
Abstract
Background:
Described by Heald in 1982, total mesorectal excision (TME) is now routinely performed as the standard procedure for mid-low rectal cancer, with remarkable decrease in local recurrence and improved oncology outcome. However, the integrity of the resected mesentery and damage to autonomic nerves still remain challenging for general surgeons, especially in the cohort of neoadjuvant therapy patients. The concept of rectal modular resection (RMR), based on an integral understanding of the regional anatomy, was proposed as a surgical skill for dissociation of the rectum with shorter surgical duration, function preservation, and improved oncology outcome.
Methods:
This was a retrospective trial. Patients with resectable rectal lesions, ranging between 3 and 7 cm from the anal verge, were enrolled and grouped by TME surgery based on RMR or classical procedure resection (CPR). We estimated perioperative outcomes, including surgery complications such as anastomotic leak, urine retention, and others. Pathological properties, including distal clearance, harvested lymph nodes, tumor differentiation, and specimen grading, were also taken into account. Patients were followed postoperatively and functional evaluation was recorded at the 3-month and 1-year postoperation visits.
Results:
From January 2019 to December 2021, a total of 92 patients were enrolled in this study. TME surgery complying with the RMR methodology was performed with a back-to-bilateral-to-front modular proceeding. Duration of operation was significantly shortened in the RMR group, without increase in blood loss or failure rate of anus preservation. The quality of the specimen, graded according to integrity of the mesorectum, stands out in the RMR group. Functional evaluation revealed no statistical difference between RMR and CPR groups regarding sexual ability impairment and defecation disorder since follow-up is still ongoing.
Conclusions:
RMR-based TME was efficient with compressed operation duration compared with CPR and its safety was well validated with regard to the occurrence of complications and function loss.
Introduction
Colorectal cancer is the third most common cancer worldwide. 1 There have been major improvements in survival and oncological outcomes due to total mesorectal excision (TME) and advances in preoperative therapy. TME surgery after neoadjuvant chemoradiotherapy has been recommended as standard practice for patients with locally advanced rectal cancer (LARC). 2 In recent years, greater focus has been placed on postoperative functional complications such as urinary, sexual, and bowel dysfunction.3,4 Surgery is the foundation of multimodal treatment of rectal cancer, thus great efforts were made after modification of surgical approaches to ensure negative circumferential resection margin (CRM) as well as function preservation.
First described by Heald in 1982, TME is the standard technique for removing perirectal tissue when performing radical rectal cancer resection, no matter if it is low anterior resection (LAR) or abdominoperineal resection (APR). 5 While different strategies emphasize the importance of fascial anatomy and surgery planes, the order of performing TME has been relatively neglected. Since there is no step-by-step guide for performing TME surgery, 6 when it comes to irradiated tumors with tissue edema and adhesion, complete removal seems to be more challenging.
In 2003, a new distal pancreatectomy approach called radical advanced modular pancreatectomy and splenectomy (RAMPS) was developed. 7 It guided dissection of pancreas using the right-to-left route. The delicate maneuver of the sequential procedure based on insight into the local anatomy proved to be safe and efficient. Inspired by RAMPS, we refined the procedure of TME as rectal modular resection (RMR) or back-to-bilateral-to-front route. This TME-based procedure starts with division of the parietal presacral fascia, creating extra space to preferably protect the hemorrhoidal vascular pedicles and adjuvant organs such as the seminal vesicle and prostate.
Thus, we hypothesize that the RMR procedure might facilitate TME; lessen the complications of surgery; and decrease the occurrence of defecation, sexual, and voiding disorders. The purpose of this study is to present a modified technique for anterior resection in preoperatively treated patients with LARC and provide methodological guidance for surgeons, especially surgical trainees.
Methods
Patients
From January 2019 to December 2021, patients diagnosed with rectal cancer by biopsy at the Division of Colorectal Surgery, Department of General Surgery, Peking Union Medical College Hospital, were enrolled.
