
Abstract
Background:
The current gold standard of treatment for giant hiatal hernias (GHHs) is laparoscopic surgery. Laparoscopic surgery was performed as a less invasive procedure for paraesophageal hernias more than 25 years ago. Its viability and safety have almost all been shown.
Materials and Methods:
A review of recent and current studies' literature was done. Prospective randomized trials, systematic reviews, clinical reviews, and original articles were all investigated. The data were gathered in the form of a narrative evaluation. We examine the state of laparoscopic GHH repair today and outline the GHH management strategy.
Results:
In this review, we clear up misunderstandings of GHH and address bad habits that may have contributed to poor results, and we have consequently performed a methodical evaluation of GHH. First, we address subcategorizing GHH and provide criteria to define them. The preoperative workup strategies are then discussed, with a focus on any pertinent and frequent atypical symptoms, indications for surgery, timing of surgery, and the importance of surgery. The approach to the techniques and the logic behind surgery are then presented along with some important dissection techniques. Finally, we debate the role of mesh reinforcement and evaluate the data in terms of recurrence, reoperation rate, complications, and delayed stomach emptying. Finally, we suggest a justification for common postoperative investigations.
Conclusions:
Surgery is the only effective treatment for GHH at the moment. If the right operational therapy principles are applied, this is generally successful. There is a growing interest in laparoscopic paraesophageal hiatal hernia repair as a result of the introduction of laparoscopic antireflux surgery. Today's less invasive procedures provide a better therapeutic choice with a lower risk.
Introduction
A
Although most people with hiatal hernias continue to have no symptoms and only receive incidental diagnoses, GHHs are usually symptomatic and associated with severe acid regurgitation, heartburn, or other reflux symptoms. Some patients may develop severe symptoms such as acute ischemia, mechanic obstruction, bleeding, and volvulus. Because medical treatments are insufficient for this anatomical issue, surgical therapy is the only approach to cure symptoms while avoiding serious consequences. The widespread acceptance of minimally invasive surgery for upper abdominal surgery in the last 15 years has changed the surgical approach to these hernias, and laparoscopic GHH repair has been demonstrated as an effective and safe procedure with significant improvement in outcomes and a low recurrence rate.4–7 Robotic-assisted GHH repair has also gained favor in recent years, however, it is not widely used at the moment and is technically the same as laparoscopic resection.
This article review examines the state of laparoscopic GHH repair today and outlines the GHH management strategy.
Risk Factors
Although the real causes of hiatal hernias are unknown, there are two possible mechanisms that are mostly accepted: (1) gastroesophageal reflux disease (GERD) can induce esophageal scarring and shortening, causing traction on the gastroesophageal junction and resulting in gastric herniation; (2) gastric displacement into the chest is caused by prolonged positive pressure on the diaphragmatic hiatus, combined with a predisposition to herniate. As risk factors a sedentary lifestyle has been linked to increased body mass index, increased abdominal pressure, and other variables. 8 According to literature, people with a body mass index (BMI) over 25 are far more likely to suffer from hiatal hernia. 9 Hiatal hernias are more common in elderly people who have thoracic abnormalities such kyphosis, scoliosis, and osteoporosis, which increase the thorax's anterior–posterior diameter. 10 In addition, as people age, the phrenoesophageal ligament becomes looser, which increases the likelihood of developing a hiatal hernia. 9 The most frequent cause of congenital abnormalities in children is intestinal malrotation, occasionally linked to other embryologic malformations. 9
Classification
Hill and Tobias in 1968 divided hiatal hernias into four classes, which are shown in Figure 1. 11 Type I hiatal hernias are identified when the gastroesophageal junction slides through the hiatus into the chest, in fact they are also known as sliding hiatal hernias, which account for the majority of cases (80%). The following three categories are the so-called paraesophageal hernias (PEHs); type II hernias are caused by a herniation of the stomach fundus through the hiatus, with the gastroesophageal junction remaining in its correct place; and the most prevalent are type III PEHs (5%–10%), which are a combination of type I and type II with a misplaced gastroesophageal junction and herniation of portions of the stomach into the chest; type IV PEHs are distinguished by a big PEH associated with a major hiatal defect involving not only the stomach but also other intra-abdominal organs such as the colon or spleen.
