
Abstract
Background:
The difficulty scoring system based on the extent of resection (DSS-ER) is a common tool for assessing the difficulty and risk of laparoscopic liver resection (LLR), but DSS-ER fails to comprehensively and accurately assess low level for beginners.
Methods:
The 93 cases of LLRs for primary liver cancer in the general surgery department of the Second Affiliated Hospital of Guangxi Medical University from 2017 to 2021 were retrospectively analyzed. The low level of DSS-ER difficulty scoring system was reclassified into three grades. The intraoperative and postoperative complications were compared among different groups.
Results:
There were significant differences in the operative time, blood loss, intraoperative allogeneic blood transfusion, conversion to laparotomy, and allogeneic blood transfusion among the different groups. Meanwhile, the postoperative complications were mainly pleural effusion and pneumonia, and the incidence of grade III was higher compared with other two grades. No significant difference existed in the postoperative biliary leakage and liver failure among three grades.
Conclusions:
This reclassified low level of DSS-ER difficulty scoring system has certain clinical value for LLR beginners to complete the corresponding learning curve.
Introduction
Since the first case of laparoscopic liver resection (LLR) reported in 1991, the feasibility, safety, and efficiency of LLR have been demonstrated. 1 Recently, the number of LLRs performed worldwide has increased exponentially. It has been a standardized operation widely used in the field of hepatobiliary surgery.2–5 Compared with the open liver resection, LLR has less blood loss, shorter hospital stay, and no significant difference in postoperative morbidity and mortality.6,7 However, LLR has high difficulty and risk for beginner.8,9
The European Guidelines Meeting for Laparoscopic Liver Surgery in 2017 highlighted the necessity of a stepwise progression through the learning curve to minimize morbidity. 10 Therefore, preoperative assessment of the difficulty of LLR is important for surgeons. Among various preoperative difficulty scoring systems for LLR, the difficulty scoring system based on the extent of resection (DSS-ER) proposed by Kawaguchi et al in 2017 has been widely applied with the advantages of objective, simple, and easy operation. 11 This scoring system classifies 11 common LLR procedures into three levels. Beginners can complete the corresponding operation according to different difficult levels. However, this scoring system ignores several important factors, including tumor size, location, and proximity to important blood vessels, which affect the accuracy of predicting surgical difficulty for LLR.
This study reclassified the low level of DSS-ER difficulty score system to establish three grades, and discussed the effectiveness of this novel classification on predicting operative difficulty and safety for LLR beginners.
Materials and Methods
Research design
From August 2017 to November 2021, 93 patients underwent LLR at the Department of General Surgery in the Second Affiliated Hospital of Guangxi Medical University in Nanning, China.
This inclusion criteria were as follows: (1) LLR for hepatocellular carcinoma (HCC); (2) Patients were in good performance status with an Eastern Cooperative Oncology Group performance score <2 points; (3) All patients underwent volumetric computed tomography or magnetic resonance imaging before operation; (4) The liver function was in Child-Pugh grade A or B. 12
Exclusion criteria: (1) Contraindications of open hepatectomy; (2) Failure to establish CO2 pneumoperitoneum during operation or failure to place laparoscopic surgical instruments; (3) Patients requiring intraoperative hepatic vascular and biliary reconstruction.
The perioperative indicators reflected the difficulty of operation were as follows: operative time, blood loss, allogeneic blood transfusion, postoperative hospital stay (POS), and postoperative complications, including liver function failure, postoperative pleural effusion, pneumonia, and bile leakage.
Definitions
Operative time was defined as the time first skin incision was made to final skin closure. The blood loss was regarded as the amount of blood loss during the procedure, which was monitored by the anesthesiologists and recorded at the end of surgery. Liver segments II, III, IVb, V, and VI according to Couinaud's classification were defined as anterolateral (AL) segment, and segments I, IVa, VII, and VIII were defined as the posterosuperior (PS) segments. 13 Multiple tumors were referred to 2–3 tumors. Previous surgical history contained upper abdominal surgery, microwave ablation for liver tumor, and alcohol injection for liver tumor.
