
Abstract
Purpose:
Sigmoidectomy is performed in most cases for benign pathologies and mainly in cases of diverticulitis. Few studies in the literature report oncological results after sigmoidectomy for adenocarcinoma. The aim of this study was to report the long-term oncological outcomes after elective laparoscopic sigmoidectomy (LS) for adenocarcinoma.
Methods:
This study is a retrospective analysis of prospectively collected data. From January 2003 to February 2021, 173 patients underwent elective LS for adenocarcinoma. Twenty-four patients with a diagnosis of preoperative distant metastases were excluded (13.9%).
Results:
Seven postoperative complications were observed (7.1%). Of these, 2 (2%) anastomotic leakages were treated surgically by the Hartmann procedure (Clavien-Dindo grade III-b). The mean number of harvested lymph nodes with the specimen was 14.2 ± 7.1. At a median follow-up of 115 months (interquartile range 133.8), 2 (2%) and 9 patients (9.2%) had developed recurrence and metastases, respectively. During follow-up, 6 patients (6.1%) with metastases died due to disease progression and 6 other patients (6.1%) died due to causes other than cancer related. At the 5- and 10-year follow-ups, the overall survival rates were 90.5% ± 3.4% and 83.8% ± 4.5%, respectively, while the disease-free survival rates were 87.1% ± 4.1% and 83.5% ± 4.7%, respectively.
Conclusion:
LS is a safe and feasible technique both in terms of the number of harvested lymph nodes and oncological results. The possibility of sparing the colon without mobilizing the splenic flexure and dividing the left colic artery could reduce intra- and postoperative complications. Further studies with larger samples of patients are required to confirm these data.
Introduction
The sigmoid colon is the most frequent site of colon cancer representing approximately a quarter of all colon cancers.1,2 Currently, sigmoidectomy is the most common colic segmentary resection performed 1 and is adopted in most cases for benign disease, predominantly for diverticular disease. 3 Left hemicolectomy is considered the gold standard surgical treatment in cases of sigmoid cancer, while colic segmentary resection is indicated in cases of nonresectable distant metastases or cancerous adenoma.4,5 However, in the literature, some authors have reported their experience regarding sigmoidectomy for cancer.6–10
For both sigmoidectomy and left hemicolectomy, minimally invasive approaches showed better postoperative outcomes in comparison to open surgery in terms of postoperative pain, bowel function, complications, and hospital stay.5,11
Regarding the surgical techniques, sigmoidectomy and left hemicolectomy are similar; however, some details could differ.6–13 One aspect that can differ is the vascular step since in the case of left hemicolectomy, the inferior mesenteric artery (IMA) should be divided at its origin,12,13 while in the case of sigmoidectomy, it is possible to divide the IMA after the emergence of the left colic artery, thus sparing it, or to divide the sigmoid trunk at its origin or the superior, middle, and inferior sigmoid arteries separately.6–10 Another difference is colon mobilization.6,10,12,14 In fact, on the one hand, in the case of left hemicolectomy, the splenic flexure should always be mobilized to perform the anastomosis without tension; on the other hand, in the case of sigmoidectomy, splenic flexure mobilization could be avoided, particularly in the case of a long-left colon.6,10,12,14 For bowel restoration, the Knight-Griffen anastomosis technique is the most performed in both cases.9,10,12
For radical oncological surgery, in addition to free colon margins, with either technique, at least 12 lymph nodes should be harvested with the specimen for correct oncological staging.5,15
The aim of the present study is to report the long-term oncological outcomes after elective laparoscopic sigmoidectomy (LS) for adenocarcinoma.
Materials and Methods
This study is a retrospective analysis of prospectively collected data that was approved by our Institutional Review Board. Informed consent was obtained from all participants.
From January 2003 to February 2021, 173 patients underwent elective LS for adenocarcinoma in our centers (General Surgery and Organ Transplantation Unit, San Camillo Hospital, Rome, and UOC of General and Minimally Invasive Surgery, Hospital “San Paolo,” Civitavecchia, Rome, Italy). Twenty-four patients with a diagnosis of preoperative distant metastases were excluded (13.9%). Follow-up data of the remaining 149 patients were obtained from the Unit of Oncology for the first 5 years after surgery. After that period, for the purpose of the present study, the patients were contacted by phone.
Study design
Sex, age, body mass index, comorbidities, previous abdominal surgery, American Society of Anesthesiologists grade, associated procedures, intraoperative complications, conversion to open surgery, operative time, postoperative complications (graded according to the Clavien-Dindo classification 16 ), number of lymph nodes harvested with the specimen, staging (according to the American Joint Committee on Cancer classification 15 ), postoperative hospital stay, readmission, 30-day mortality, follow-up duration, data on recurrences and metastases were collected in the Microsoft Excel program (Microsoft Corporation, Redmond, WA).