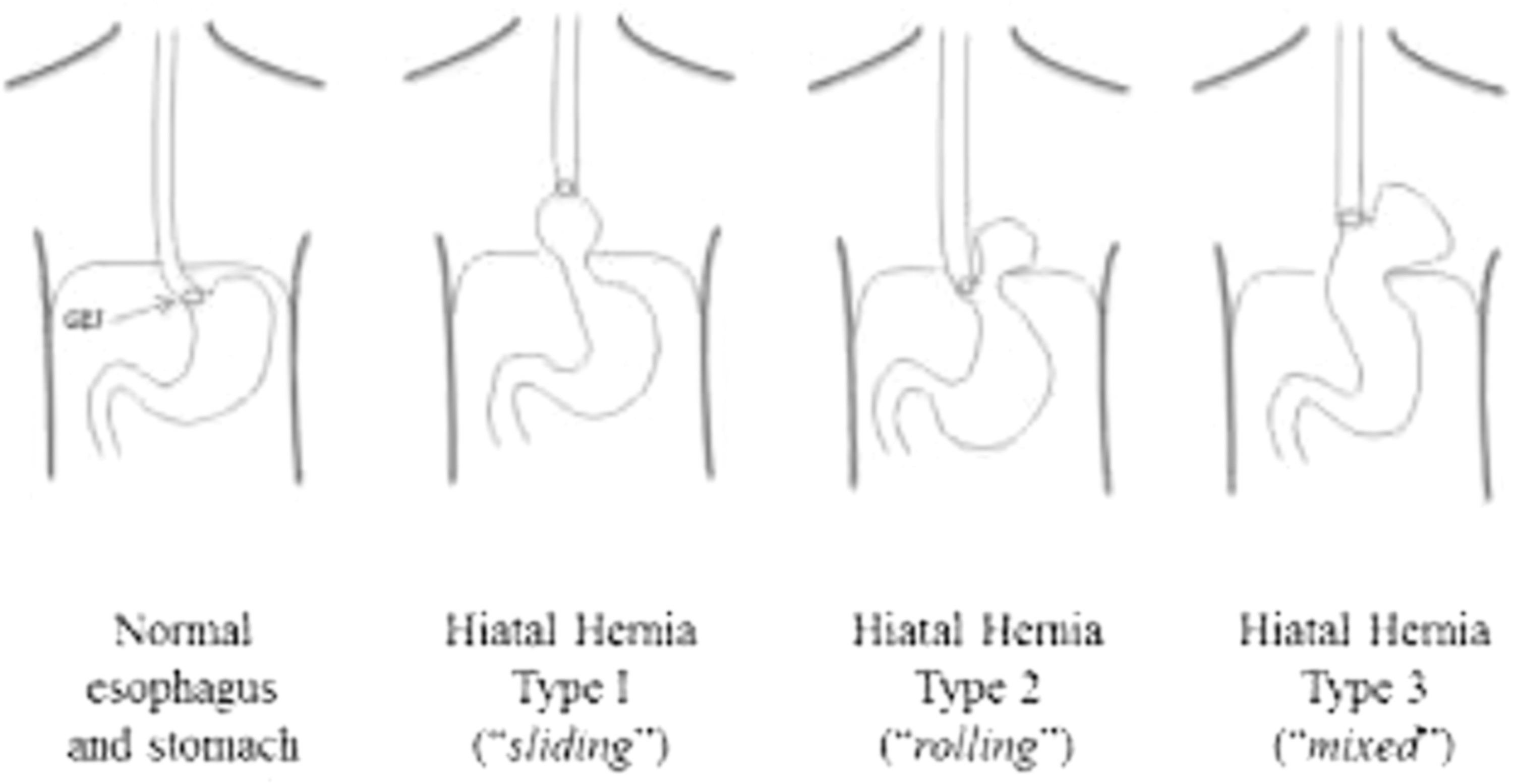
Classification of hiatal hernias from Jalilvand et al. 12
There is no standard definition for GHH; some authors define it as a herniation including more than 30% of the stomach, while others define it as a herniation involving more than 50% of the stomach. Unquestionably, a GHH should be addressed when more than 30% of the stomach herniates into the chest.
Clinical Evaluation of Patients with GHH
Patients with a GHH generally present with pain, heartburn, or a history of heartburn, dysphagia, vomiting, and anemia (in order of decreasing frequency).13–15 A barium esophagogram may be conducted on a patient with a GHH to determine the size of the hernia, as well as whether there are any strictures or axial or longitudinal rotation (Fig. 2), however, due to the growing use of endoscopy, hiatal hernias are frequently detected during endoscopy performed for other symptoms or disorders. Hiatal hernias have been associated with GERD, which can lead to additional esophageal illness. Hiatal hernias are linked to GERD, and this might result in further esophageal disease, the existence and degree of which can be assessed by endoscopy. Endoscopy can reveal the amount of esophagitis, the size of the hiatal hernia, the presence of neoplasia, and even the possibility of delayed stomach emptying.