New classification of low level
The low-level procedures of DSS-ER difficulty score system contained partial hepatectomy of AL segment, partial hepatectomy of posterolateral segment, and left lateral lobectomy. 11 It was divided into three levels of difficulty by the new classification. Grade I (low level) contained partial hepatectomy of AL segment with tumor diameter <5 cm. Grade II (intermediate level) was shown as following: (1) Partial hepatectomy of the AL segment with tumor diameter of 5–10 cm; (2) Partial hepatectomy of PS segment with tumor diameter <5 cm; (3) Left lateral lobectomy. Grade III (high level) included: (1) Partial hepatectomy for AL segment with tumor diameter >10 cm; (2) Partial hepatectomy of PS segment with tumor diameter >5 cm. The flowchart was demonstrated as Figure 1.
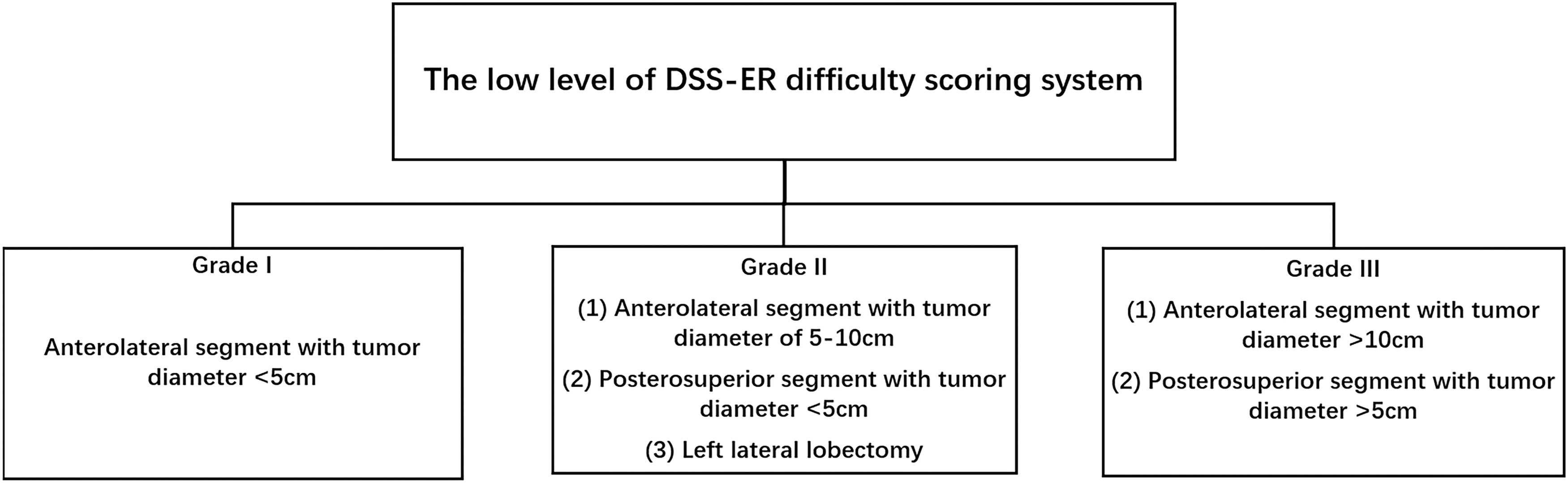
Reclassifying low level of DSS-ER difficulty scoring system. Grade I represents low level of difficulty; Grade II represents intermediate level of difficulty; Grade III represents high level of difficulty. DSS-ER, difficulty scoring system based on the extent of resection.
Statistical analyses
Statistical analyses were performed by SPSS 23.0 software package (SPSS Statistics, Inc., Chicago, IL). Continuous variable data were presented as mean ± standard deviation. Data conforming to the abnormal distribution were represented by median [mean (interquartile range)]. Least-Significant Difference test was used to compare between two groups. Kruskal–Wallis rank-sum test was used to compare in multiple groups. Chi-Squared test or Fisher's exact test was used to determine the association between categorical variables. For all analyses, P < .05 was considered significant.
