
Abstract
Purpose:
The purpose of this study was to explore whether liver cirrhosis (LC) influences short-term and long-term outcomes in gastric neoplasm patients who undergo endoscopic submucosal dissection (ESD).
Materials and Methods:
Eligible studies were identified in three databases, including PubMed, Embase, and the Cochrane Library on December 18, 2022. Clinical characteristics, short-term outcomes, and long-term outcomes were compared between an LC group and a no liver cirrhosis (NLC) group. For continuous variables, the mean difference (MD) and standard deviation (SD) were pooled. For discontinuous variables, raw data from the 2 × 2 tables or odds ratio (OR) and 95% confidence intervals (CIs) were pooled. Forest plots were used to show the results, and a funnel plot was used to evaluate publication bias. Data analyses were performed by STATA SE 16.0 software.
Results:
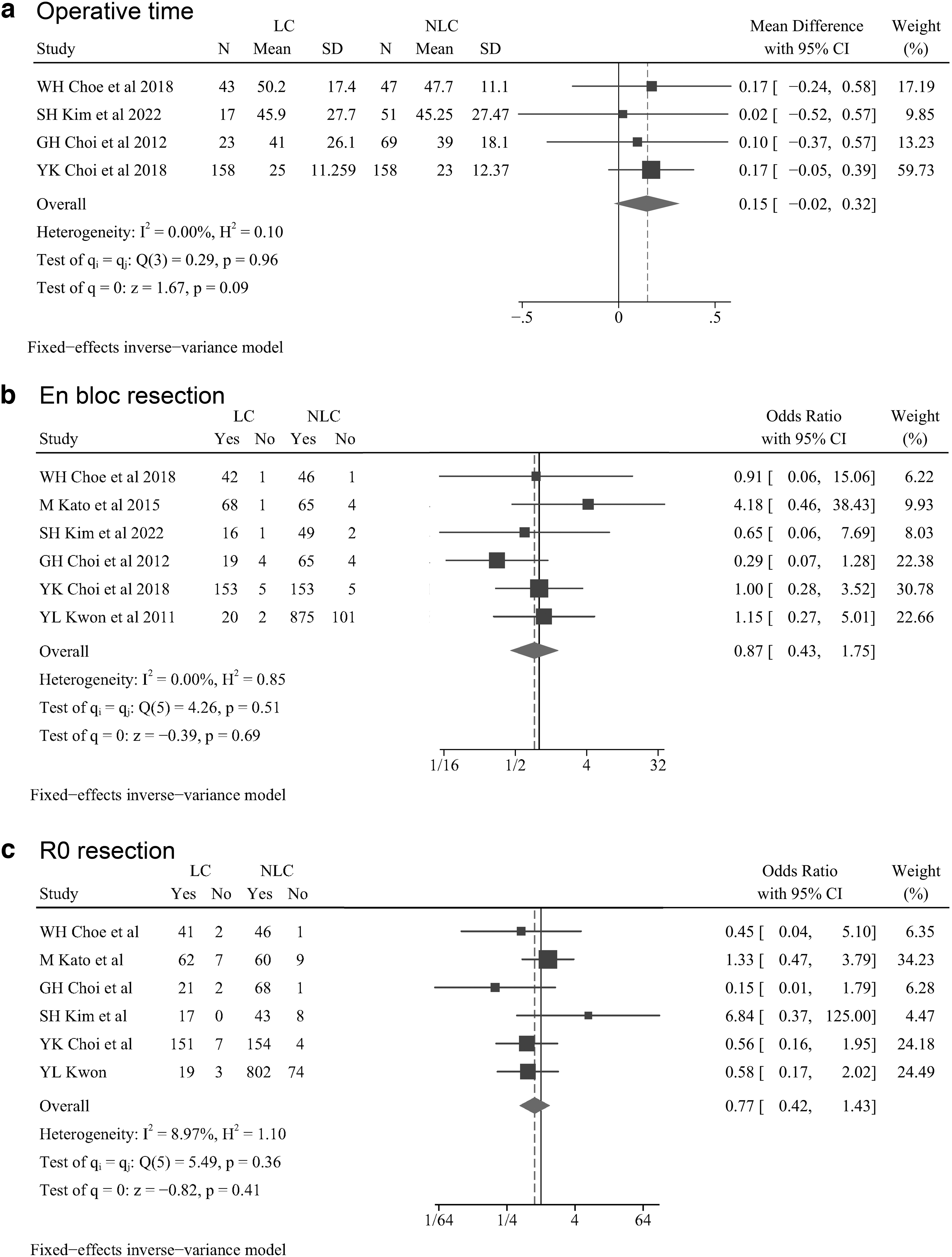
Six retrospective studies involving 1616 gastric neoplasm patients were included in the study. Clinical characteristics, including age, gender, location, macroscopic type, invasion depth, differentiation, and ulceration, were found to be not significantly different between the LC group and the NLC group (P > .05). Moreover, LC was not a risk factor for short-term outcomes, including operative time (MD = 0.15, 95% CI = −0.02 to 0.32, I2 = 0.00%, P = .09), en bloc resection (OR = 0.87, 95% CI = 0.43–1.75, I2 = 0.00%, P = .69), R0 resection (OR = 0.77, 95% CI = 0.42–1.43, I2 = 8.97%, P = .41), bleeding (OR = 1.10, 95% CI = 0.62–1.93, I2 = 0.00%, P = .75), and perforation (OR = 1.62, 95% CI = 0.45–5.84, I2 = 0.00%, P = .46). However, gastric cancer patients with LC exhibited a higher recurrence rate (OR = 3.40, 95% CI = 1.09–10.61, I2 = 0.00%, P = .04) after ESD.
Conclusion:
Surgeons performing ESD in gastric neoplasm patients should pay more attention to long-term effects.
Introduction
Gastric neoplasms are a common disease of the gastrointestinal tract, which include gastric dysplasia and gastric cancer. 1 With the development of medical technology, endoscopic submucosal dissection (ESD) has been accepted as a convenient and less invasive treatment for early and superficial gastric neoplasms. 2 ESD improves the en bloc resection rate because it involves direct dissection of the submucosa beneath the lesion.3,4 However, complications such as bleeding and perforation cannot be ignored; the ranges of their rates of incidence are 0%–15.6% and 1.2%–5.2%, respectively.5,6