Inclusion criteria were as follows: (1) the distance from the lower edge of the tumor measured through endoscopy and radiographic diagnosis should be <7 cm and more than 3 cm from the anal verge—such patients required low anterior rectum resection or abdominal perineal resection, involving problems such as preservation of anal and reproductive functions; (2) rectal MRI assessment of the tumor should be radically resectable, all patients were above T3 and N1 and received neoadjuvant therapy; and (3) male patients.
Exclusion criteria were as follows: (1) patients with intraoperative factors, such as intra-abdominal implantation metastasis, and patients unable to undergo surgery; (2) organ transplant patients, patients who have received or are receiving immunotherapy; and (3) patients who cannot be followed up for various reasons such as mental and psychological factors.
RMR was performed individually in our center by experienced surgeons, of which all were required to have experience of performing at least 80 laparoscopic surgeries for rectal cancer per year. The study was approved by the Ethics Committee of Peking Union Medical College Hospital. We collected the information above from the patient's medical records and by telephone follow-up.
Surgery procedures
More details can be seen in the supplying video (Supplementary Video S1). For the RMR group, surgery was performed in three steps (Fig. 1):
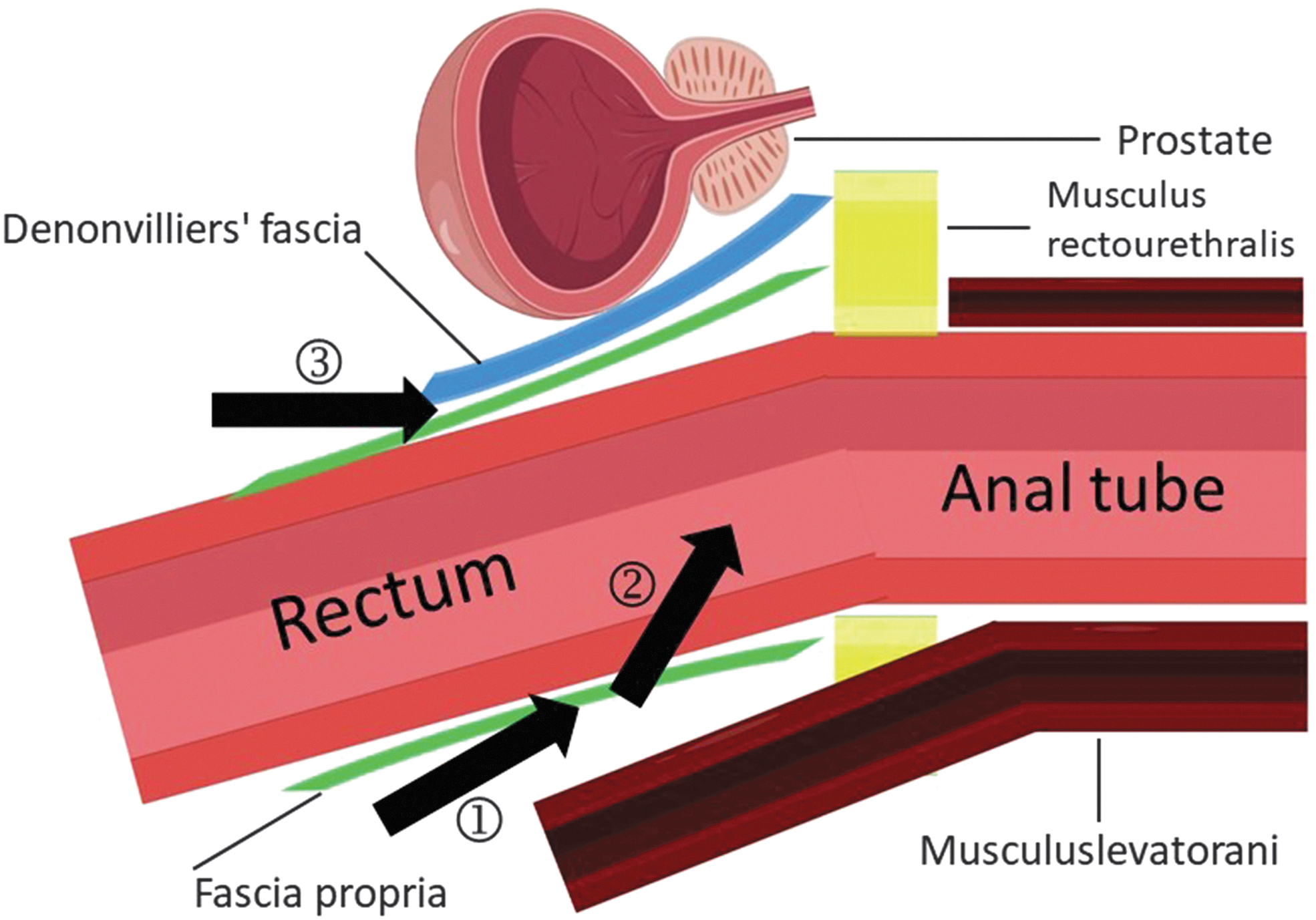
The procedure of rectal modular resection. Figure produced by https://www.figdraw.com, the authorization number is URSIYYe2ee2.
After ligation of the superior rectal artery, RMR starts posteriorly of the rectal artery and sigmoid mesocolon. Pull the inferior rectal artery upward, and there is an avascular space behind the sigmoid mesocolon in the pelvis. Gently retract the sigmoid colon or the upper rectum anteriorly to facilitate identification of the avascular presacral space between the fascia propria and the presacral fascia. The dissection starts at the transition of the mesosigmoid to the mesorectum and enters the avascular space in the midline using electrocautery or an ultrasonic scalpel. The RMR principle emphasizes dissection into the “real holy plane,” which is the space between FPR (i.e., the visceral fascia) and urogenital fascia (UGF), dividing the parietal presacral fascia to the distal margin of the tumor.