Barium esophagogram showing large PEH (type III). The fundus of the stomach and the gastroesophageal junction are positioned above the diaphragm. PEH, paraesophageal hernias.
Manometry may aid in identifying individuals with motility problems that may require a different surgical strategy; however, manometry is not always physically viable in large hernias with rotation. For patients with potential problems from a volvulized PEHs, a computed tomography scan can be useful, especially in an emergency situation. In most cases, the organs that have migrated into the chest cavity and the hernia site are clearly visible (Fig. 3). Finally, pH monitoring is either superfluous or unreliable in the context of a GHH.

Computed tomography revealed a giant hiatal hernia with the stomach, ileum, and colon in the thoracic cavity.
Indications for Surgery
Any patient with a GHH should be considered a surgical candidate unless comorbidities are prohibitive; in fact, a meticulous cardiopulmonary investigation is necessary in most cases. 16 Symptomatic PEH is always an indication for elective surgical repair to avoid the potentially serious complications, such as acute strangulation, volvulus, massive hemorrhage, and perforation.17,18
Surgical Principles of GHH Repair
Many of the principles of standard fundoplication apply to GHH repair, the most important of which is the tension-free repair of the crura. 19 The standard approach is laparoscopically via the abdomen. Laparoscopic surgery is just as effective as open surgery in terms of recurrence rate and postoperative complications, according to several studies, if an experienced laparoscopic surgeon carries out the procedure.2,20,21 Hospitalization is shorter after laparoscopy and patients experience less pain. 22
The fundamental critical steps of the laparoscopic paraesophageal hiatal hernia operation include the following: (1) excision of the hernia sac in its entirety; (2) assessment of esophageal length by intraoperative evaluation of esophageal length and appropriate use of esophageal lengthening procedures; (3) adequate mediastinal esophageal mobilization; (4) crural repair; and (5) addition of fundoplication. 23 The likelihood of intrathoracic wrap migration and recurrence is increased by incomplete dissection of the sac. Similarly, a crucial step in minimizing wrap migration and recurrence postoperatively is an adequate mobilization of the esophagus to establish enough abdominal length of the esophagus (2–5 cm).
Collis gastroplasty can be performed to achieve this maneuver in the case of a short esophagus. 24 Of note, a Collis gastroplasty should not be used in place of extensive mediastinal mobilization, because the distal esophagus may be exposed to acid if a portion of the tubularized stomach remains above the fundoplication, and it may also enlarge over time, for these reasons it should only be used in cases where it is absolutely necessary.
Sutures or a mesh can be used to fix the crural defect. Nonabsorbable sutures can be used for cruroplasty in a continuous or interrupted method. Although some sutures may need to be put anteriorly if the crura remain splayed following posterior cruroplasty, the majority of the sutures are placed posterior to the esophagus.25,26 Mesh can be utilized to support the crural repair (Fig. 4), and the surgeon's personal preferences and the size of the hiatal defect will determine which mesh is used (some surgeons only use mesh when the hiatal defect is substantial or >5 cm).27,28 A 6-month recurrence rate of 24% versus 9%, respectively (P = .04), was found in a multicenter, prospective, randomized trial of laparoscopic GHH (i.e., >5 cm) repair comparing primary crural repair (n = 57) versus primary crural repair reinforced with porcine small intestinal submucosa (n = 51). 29

Large hiatus hernia reinforced with Gore Bio-A mesh.
Complete, partial, anterior, or posterior fundoplications are the several types of fundoplications. Nissen30–32 (Fig. 5) and Toupet33,34 are the two most popular varieties. In addition to fundoplication, some surgeons utilize tube gastrostomy or suture the wrap to the crura or the stomach to the front abdominal wall to further prevent recurrence.7,35

Laparoscopic view of posterior Nissen fundoplication.
Surgical Procedures
The patient is positioned supine in the steep reversed Trendelenburg position, which is the lithotomy position. To produce an optimal intra-abdominal working area, complete muscular relaxation is crucial. Ports, 5–11-mm, are utilized during the laparoscopic surgery in positions comparable with those of the Nissen fundoplication (Fig. 6).

Trocar placement for laparoscopic PEH repair. PEH, paraesophageal hernias.