Surgical technique
The surgeon stood at the patient's right side. Four trocars were used. Surgery started with the identification of the sigmoid trunk or the superior, middle, and inferior sigmoid arteries, which were divided with clips. The sigmoid colon was mobilized with the splenic flexure only if needed. Colon dissection proceeded reaching the rectosigmoid junction that was divided using a linear stapler (Endo GIA™ Ultra Universal Stapler; Covidien, Minneapolis, MN, USA). Using a left hypochondrium incision, the colon stump was extracted and divided proximally to the lesion, and the anvil of the circular stapler was inserted. Through laparoscopy, an end-to-end anastomosis with a circular stapler (DST series™ EEA™ Stapler; Covidien, Minneapolis, Minnesota, USA) was performed according to the Knight-Griffen technique.
Statistical analysis
Continuous variables are expressed as the mean ± standard deviation, while categorical variables are expressed as frequencies and percentages.
Overall survival (OS) was calculated from the date of surgery to the date of death, and disease-free survival (DFS) was calculated from the date of surgery to the date that evidence of recurrence or metastases was obtained. Survival analysis was performed by the Kaplan–Meier method. Subgroup analysis was performed after stratifying patients according to tumor stage, and comparisons were performed using the log-rank test.
A P-value lower than .05 was considered statistically significant. Statistical analyses were carried out with SPSS software 22.0 (SPSS, Inc., Chicago, IL, USA).
Results
Fifty-one out of 149 patients (34.2%) were lost to follow-up, leaving 98 patients with sufficient data for analysis and forming our study population (Fig. 1). Table 1 reports the patients' characteristics.

Patient enrolment.
Patient Characteristics
SD, standard deviation.
Five associated procedures were performed (4 umbilical primary hernia repairs and 1 resection of the fundus of the uterus, 5.1%). Conversion to open surgery was required in 3 patients due to adhesions from previous surgeries (3%). The mean operative time was 139.9 ± 35.1 minutes (range 60–300 minutes) (Table 2).
Perioperative Details
AJCC, American Joint Committee on Cancer; 15 SD, standard deviation.
Overall, seven postoperative complications were observed (7.1%). Two patients (2%) with anastomotic leakage were treated surgically by the Hartmann procedure (Clavien-Dindo grade III-b) (Table 2).
The mean number of lymph nodes harvested with the specimen was 14.2 ± 7.1 (range 5–47). The mean postoperative hospital stay was 8.8 ± 4.5 days (range 5–42). The readmission and 30-day mortality rates were nil (Table 2).
At a median follow-up of 115 months (interquartile range 133.8), 2 (2%) and 9 patients (9.2%) had developed recurrence and metastases, respectively (Table 3). Twelve patients (12.2%) died during follow-up. Of these, 6 patients (6.1%) with metastases died due to disease progression, and 6 other patients died due to causes other than cancer.
Recurrences and Metastases That Occurred During the Follow-Up Period
At the 5- and 10-year follow-ups, the OS rates were 90.5% ± 3.4% and 83.8% ± 4.5% (medians were not reached), while the DFS rates were 87.1% ± 4.1% and 83.5% ± 4.7% (medians were not reached), respectively. The probabilities of OS and DFS according to different tumor stages are reported in Figure 2.