Incise and divide the lateral ligaments of the rectum, which contain the middle hemorrhoidal vascular pedicles. Proceed with dissection to the level of the distal margin of the tumor or pelvic diaphragm. The ligament is ligated without injuring the more caudally located neurovascular bundle (NVB) or the underlying inferior hypogastric plexus.
Incise the peritoneum ∼5 mm anterior to the fold of the cul-de-sac, exposing the seminal vesicles that are cleared by sharp dissection with an ultrasonic scalpel. Continue the plane of dissection anteriorly, until the junction with the prostate capsule is reached.
For rectal cancers located anteriorly, Denonvilliers' fascia is separated from the prostate capsule to provide a clear margin. For rectal cancers located posteriorly, the dissection is performed in the plane closer to the anterior surface of the rectum, leaving Denonvilliers' fascia intact to preserve the nerves.
For the classical procedure resection (CPR) group, the same resection extension was performed according to the surgeon's own habits, without strict compliance with the three steps. 8 Both groups received laparoscopic resection and no conversion to open surgery was made. After the rectum resection, stapled anastomosis was performed to reconstruct the alimentary tract in all patients. Drainage of the surgical field was regularly performed, and protective transverse colostomy or ileostomy was performed according to the surgeon's discretion.
Definitions and outcomes
The primary endpoint of the study was the anus preservation rate after the surgery. The secondary endpoints of the study were perioperative and pathology outcomes, including complications and specimen quality. An additional secondary endpoint was the sexual and defecation function after surgery.
Anastomotic leak was defined as a complete intestinal wall defect at the anastomotic suture line, allowing intra- and extraluminal spaces to communicate, which is detected by means of endoscopy, radiological contrast enema, thin-layer CT, or surgery. The severity of anastomotic leakage was graded as follows
9
:
Grade A: anastomotic leakage results in no change in patients' management. Grade B: leakage requires active therapeutic intervention, but is manageable without relaparotomy. Grade C: anastomotic leakage requires relaparotomy.