A 12-mm trocar is introduced about 2 cm supraumbilically. The liver retractor is inserted via a 5–12 mm trocar and positioned as high as feasible to the left side of the falciform ligament, at the angle between the xiphoid and the apex of the left costal border. This device exposes the hiatal defect by retracting the left lobe of the liver upward and slightly to the right. The following three ports are placed similar to this: a 5-mm port in the right midclavicular line that is immediately subcostal, a 5–12-mm trocar at the intersection of the left midclavicular line and transverse umbilical line, and a 5-mm port in the anterior left axillary line that is about 3 cm below the costal margin. After the ports have been placed, the hernia's size and the hernia sac's contents are initially examined (Fig. 7).

After the ports are placed, the stomach is retracted, exposing the large hiatal defect.
The first phase in GHH repair is to entirely reduce the hernia contents; however, in particularly big hernias, this is usually not possible until the hernia sac has been fully dissected. Therefore, by severing the gastrohepatic ligament at its flaccid end, dissection is started. The hernia sac is separated along the free margin of the hiatus as the right crus is visualized. To ensure that the sac is released very far posteriorly on the left, this is prolonged onto the left crus. After that, the sac is pulled and the peritoneum is fully mobilized within the mediastinum (Fig. 8).

The incision of the peritoneum along the crural edge allows access to adipose tissue in the posterior mediastinum, and the sac can be dissected easily out of the mediastinum.
Once removed from the chest, the sac remains attached to the front surface of the stomach. Dissection in this area should be done with caution to avoid damaging the left vagus nerve, blood vessels, or the stomach or esophageal wall. However, if the peritoneal sac is very thick, it may be trimmed. Now that the esophagus is raised on a silicone loop, it can be seen and examined. This enables us to create a window posterior to the esophagus, which may then be further released from its connections in the mediastinum to achieve the proper length. Sutures are then used to close the hiatus. Two or more interrupted figures of 2/0 nonresorbable monofilament stitches are used to approximate the left and right pillars. The first stitch should be placed just above the point where the two crura meet. To avoid ripping the muscle, the stitches should incorporate enough tissue. The reconstruction should be tension-free. It is essential to avoid stenosis of the esophageal hiatus. Mesh, such as polypropylene, Gore-Tex®, or denatured animal tissue, can be used to reinforce the hiatal defect and is attached to the diaphragm via metallic staples or stitches (Fig. 9). The mesh is ∼4–5-cm long and is cut with a keyhole to encircle the esophagus and overlaps posteriorly. The mesh is positioned over the hiatal musculature (Fig. 4).

Different types of meshes used to reinforce hiatal defect:
The short gastric vessels are separated with an energy device after the hiatal defect has been repaired. A fundoplication, which can be performed as a 360° Nissen (Fig. 5) or a 270° Toupet surgery, completes the procedure. Preoperative esophageal motility is used to choose which procedure is more feasible. A Toupet fundoplication is advised if a significant motility impairment was identified. Finally, an abdominal drainage tube is inserted near the diaphragmatic hiatus.
Postoperative Management
In general, a nasogastric tube is not placed because the majority of patients do not tolerate it well and is considered a needless discomfort. Patients are advised to adopt incentive spirometry and start walking immediately. It may be necessary to perform a gastrografin esophagogram, particularly if the dissection was challenging and if symptoms such as severe pain, nausea, or fever are present. Oral analgesics such as paracetamol are effective for pain management within the first 24 hours following surgery; tramadol or any synthetic opioid, and nonsteroidal anti-inflammatory drugs can all be used too.
As antiemetic drugs, metoclopramide or ondansetron is usually preferred. Vomiting and retching must be controlled to protect the fundoplication and the repaired hiatus from damage. On the night after surgery, patients begin a liquid diet and progress to pureed food as tolerated. For about 3 weeks, fresh bread and meat should be avoided. After surgery, a regular diet may normally be resumed after 6 weeks.
Follow-Up of Patients and Recurrence
There are no guidelines for patient follow-up after a GHH repair. Although recurrences typically happen within the first 2 years following surgery (but may happen several years after the repair), it is known that mucosal pathology may persist or even advance in many patients who have preoperative mucosal abnormalities (esophagitis, stricture, or Barrett's esophagus) and that postoperative symptoms correlate poorly with objective abnormalities.36–38
The recommended follow-up protocol invites for performing the following: (1) every year for 5 years, a validated symptom questionnaire; (2) every year for the next 5 years, anatomic evaluations (radiographic or endoscopic) can be performed; (3) endoscopic evaluations of patients with preoperative esophagitis, stricture, or Barrett's esophagus within a year after surgery; and (4) long-term monitoring of esophageal mucosal abnormalities that continue or worsen without anatomic recurrence. Until a normal postoperative pH testing or regression has been verified, it is unclear if every patient with preoperative mucosal disease should receive postoperative proton pump inhibitor treatment.