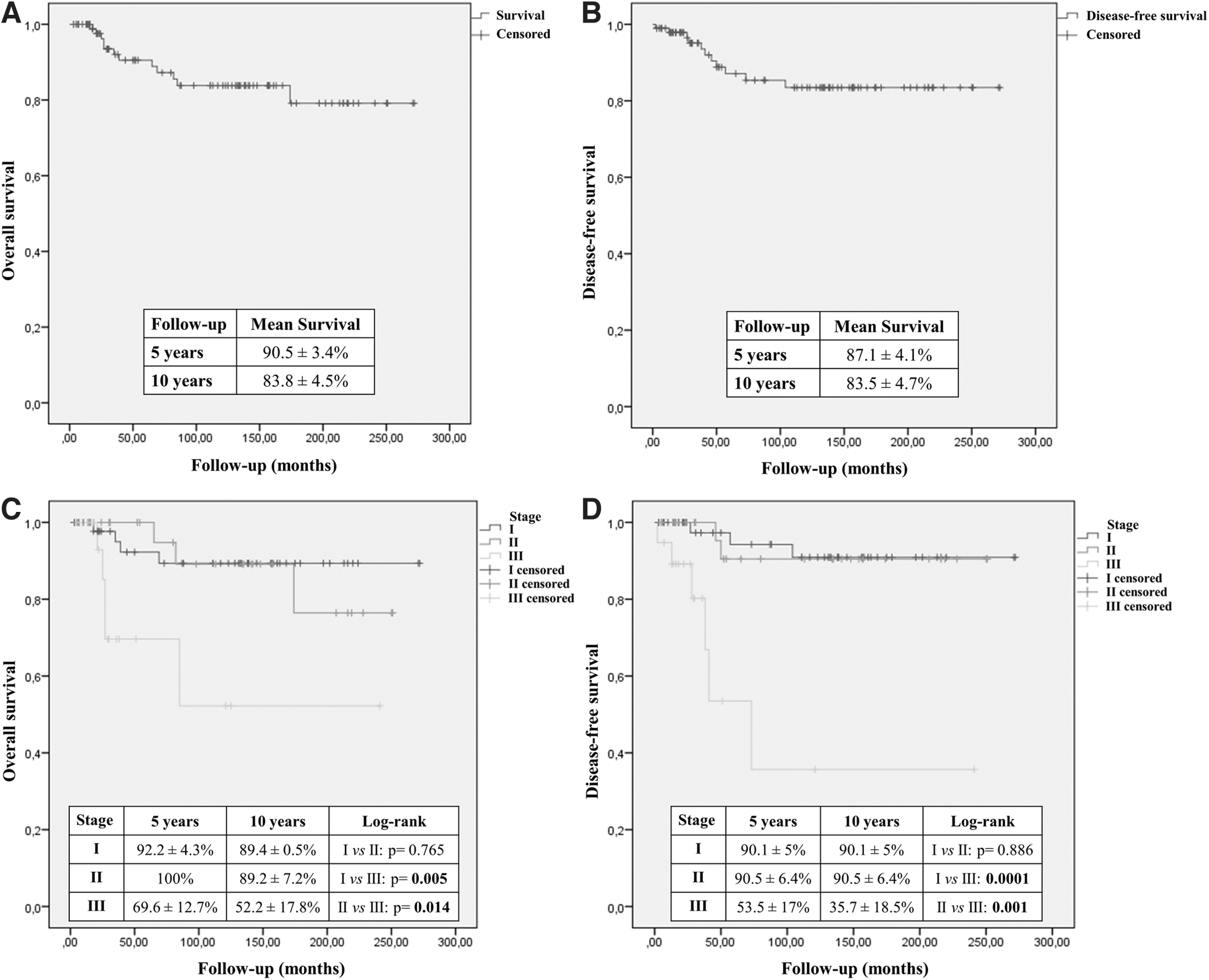
Kaplan–Meier curves of overall survival
Discussion
The present study was conducted with the aim of reporting the long-term oncological results of LS for sigmoid adenocarcinoma. To obtain homogeneous data, patients with metastases at surgery were excluded from the study. The OS and DFS rates at the 5- and 10-year follow-ups were encouraging in patients with stage I and II, and even those with stage III, although a reduction in both OS and DFS was observed. The mean number of harvested lymph nodes with the specimen was sufficient to obtain an accurate disease staging.5,15
LS is a feasible and safe surgical technique; however, in the case of adenocarcinoma, the main criticism against this technique is related to vascular ligation, which can influence the number of harvested lymph nodes and, as a consequence, the oncological result.4,8,15,17,18 Three important aspects regarding vascular ligation should be considered.8,19 The first is the oncological aspect; in fact, lymph node invasion is the most important negative prognostic factor in colon cancer, and the level of vascular ligation could influence the oncological radicality and the staging accuracy.8,19 Thus, vascular ligation is mandatory for radical surgery, but it is necessary to ensure optimal vascularization of the remaining colon to avoid complications such as anastomotic leakage.8,20,21 Finally, the nerves of the autonomic nervous system, located near the vascular structures, must be preserved to avoid anorectal and urogenital dysfunction.8,22
Two levels of IMA ligation are typically described in the literature.6,8,23 “High” ligation (HL) is defined as when the artery is divided at its origin at the aorta level, while “low” ligation (LL) is defined as when the artery is divided distal to the origin of the left colic artery.6,8,23 However, two other types of ligations have been proposed: in the first one, described by Valdoni et al., the IMA is skeletonized and along its axis and left colic artery, and all the sigmoid arteries encountered are divided6,24; in the second one, described by Nano et al., named “flush” ligation, the ligation is performed flush with the aorta (<0.5 cm).8,25 In the literature, there is no consensus regarding the best ligature to perform in terms of oncological results, with the results of HL and LL being comparable in terms of OS and DFS.26–28
In the present study, division of the sigmoid trunk or division of the sigmoid arteries was performed, avoiding both HL and LL IMA ligation. However, the number of harvested lymph nodes and the oncological results obtained do not deviate from the literature.27,29–31 Kim et al. compared the oncological results of HL versus LL of the IMA plus lymph node removal between the root of the IMA and the IMA ligation in patients with sigmoid or rectal cancer. 27 The mean number of harvested lymph nodes was similar between the two groups (20.9 ± 13.2 and 20.2 ± 9.2 for HL and LL, respectively), with OS durations of 63.7 ± 1.6 and 57.7 ± 2.1 months, and DFS durations of 69.1 ± 2.6 and 45.9 ± 2.4 months for HL and LL, respectively. 27 Yin et al. performed HL in cases of sigmoid or rectal cancer, and over the reported median follow-up duration of 49.1 months, the estimated OS and DFS rates were 86.1% and 79.6%, respectively. 29 Yamamoto et al. compared results obtained with HL and LL in cases of surgery for stage II and III sigmoid and rectosigmoid cancer. 30 The median number of harvested lymph nodes was not significantly different when dividing patients based on HL and LL or based on stage II and III. 30
In patients with stage II disease, at the 5-year follow-up, the OS rate was 94.8% in the HL group (43 patients) versus 91.8% in the LL group (70 patients), while the DFS rate was 93% in the HL group versus 87.6% in the LL group. 30 In patients with stage III disease, at the 5-year follow-up, the OS rate was 88.3% in the HL group (48 patients) versus 86.9% in the LL group (50 patients), and the DFS rate was 71.4% in the HL group versus 69.8% in the LL group. 30