Perioperative complications, including anastomotic leak, anastomotic site hemorrhage, impaired wound healing, urine retention, ileus, stoma-related complications, thromboembolic events, and other adverse events, were recorded. Complications were graded according to the Clavien–Dindo classification; grade I–II events are classified as minor complications and grade III–IV events are classified as serious complications. 10 Specimens are pictured and examined by surgeons and pathologists. TME completeness is scored as complete, nearly complete, or incomplete based on four parameters: bulk, surface regularity, defects, and coning. 11
A self-assessment questionnaire, low anterior resection syndrome (LARS) score, measured bowel dysfunction. The LARS questionnaire consists of five questions where each question has response alternatives with a weighted score. The International Index of Erectile Function (IIEF-5) score measured sexual ability.
Statistical analysis
Categorical and ordinal variables are summarized as means of frequencies and percentages and analyzed by the Pearson chi-square or Fisher's exact test. Continuous variables are summarized as medians, means, and range values and analyzed by the t-test or Mann–Whitney U test. Overall survival was calculated with the Kaplan–Meier method.
All reported P values were two-sided and considered significant at the 5% level. SPSS, version 26.0 (SPSS, Chicago, IL), and R, version 4.2.1, were used for statistical analysis.
Results
Patient characteristics
A total of 92 patients were retained for the analysis, as either the RMR group (n = 59) or the CPR group (n = 33). Baseline characteristics, including age, body–mass index, previous history, neoadjuvant therapy, and clinical TNM stages, were confirmed without any statistical differences (Table 1).
Baseline Clinical Characteristics
BMI, body–mass index; CPR, classical procedure resection; RMR, rectal modular resection.
Perioperative outcomes
The anus preservation rate in the RMR group is 53 of 59 patients (89.83%) versus 26 of 33 patients in the CPR group (78.79%) (P = .213). Blood loss is similar in the two groups, with a median loss of 50 mL. Duration of operation was significantly longer in the CPR group than in the RMR group (125.20 versus 169. 61 minutes, P = .000) (Table 2).
Perioperative Outcomes
CPR, classical procedure resection; RMR, rectal modular resection.
As the second endpoint is perioperative outcomes, considering the differences between LAR and intersphincteric APR such as the existence of an anastomotic stoma, only LAR surgery is taken into account. The anastomotic leak rate in the RMR group is 2 of 53 patients (3.77%) versus 4 of 33 patients in the CPR group (15.38%) (P = .087).
Two anastomotic leakage cases in the RMR group were rated as grade 2, while three leakage cases in the CPR group were recorded as grade 2 and one was recorded as grade 3. Although there is no statistical difference between the two groups, the rate and severity of anastomotic leakage tend to be higher in the classical procedure group.
One patient in the RMR group developed stoma ischemia, while 1 patient in the CPR group developed stoma prolapse. Both patients underwent emergency surgical stoma reconstruction and recovered successfully. Urine retention, fever of unknown origin, and ileus were similar in the two groups. Other complications include cerebral infarction, pulmonary infection, acute renal failure, and deep vein thrombosis. All complications were graded according to the Clavien–Dindo classification.
The average duration of hospital stay was 8.5 days in the RMR group and 11.5 days in the CPR group (P = .215) (Table 3).
Perioperative Outcomes (with Anus Preserved Surgery)
CPR, classical procedure resection; RMR, rectal modular resection.
Pathological properties
The distal margin clearance is similar between the RMR group and CPR group (P = .124). The CRM-positive rate between the two groups indicates no statistical difference. More peri-intestinal lymph nodes were harvested with the RMR procedure than the CPR procedure (n = 11.00 versus n = 8.50, P = .028).
