underwent EA repairs, with 355 patients undergoing a TR and 1077 an OR. Mean age at procedure ranged from 1 to 7.3 days across both groups, with an overall total of 902 of 1381 patients recorded to have major comorbidities (Table 1).
Preoperative Demographics of Patients
Represents where the mean age is not used, but instead median age is used.
OR, open repair; TR, thoracoscopic repair.
Table 2 details perioperative and postoperative surgical outcomes. Outcomes included anastomotic leak rate, mortality, stricture rate, redo of operation, lower respiratory tract infection (LRTI)/pneumonia, mean length of hospital stay, mean length of operation, and duration of intubation (Table 2).
Perioperative and Postoperative Data
Data were statistically analyzed using Fisher's exact tests and t-tests to compare TR versus OR, with the P < .05 deemed to be statistically significant (Table 3).
Results of Statistical Analysis of Data
^Describes where % has not be used in this column but mean value has been used instead.
°Describes where % has not been used in this column, but instead the mean value has been used.
LRTI, lower respiratory tract infection.
Major comorbidities
Twelve studies included data of existing major comorbidities in patients, with 60.7% of patients in the TR group and 66.8% of patients in the OR group. Statistical analysis showed that major comorbidities were more likely in OR patients than in TR patients, statistically significant at P = .0471.
Mortality
Ten studies included data on mortality of patients undergoing esophageal repairs. Mortality was 2.6% in the TR group and 2.8% in the OR group (P = 1.0000).
Anastomotic leak
Eleven studies included information on the number of anastomotic leaks, with 14.3% and 12.4% in the TR and OR groups, respectively (P = .6883).
Stricture
Eleven studies reported data on strictures, with 27.7% of the TR group and 25.3% of the OR group (P = .6026).
Redo operation
Four studies published information on redo operations. This occurred in 6.8% of TR procedures and 7.8% of OR procedures (P = .6655).
LRTI/pneumonia
Six studies included information on the number of postoperative LRTI/pneumonia, with 11.4% and 14.7% in the TR and OR groups, respectively (P = .2173).
Mean operation time
The mean operation time across 10 studies was 170.87 and 148.41 minutes in the TR and OR groups, respectively (P = .2041).
Duration of intubation
Nine studies published data regarding the duration of intubation postoperatively. The mean duration of intubation was 5.07 days in the TR group and 8.05 days in the OR group (P = .2522).
Mean length of hospital stay
Nine studies published data regarding the duration of hospital stay, with the mean duration of 31.16 days in the TR group and 41.83 days in the OR group (P = .1611).
Discussion
This systematic review highlights the increasing use of TR of EA within standard practice worldwide, and that surgical outcomes are comparable with that of the conventional OR. By reviewing the published literature of TR versus OR of EA from the past 15 years, we can see on a larger scale the use and implications of these repairs that are now well established in the field, giving us the most up-to-date analysis of these procedures.
One key finding of this systematic review is that patients undergoing an OR had a significantly higher prevalence of major comorbidities compared with the thoracoscopic group, 66.8% versus 60.7%, P = .0471. Major comorbidities included VACTERL associations, cardiac abnormalities, and duodenal atresia, among many others. And 60.7% (n = 201) of patients undergoing a TR were reported to have major comorbidities, compared with 66.8% (n = 701) of patients undergoing OR. This difference was statistically significant at P = .0471.
As evidenced by this review and previously published literature, comorbidities alongside EA are very common 3 and, therefore, will tend to influence decisions regarding the best holistic management for patients, including the decision as to whether an EA repair should take place open or thoracoscopically. This statistically significant result could be explained by the relative contraindications for TR of EA, including specific cardiac abnormalities. 21 Those patients at higher risk and/or with an increased number of comorbidities may require an OR and, therefore, statistically show this consistently through the literature.
All other surgical outcomes between the two groups were comparable, which is generally in line with previous reviews of the literature.
Mortality was similar across both groups (2.6% in the TR group and 2.8% in the OR group, P = 1.0000), displaying that neither surgery has a worsened mortality risk than the other. Strictures occurred commonly in both sets of EA repair patients (OR: 27.7%, TR: 25.3%), often requiring balloon dilatation.
Other postoperative complications that were not statistically significant included anastomotic leak rate (TR: 14.3% and OR: 12.4%, P = .6883) and LRTI/pneumonia (TR: 11.4% and OR: 14.7% P = .2173). Requirement for redo surgery was small and comparable in both groups (TR: 6.8% and OR: 7.8%, P = .6655).
These results show that there are generally similar postoperative outcomes in both surgical procedures and the incidence in which a redo operation is need is almost equal for thoracoscopic and OR.
Despite a marginally shorter mean duration of intubation (TR: 5.07 days versus OR: 8.05 days) and hospital stay (TR: 31.16 days versus OR: 41.83 days) among the TR group, these figures were not statistically significant and generally ranged widely across the published literature, as given in Table 2.
Owing to the nature of this systematic review collating data from multiple sources, it is difficult to say whether some of the postoperative complications that occur are due to specific surgeon technique. For example, Ergun et al.'s 7 data show a 21% TR and 25% OR occurrence of anastomotic leaks among patients, compared with Koga et al.'s 12 data that recorded a 12% leak rate in the TR group and 2.5% leak rate in the OR group.
Published literature consistently refers to the learning curve that exists for all types of surgery. This curve is particularly steep with more advanced surgical skills such as thoracoscopy, especially within the pediatric population.22,23 Studies such as Lee et al. 24 reflect on the outcomes of TR cases over time and show a reduced number of strictures, leaks, and length of operation in their later cases in comparison with their earlier cases, indicating superior outcomes when this initial learning curve is endured.
Despite this steep learning curve for TR, there are benefits of avoiding an OR thoracotomy. TR allows for the avoidance of a thoracotomy incision, resulting in less pain for patients, and gives greater visualization for easier esophageal dissection. 25 TR has been found to show a reduction in musculoskeletal morbidity for patients, 26 with Lawal et al. 27 reporting a better cosmetic outcome and significantly reduced musculoskeletal anomalies with video-assisted thoracoscopy versus conventional thoracic surgery.
Conclusions
Overall, this systematic review has highlighted that both conventional OR and TR of EA are now standard practice and has concluded that there are similar surgical outcomes and complication rates in both procedures. This systematic review is in keeping with previous published literature, concluding that surgical outcomes of TR versus OR of EA are comparable. 28
As the TR technique is increasingly taught and used within clinical practice, further analysis of the surgical outcomes may be needed in the future to establish any impact of future developments. Previous literature has focused on the longer term impact on patients who have undergone EA repair, such as Acher et al. in 2015 29 This systematic review focused only on short-term surgical outcomes of TR and OR, but there is scope for future research to further assess the quality of life and psychological impact of the surgeries.
This study is limited by the small number of published studies comparing TR and OR of EA, however, we were able to analyze a relatively large number of patients to ensure we could produce confident statistical results and clearly show that OR and TR are comparable. In the future, a prospective randomized trial would provide better understanding of outcomes between the two operative approaches.
Footnotes
Authors' Contributions
E.F. contributed to conceptualization, methodology, investigation, data curation, formal analysis, writing—original draft, writing—review and editing, visualization, and project administration. S.E.F. was involved in conceptualization, methodology, investigation, writing—review and editing, supervision, and project administration.
Disclosure Statement
No competing financial interests exist.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.