Liver cirrhosis (LC) is widely prevalent, with an age-standardized incidence of 20.7/100,00 worldwide. 7 The most common causes of LC include obesity, overconsumption of alcohol, and hepatitis B or C infection. 8 LC imposes a huge health burden on many countries and is especially a problem in some low-income countries. 9 Moreover, patients with LC are at a high risk of bleeding when receiving invasive treatments because of coagulation disorders.10–12
Regarding ESD, several studies revealed that gastric neoplasm patients with LC had a higher risk of bleeding, longer hospital stay, and higher mortality and recurrence rates.13–17 However, Choi et al. demonstrated that LC did not influence the short-term and long-term outcomes in gastric neoplasm patients undergoing ESD; this finding was controversial given previous studies. 18 Therefore, this study aimed to investigate the safety and feasibility of ESD for LC patients.
Materials and Methods
This study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement. 19
Search strategy
The search strategy included three items (gastric neoplasms, ESD, and LC), and text words were used for searching eligible studies. The complete search strategy was as follows: (“gastric cancer” OR “gastric carcinoma” OR “gastric neoplasms” OR “stomach cancer” OR “stomach carcinoma” OR “stomach neoplasms”) AND (“endoscopic resection” OR “endoscopic submucosal dissection”) AND (“liver cirrhosis” OR “cirrhosis” OR “cirrhotic”). The search scope was limited to title, abstract, and keywords. The language was limited to English only.
Inclusion and exclusion criteria
The inclusion criteria were as follows: (1) patients who were diagnosed with gastric neoplasm and underwent ESD; (2) patients were divided into the LC group and the no liver cirrhosis (NLC) group; and (3) short-term or long-term outcomes were reported. The exclusion criteria were as follows: (1) insufficient data; and (2) the study types were conferences abstract, trail, review, meta-analysis, case report, letters to the editor, or comments.