CPR and RMR groups show the same proportion of tumor differentiation: well, moderate, poor, and others. For the pathological TNM category, the CPR group shows a larger proportion of T2 stage tumors (35.84% versus 57.69%, P = .029). This may account for the fact that RMR can isolate the specimen more completely.
It is to be noted that the RMR group can reach a higher percentage of complete TME than the CPR group (77.36% versus 61.54%, P = .033) (Table 4). Specimen quality is classified into three subtypes: complete, nearly complete, and incomplete (Fig. 2). More specimens in the RMR group achieved the complete grade, while there is no remarkable difference between the two groups in the nearly complete and incomplete categories.
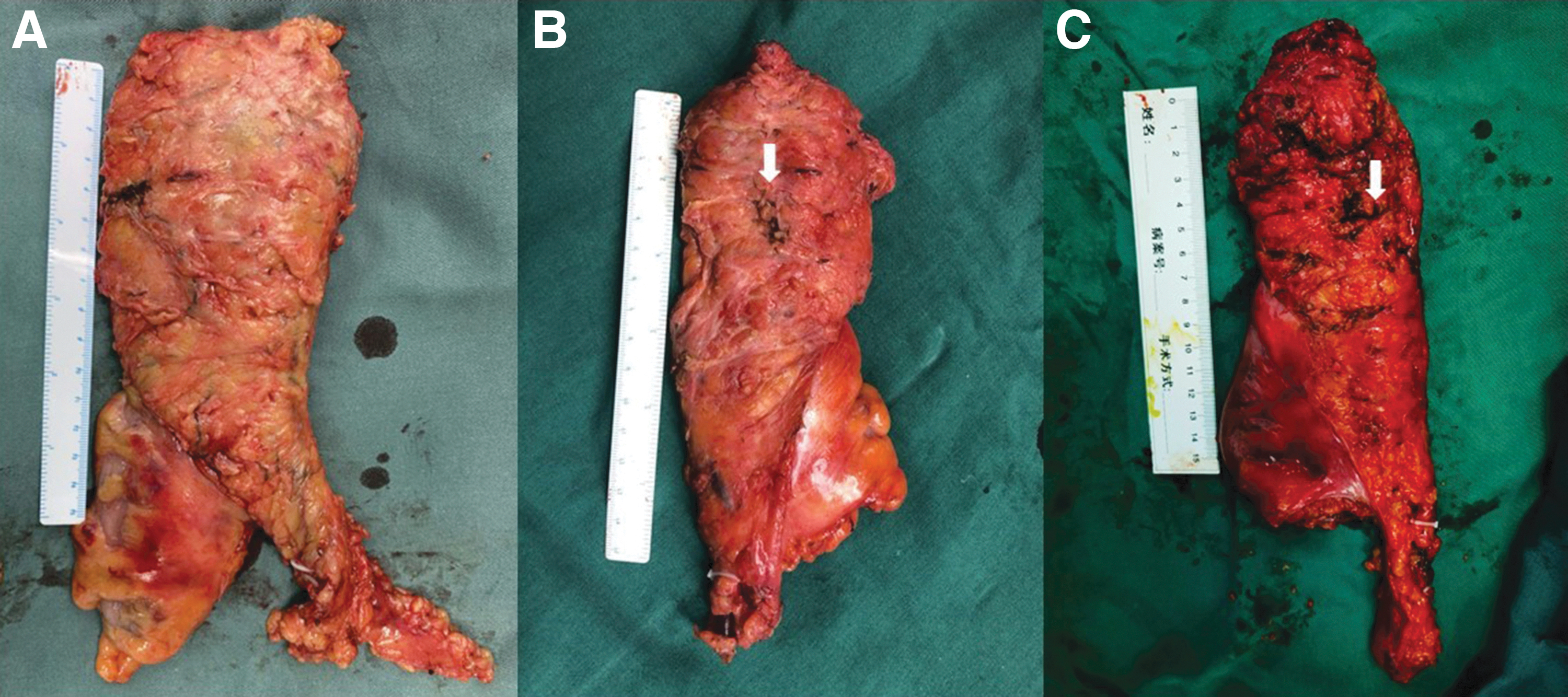
Specimen grading:
Pathological Properties
Tumor differentiation–other includes pathological complete remission, mucinous adenocarcinoma, and adenocarcinoma unable to acquire specific types of differentiation.