Results
The characteristics of patients are summarized in Table 1. Of the 93 patients diagnosed with primary liver cancer, 78.5% were male. The patients had an average age of 53.51 ± 11.58 years, and average body mass index (BMI) was 23.02 ± 3.02 kg/m2. The majority etiology of HCC was hepatitis B virus (HBV), accounting for 80.6% of the study group. Sixty-seven (72.0%) patients complicated with liver cirrhosis. Fifty-three (57.0%) patients were in stage Ia according to China liver cancer staging, and stage Ib was 38 (40.9%) of the cohort. 14 Laparoscopic partial hepatectomy was performed in 77 (82.8%) patients.
Basic Characteristics of the Enrolled Patients
AL; Liver segments II, III, IVb, V, and VI; PS Liver segments I, IVa, VII, and VIII. Data are presented as the mean with standard deviation (x¯ ± SD), or counts with percentages n (x%).
AFP, alpha fetoprotein; AL, anterolateral; ALB, albumin; ALP, alkaline phosphatase; ALT, alanine aminotransferase; BMI, body mass index; CNLC, China liver cancer staging; HBV, hepatitis B virus; PAB, prealbumin; PS, posterosuperior; PT, prothrombin time; SD, standard deviation; TBIL, total bilirubin.
Patients were classified into three groups according to new classification as follows: 28 cases in grade I, 42 cases in grade II, and 23 cases in grade III. The clinical characteristics of patients and statistical difference in the three grades are shown in Table 2. There was significant difference in the preoperative features, including tumor location (P = .000), tumor diameter (P = .000), Alpha fetoprotein level (P = .043), and operative maneuvers (P = .000). However, no significant difference existed in patients' characteristics among three grades, including age, sex, BMI, previous surgery, history of smoking, history of alcohol consumption, diabetes mellitus, hypertension disease, history of HBV, liver cirrhosis, Child-Pugh stage, platelet, alanine aminotransferase, total bilirubin, albumin, tumor numbers, and whether adjacent to vital vessel or not.
Basic Characteristics of Patients Between Groups
Data are presented as the counts with percentages n (x%).
Indicates using Fisher exact test.
Indicates P < .05.
AFP, alpha fetoprotein; AL, anterolateral; ALB, albumin; ALT, alanine aminotransferase; BMI, body mass index; HBV, hepatitis B virus; PS, posterosuperior; TBIL, total bilirubin.
In addition, significant difference existed in the perioperative conditions among three grades, including operative time, blood loss, intraoperative allogeneic blood transfusion, and conversion to laparotomy, as well as whether allogeneic blood transfusion or not (P < .05). Furthermore, the amount of blood loss gradually increased by the operation difficulty after pairwise comparison (P < .05). The significant longer operative time, higher conversion to laparotomy, and longer POS were observed in grade III than the other grades (P < .05). The significant difference in allogeneic blood transfusion was found between grades I and III (P < .05). These results are shown in Table 3.
Comparison of Surgical Conditions with New Difficulty Score
Indicates compared with Grade I, P < .05.
Indicates compared with Grade II, P < .05.
Indicates compared with Grade III, P < .05.
§Indicates using Fisher exact test.
POS, postoperative hospital stay.
The postoperative complications mainly were pleural effusion and pneumonia in three groups, and higher incidence in grade III compared with other two grades (P < .05). Meanwhile, no significant difference existed in postoperative biliary leakage and liver function failure in three groups (P > .05).
Discussion
Since LLR is one of the most complicated operations and characterized by high technical requirements, both preoperative evaluation and strict technical training are needed.15,16 To apply difficulty scoring system before LLR can help surgeons choose the LLR procedure with appropriate difficult level, and protect fundamental interests of patients,17,18 as well as guild beginners to overcome the LLR learning curve shortly.19–21
The main factors affecting the difficulty of LLR contain tumor size, tumor location, and whether adjacent to important blood vessels or not. At present, LLR has been widely used in the treatment for tumors in AL segments. Although the safety and efficacy of LLR for tumors in PS segments have been confirmed, it is still limitedly performed by advanced skilled surgeons. 22 It is necessary to provide an effective and accurate way to delimit LLR difficulty classification for beginners.