Study selection
The search strategy was conducted in three databases, including PubMed, Embase, and the Cochrane Library. First, duplicated records and studies with unqualified study types were removed. Then, titles and abstracts were screened to exclude irrelevant studies. Finally, the full text would be accessed to find eligible studies according to the inclusion and exclusion criteria. Two authors would conduct the study selection independently, and any disputes would be solved by the third author.
Data collection
Characteristics of both studies and patients were collected. Regarding the included studies, baseline characteristics included author, year, country, study type, sample size, patients, diagnosis of LC, and the Newcastle-Ottawa Scale (NOS). Regarding patients, characteristics that were reported in at least two studies were included for analysis. Baseline characteristics and pathology data included age, gender, location, macroscopic type, invasion depth, differentiation, and ulceration.
Quality assessment
The NOS score was used to assess the quality of eligible studies according to three aspects, including selection, comparability, and exposure. 20 Moreover, high quality is score greater than seven; otherwise, it is low quality.
Statistical analysis
For continuous variables, mean difference (MD) and standardized difference (SD) were pooled. For dichotomous variables, odds ratios (ORs) and 95% confidence intervals (CIs) were pooled; otherwise, raw data from the 2 × 2 tables were collected. The random-effects model and DerSimonian–Laird method were used as the default, and P < .1 was considered statistically significant. The I2 value and the chi-squared test were used to evaluate the statistical heterogeneity.21,22 According to the Cochrane handbook, the I2 < 30% was considered unimportant, 30%–60% was considered moderate, and >60% was considered substantial. The forest plots were used to show the results of the analyses. The funnel plot was used to assess the publication bias. STATA SE V16.0 software was used for all the data analysis.
Results
Study selection
There were 75 studies remaining after the search strategy was performed in three databases (27 studies in PubMed, 48 studies in Embase, and 0 study in the Cochrane Library). Twenty duplicate records were removed first. Then 20 studies with unqualified study types were excluded. Next, titles and abstracts were screened, and 22 studies with irrelevant content were removed. Finally, full texts of the remaining 13 studies were screened, and 6 studies with sufficient data were included. (Fig. 1)