CRM positive refers to CRM ≤1 mm.
CPR, classical procedure resection; CRM, circumferential resection margin; RMR, rectal modular resection.
Long-term outcomes
Fifty patients in the RMR group and 25 patients in the CPR group were followed up to more than 1 year. The 1-year disease-free survival rate remains the same between the two groups (92% versus 100%, P = .51) (Fig. 3) and the patients continue to be followed. The function of the rectum is assessed by the LARS questionnaire 3 months and 1 year after surgery.
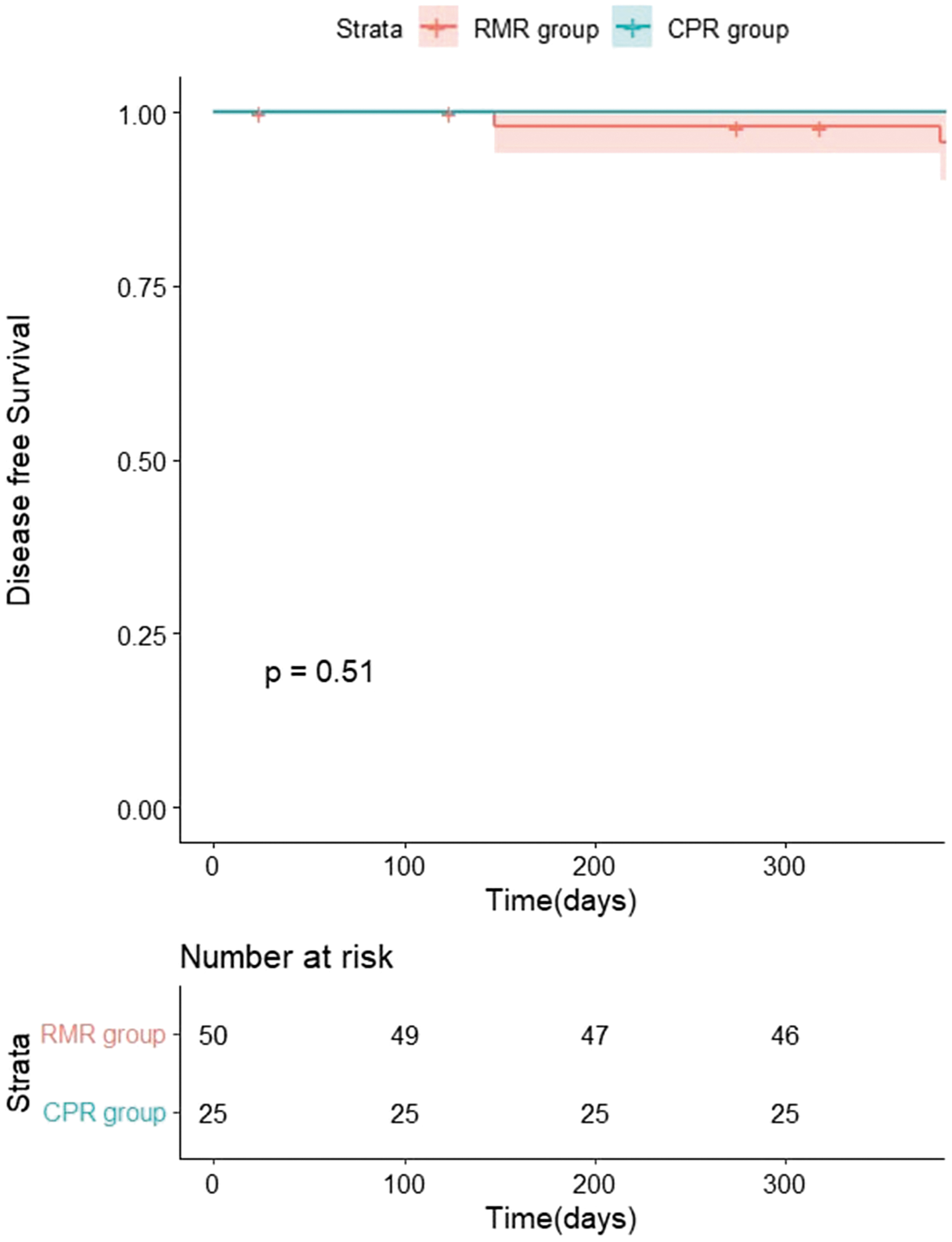
One-year disease-free survival rates of the two groups.