Kwak et al. proposed radical lymphadenectomy during left colon resection (mean lymph nodes harvested 30, range 12–122), reporting at the 5-year follow-up that the OS rates for stage I, II, and III were 97.8%, 97.9%, and 62.5%, respectively, with DFS rates of 79.3%, 89.6%, and 93.9%, respectively, in a sample of 623 patients. 31 Lim et al. reported their experience with 207 patients, with a mean number of harvested lymph nodes of 16 ± 11.1. 32 At the 5-year follow-up, the OS rates for stage I, II, and III were 98.9%, 87.9%, and 78.6%, respectively, and the DFS rates were 100%, 84.6%, and 81.9%, respectively. 32
The level of vascular ligation, as mentioned above, could also influence postoperative complications, particularly the anastomotic leakage rate.8,20,21,23,33,34 It is reported that in ∼5% of cases, the vascular anastomosis between the ascending branch of the left colic artery and the ascending branch of the middle colic artery (first branch of the superior mesenteric artery) (Riolano's arcade) and the vascular anastomosis between the superior and inferior mesenteric arteries (including anastomosis between ileocolic artery branches and branches from right, middle, and left arteries) (Drummond's arcade), both forming the marginal arteries of the colon, are missing.8,20,21,23,33,34
This could lead, in cases of LL of IMA, to ischemia of the proximal left colon stump, increasing the risk of anastomotic leakage, even if this condition is related to a low percentage of vascular variations.8,20,21,23,33,34 In the present series, the anastomotic leakage rate was 2%, which is a good result compared to that in the literature, in which the anastomotic leakage rate reported ranges between 2% and 36%.8,12,20,21,23,26,27,33–35 Moreover, sigmoidectomy could help avoid mobilization of the splenic flexure, further reducing the risk of intra- or postoperative complications.
To the best of our knowledge, this is the first study reporting the long-term (up to 10 years) oncological results after LS for adenocarcinoma. The main limitations of the present study are its retrospective nature, the lack of a comparison group, and the small sample of patients.
In conclusion, LS for adenocarcinoma proved to be a safe and feasible technique both in terms of the number of harvested lymph nodes and oncological results at 5- and 10-year follow-ups, and was comparable to more radical techniques, such as left hemicolectomy with LL of the IMA. The possibility of sparing the colon without mobilizing the splenic flexure and dividing the left colic artery could reduce the intra- and postoperative complication rates. Further studies with larger samples of patients are required to confirm these data.
Footnotes
Authors' Contributions
A.B.: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing—original draft, Writing—review and editing. F.S.: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Supervision, Validation, Visualization, Writing—original draft, Writing—review and editing. A.G.: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Supervision, Validation, Visualization, Writing—original draft, Writing—review and editing. R.S.: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Supervision, Validation, Visualization, Writing—original draft, Writing—review and editing. D.C.: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Supervision, Validation, Visualization, Writing—original draft, Writing—review and editing. G.M.E.: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Supervision, Validation, Visualization, Writing—original draft, Writing—review and editing. P.L.: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Supervision, Validation, Visualization, Writing—original draft, Writing—review and editing.
Disclaimer
The authors alone are responsible for the content and writing of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.