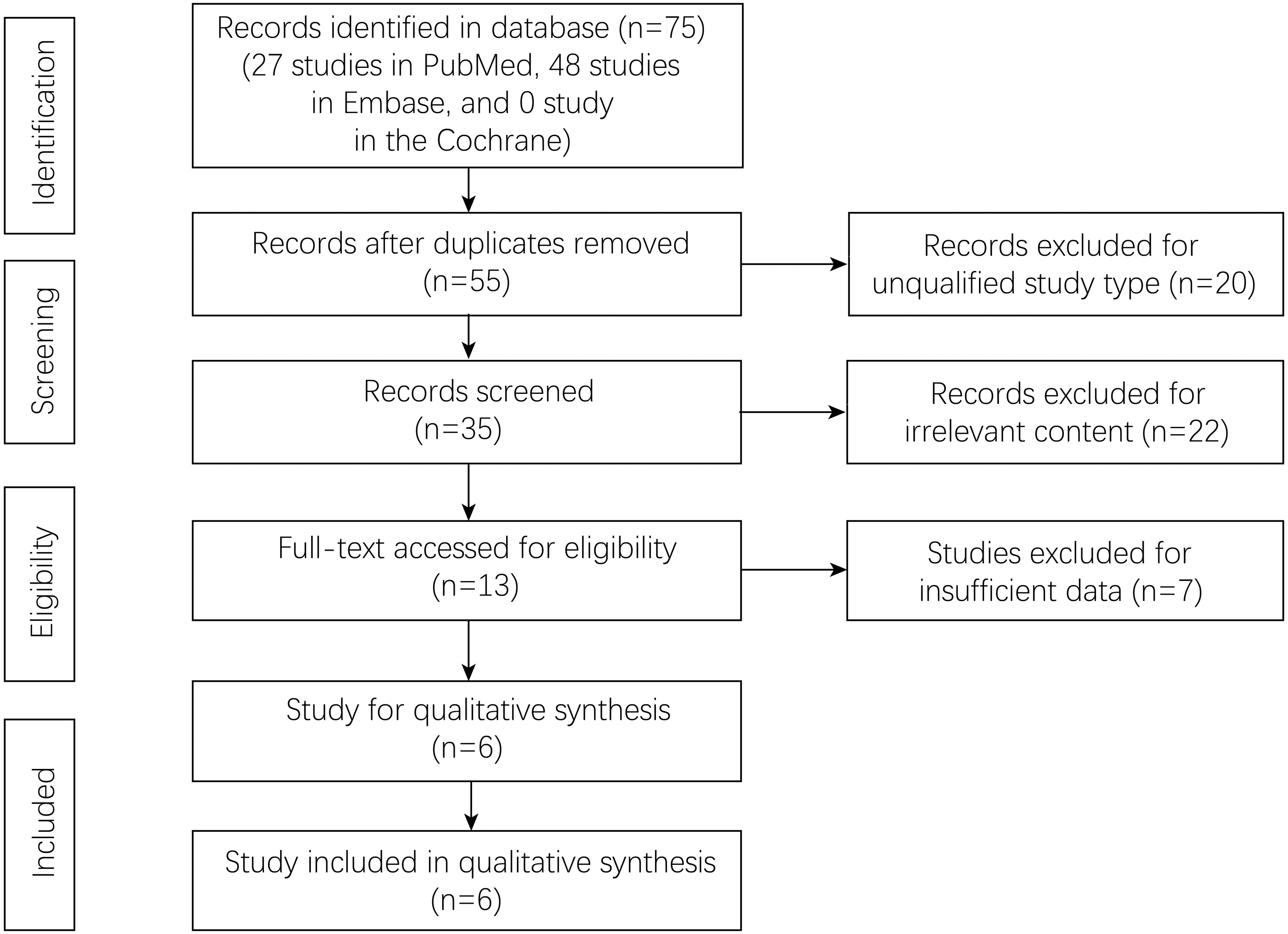
Flowchart of study selection.
Baseline characteristics of the included studies
Six retrospective studies were included in the present analysis. Five studies were performed in Korea, and the other study was performed in Japan. Three studies included only early gastric cancer patients, and three studies included patients with gastric neoplasms. Clinical, biochemical, and radiological data were used for the diagnosis of LC. More baseline characteristics, including author, year, sample size, and NOS score, are shown in Table 1.
Baseline Characteristics of Included Studies
EGC, early gastric cancer; ESD, endoscopic submucosal dissection; HBsAg, hepatitis B surface antigen; LC, liver cirrhosis; NA, not applicable; NLC, no liver cirrhosis; NOS, Newcastle-Ottawa Scale.
Baseline characteristics of the LC and NLC
The baseline characteristics, including age, gender, location, macroscopic type, invasion depth, differentiation, and ulceration, were compared. No significant difference was found between the LC group and the NLC group (P > .1; Table 2).
Summary of Characteristics Between Liver Cirrhosis Group and No Liver Cirrhosis Group
CI, confidence intervals; FE; M, mucosa; LC, liver cirrhosis; NLC, no liver cirrhosis; SM, submucosa.
Short-term and long-term outcomes of LC
In gastric neoplasm patients after ESD, there was no association between LC and short-term outcomes, including operative time (MD = 0.15, 95% CI = −0.02 to 0.32, I2 = 0.00%, P = .09), en bloc resection (OR = 0.87, 95% CI = 0.43–1.75, I2 = 0.00%, P = .69), R0 resection (OR = 0.77, 95% CI = 0.42–1.43, I2 = 8.97%, P = .41), bleeding (OR = 1.10, 95% CI = 0.62–1.93, I2 = 0.00%, P = .75), and perforation (OR = 1.62, 95% CI = 0.45–5.84, I2 = 0.00%, P = .46). Recurrence was observed only in gastric cancer patients, and the results confirmed that the LC group had a higher recurrence rate than the NLC group (HR = 3.40, 95% CI = 1.09–10.61, I2 = 0.00%, P = .04) after ESD. (Figs. 2–3)
Surgical outcomes

Postoperative complications
Publication bias
A funnel plot was used to assess the publication bias. All the plots were inside the 95% CIs, and the plot was relatively symmetrical, which meant that there was little publication bias (Fig. 4).