After excluding patients who died during peripheral surgery, were lost to follow-up, or refused to be investigated, 31 patients in the RMR group and 15 patients in the CPR group finished the LARS questionnaire. Results revealed no statistical differences between the two groups (Table 5).
Long-Term Functional Outcomes
CPR, classical procedure resection; LARS, low anterior resection syndrome; RMR, rectal modular resection.
The sexual ability function is assessed by the IIEF-5 questionnaire. Eleven patients in the RMR group and 6 patients in the CPR group finished the IIEF-5 questionnaire, with no significant difference between the two groups (Table 6).
Long-Term Functional Outcomes
CPR, classical procedure resection; IIEF-5, International Index of Erectile Function; RMR, rectal modular resection.
Discussion
TME is widely accepted as the standard surgical approach to ensure negative circumferential resection margins.8,12–14 TME employs precise sharp dissection between the visceral and parietal layers of the endopelvic fascia to ensure intact removal of the perirectal areolar tissue, including the lateral and circumferential margins of the mesorectal envelope, lymphatics, and vascular/perineural tumor deposits, with the primary lesion.
However, in practice, more details are needed to achieve complete TME without tumor residual or unnecessary damage. When entering the space between the fascia propria and presacral fascia, entering wrong planes may result in bleeding or unnecessary nerve damage. Improper dissection of the lateral ligaments of the rectum may lead to damage of the NVB. Denonvilliers' fascia should be protected if possible as urination and sexual function may be impaired after surgery. For general surgeons, especially surgical trainees, there is no standard procedure or guide for performing the TME technique, therefore inadequate understanding of the surgery routines often results in surgical complications.
In recent years, the content of fascial anatomy has been constantly refreshed based on advances in anatomic and topological understanding by cadaver and video studies. For the fascial structure posterior to the rectum, Liu et al. 15 demonstrated the “real holy plane” and defined the concept of UGF (Ureterohypogastric Fascia). Preservation of the NVB has been facilitated by sharp dissection along the lateral fascial interval.16,17 Controversies around retention of DVF anterior to the rectum have led to prompt precise delineation of the anatomy boundary.18–21
We summarized the development of techniques aimed to improve the TME procedure (Table 7).22,23 However, pitfalls in these approaches remain as they do not provide a systematic view of the whole process of TME. Where to start the surgery approach and how to carry it forward still remain confusing especially for surgical trainees. In addition, nearly all the studies above enrolled subjects who were free of preoperative treatment. Neoadjuvant chemoradiotherapy, especially radiotherapy, could induce tumor regression and restrain local recurrence.
Total Mesorectal Excision Skills and Procedures
LLND, lateral lymph node dissection; MRF, mesorectal fascia; NVBs, neurovascular bundles; TME, total mesorectal excision.