In this study, we established a novel classification for low level of DSS-ER difficulty scoring system for LLR. We ascertained the effectiveness of the classification through analyzing perioperative characteristics of 93 patients with LLR. We found that procedures in grade I had less operative time, less intraoperative bleeding, lower intraoperative allogeneic blood transfusion rate, and lower conversion to laparotomy. Moreover, the operative time, blood loss, intraoperative allogeneic blood transfusion rate, and conversion to laparotomy would gradually increase by difficult levels. The postoperative pneumonia and pleural effusion significantly increased in grade III.
In addition, no significant differences were observed in operative time, intraoperative allogeneic blood transfusion rate, and conversion to laparotomy in grade II compared with grade I. However, we found that laparoscopic left lateral lobectomy accounted for 38.1% in grade II group. The left lateral lobe was easily exposed and relatively simply performed in the laparoscopic operation, which is the earliest and widely used procedure. 23 Furthermore, blood loss, operative time, and intraoperative allogeneic blood transfusion rate in laparoscopic left lateral lobectomy is lower than traditional open surgery.24,25 Meanwhile, autologous blood transfusion was widely used in three groups, which reduced allogeneic blood transfusion rate.
This study showed that 6 cases (24.1%) were converted to open surgery during operation in grade I, of which 4 converted cases were due to the deep location of tumor in the early period of beginner. Because laparoscopy provides a two-dimensional view plane, it is relatively difficult for beginners to find tumors with deep location in the liver. 26 With the assistance of laparoscopic ultrasound, surgeons can easily understand the location and size of tumors, the relationship between the tumor with vessels and bile ducts, as well as intrahepatic metastasis in the operation. 27
This study showed that the incidence of postoperative respiratory complications, such as pneumonia and pleural effusion in grade III group, was higher than those in the other groups. Uchiyama et al found that obstruction of lymphatic reflux from liver to thorax caused by the destruction of perihepatic ligament was one important factor for pleural effusion formation. 28 In the grade III, PS segment accounted for 82.6% of partial hepatectomies. Since the right perihepatic area was significantly larger compared with the left liver, the incidence of right pleural effusion was higher compared with the left side after hepatectomy. 29 Meanwhile, higher conversion to laparotomy in the grade III resulted in increased pulmonary infection due to insufficient sputum drainage caused by incision pain.
In addition, this study showed that postoperative bile leakage and liver function failure were not correlated to the different grades. However, there were 2 cases of postoperative liver function failure in the grade III group, which was considered to be caused by the greater extent of liver resection and difficultly of controlling bleeding from the injured adjacent blood vessels in the operation.
In summary, the low level of the DSS-ER difficulty scoring system was reclassified to three grades for LLR beginners in this study. We confirmed the effectiveness of this novel classification. The limitation of this study was that results were dependent on a single-center retrospective analysis with a small sample size and the possibility of selection bias. Meanwhile, this study was not verified externally. Therefore, further large-scale multicenter studies are needed to confirm it.
Conclusion
The low level of DSS-ER difficulty scoring system is delimited. This novel classification accurately predicts intraoperative conditions and postoperative complications, which will be beneficial for beginners to overcome LLR learning curve shortly.
Footnotes
Acknowledgments
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Authors' Contributions
T.L. and Y.Y. designed the project. T.L., Y.O., T.H., Z.X., M.Y., and J.L. collected the data. T.L., Y.O., and Y.Y. wrote the article. Y.H. and X.C. contributed on project consultations and helped with the interpretation of the results. All authors contributed to the article and approved the submitted version.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors without undue reservation.
Ethics Statement
This study was approved by the Ethics Committee of the Second Affiliated Hospital of Guangxi Medical University. The patients provided their written informed consent to participate in this study.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Disclosure Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
This work was supported by the Guangxi Natural Science Foundation (2020GXNSFAA297008, Y.Y.) and the Scientific Research Project of Guangxi Health Commission (S2021114, Z20170075, Y.Y.).