There is no standard or accepted definition of recurrence in the published literature. Some authors consider that the migration of the wrap must be at least 2 cm above the diaphragm, 24 however, some have defined it as any degree of herniation (range 30%–50%) of the wrap above the diaphragm.1,25,39
There are numerous methods for objectively assessing recurrence. The most adopted method is an esophagogram, which was utilized by almost all the studies evaluating recurrence.24–28,30–33,37,38,40 The second most common method was esophagogastroscopy.1,34,35 However, an ambulatory esophageal pH study, which is considered to be the gold standard for objective evaluation of recurrence of GERD symptoms, was utilized the least in the literature.1,26,32,39 In assessing major recurrences or patients with acute conditions, computed tomography can be effective.
When to Reoperate
Reoperative indications include herniation symptoms such as incarceration or obstruction, dysphagia, anemia, and dyspnea, as well as reflux symptoms that have not been successfully treated. Reoperation proposals should have a higher bar, especially for elderly patients, because of the increased operating risks and the risk of unsuccessful surgery. The aims of the operation must be determined in relation to the patient's symptoms and objective results, much similar to primary surgery, and the risks must be weighed against the reasonable expectation of benefit. Until the symptoms worsen, continuous medical therapy may in certain situations be the best option.
Evolution of Operative Treatment
Robotics has been increasingly prevalent in operating rooms over the past few years. These devices were created to aid surgeons in overcoming the drawbacks of traditional open surgery and laparoscopic surgery. The potential benefits of such systems set the stage for the next significant growth in the surgical profession. All upcoming generations of surgeons will need to be proficient with these devices as their availability grows and their costs decrease. In addition, as more media attention is given to this technique, it is anticipated that patient requests for robotic surgery will rise.
Cadiere and associates performed the first robotic Nissen fundoplication (1999, France). Results of robotic surgery versus laparoscopic Nissen fundoplication were compared in a prospective randomized experiment done by Cadiere on 21 patients. The results of both methods were comparable, despite the robotic group's much longer operating time (72 minutes versus 52 minutes, P = 0.01). 41
Multiple additional studies comparing robotics and laparoscopic surgery were conducted. These investigations showed that using a robotic platform resulted in an increase in costs and an average increase in operating time of 30 minutes. 42 Robotic surgery, on the contrary, has been shown to be a safe option with clinical outcomes comparable with laparoscopic surgery. Despite the belief that robotic surgery would result in superior patient outcomes in antireflux and hiatal hernia surgery, clinical investigations comparing it with laparoscopy showed otherwise.43–45
It is important to highlight that the majority of the trials involved people who had a small type I hiatal hernia or GERD symptoms. Significant clinical gains might be shown if laparoscopy were compared with robotic platforms with larger and more intricate PEH that demand more dissection and accuracy of movements in the small hiatus. In conclusion, the use of robotics is still an area that is ripe for investigation and prospective trials.
Conclusions
Surgery is the only effective treatment for GHH at the moment. If the right operational therapy principles are applied, this is generally successful. The principles of GHH repair include reducing the stomach, mobilizing the hernia sac from the mediastinum, effectively closing the hiatus, and achieving a sufficient gastropexy. There is a growing interest in laparoscopic paraesophageal hiatal hernia repair as a result of the introduction of laparoscopic antireflux surgery.
Today's less invasive procedures provide a better therapeutic choice with a lower risk. The symptoms are quickly relieved by laparoscopic repair of GHH, which is safe, technically possible, and well tolerated. Excellent hiatus visibility and superior esophageal mobility are made possible by the laparoscopic method, with considerably less surgical trauma to this frequently elderly and frail patient group. The lower esophageal sphincter is significantly engaged throughout the dissection and is hence probably incompetent, necessitating an antireflux procedure. This does not considerably lengthen the time needed for the operations, and it gives the stomach a great anchoring mechanism to the diaphragm. The use of prosthetic hiatal herniorrhaphy for GHH must be tailored to the operational findings and the surgeon's guidance.
Footnotes
Authors' Contributions
F.D.: Conceptualization (lead); writing—original draft (lead); formal analysis (lead); and writing—review and editing (equal).
N.T.: Review and editing (equal).
G.R., P.M., and M.S.: Conceptualization.
G.A.: Supervision.
Disclosure Statement
No competing financial interests exist.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.