Along with specific and nonspecific treatment-related inflammation responses, tissue edema, adhesion, and blurred fascial gap imposed extra difficulty in operation. Thus, for patients treated preoperatively, the procedure guided by recognition of fascial anatomy markers seems to be rather impractical and inefficient. The back-to-bilateral-to-front continuous navigation method or RMR technique was proposed to circumvent defects above and demonstrate a safe and effective surgery approach for patients after neoadjuvant therapy.
A total of 92 patients divided in a ratio of 2:1 in the RMR group and CPR group were recruited. The anus preservation rate was close in the two groups, with a slight advantage in the RMR group. In this retrospective study, duration of surgery was significantly shortened in the RMR group. Bleeding caused by mobilization in an improper plane would stain the visual field. Clear dissection with the RMR technique improved fluency and efficiency in TME without increase in total blood loss. Perioperative safety was evaluated through surgical complications and revealed no difference in RMR and CPR groups.
The integrity of the mesorectum is key for oncological clearance. The RMR group achieved higher completeness of the mesorectum or better quality of the specimen, and higher yield of peri-intestinal lymph nodes, thus manifesting significant superiority over the CPR group in complying with the TME principle. Long-term survival was hypothesized to improve in the RMR group. For short-term follow-up, no difference in disease-free survival was yet observed in the two groups.
The measurement of IIEF-5 was slightly better in the RMR group without statistically significant differences. All the patients selected received neoadjuvant radiotherapy. Radiation damage to the genital system could be misleading and could reinforce nerve injury, except for those secondary to surgery. Urogenital evaluation has subjectivity and timeliness. Because of the retrospective nature of this study and small number of eligible questionnaires recycled, the evaluation of genital dysfunction could be limited.
Urinary function was recorded as the incidence of urine retention and revealed no difference in the two groups. Along with recovery, urogenital function was observed to have gradually improved. Since long-term follow-up is still ongoing, we assume that with better neuroprotection, significant amelioration of sexual and urination disorders could be reported earlier in the RMR group. Further studies are warranted to improve urogenital functions for patients under radiotherapy. As for LARS, there was no significant difference when a modified surgical technique was employed, and subsequent observation is required.
Reasonable laparoscopic skill is achieved as cases accumulate. 24 With guidance, by steps, the RMR method provided a concise, detailed, and simplified procedure for inexperienced surgeons for the purpose of standardization of TME surgery. Further studies should be conducted during popularization of RMR surgery between other surgeons and centers.
As for limitations, this is a retrospective study conducted in a single center with a limited number of patients. The superiority of the RMR technique, a modified method complying with the TME principle, was primarily discussed with regard to surgical efficiency and safety. The functional evaluation mainly focused on sexual, urination, and defecation disorders. The long-term functional and survival outcomes are to be supplemented in following studies.
Conclusions
RMR-based TME was efficient in lymph node clearance and surgical performance compared with traditional methods. In addition, its safety was confirmed without increase in complication occurrence or failure of organ preservation. The RMR technique could provide clear recognition of the optimal surgical plane, thus leading to improvements in functional and oncological outcomes in further studies.
Footnotes
Acknowledgments
The authors would like to thank their assistants, Zhu Danyang and Wang Yue, for helping out in collecting data from the electronic medical record system and following patients. In addition, the authors want to thank Professor Xiao Yi and Professor Wu Bin for providing some of the needed information as well as advice.
Authors' Contributions
W.C. was involved in conceptualization, resources, writing—review and editing, and funding acquisition. Y.L. was involved in methodology, software, investigation, and writing—original draft. Y.A. was involved in validation, investigation, and writing—original draft. W.S. and X.Q. were involved in resources and writing—review and editing. G.L. was involved in conceptualization, methodology, and funding acquisition. J.Z. was involved in conceptualization and writing—review and editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by the CAMS Innovation Fund for Medical Sciences (2021-I2M-C&T-B-019) and the National High Level Hospital Clinical Research Funding (2022-PUMCH-C-005).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.