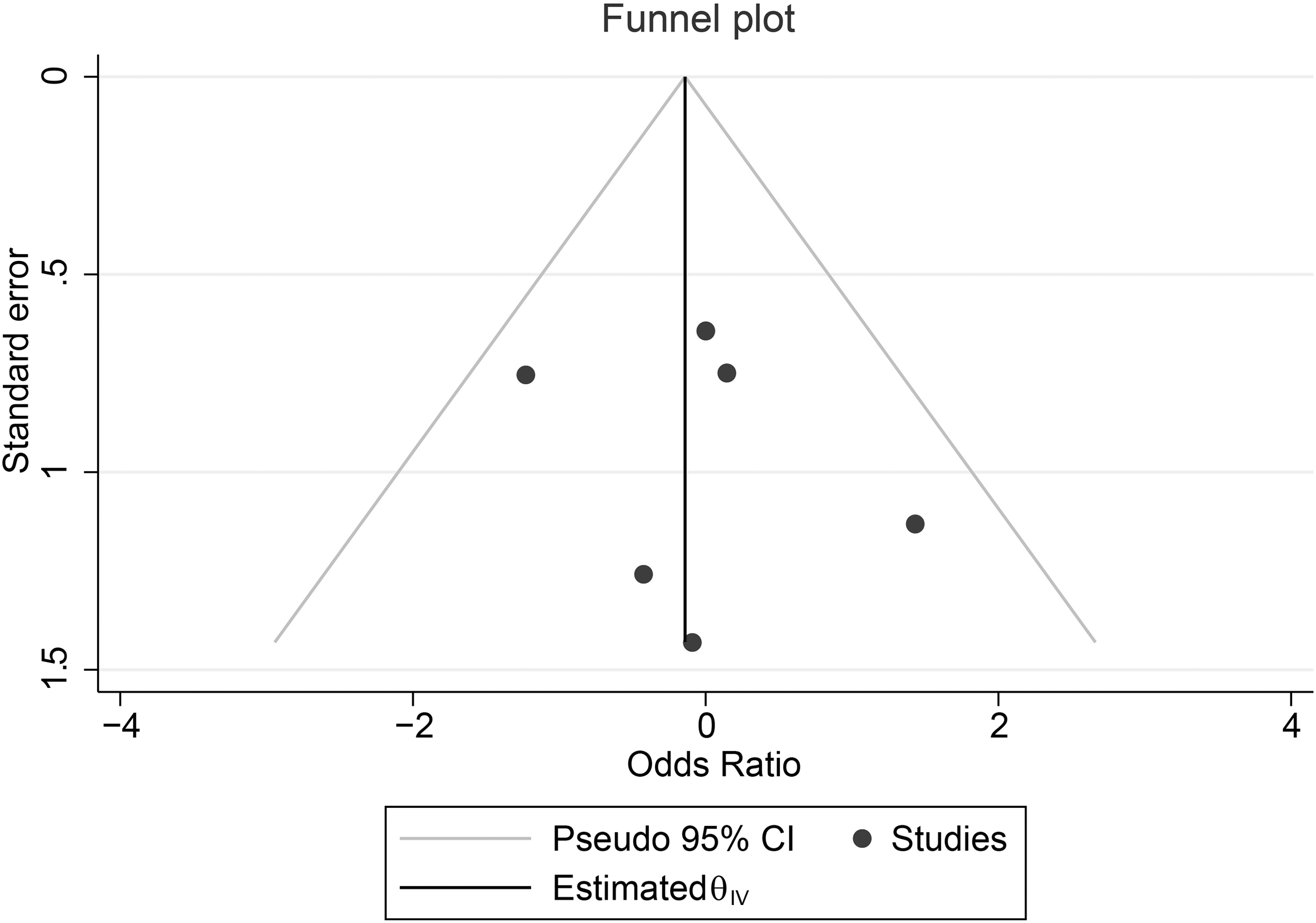
Funnel plot.
Sensitivity analysis
Each study was excluded at once to evaluate the sensitivity of the result, and no significant difference was found in outcomes, which meant the analyses were robust.
Discussion
A total of 1616 patients with gastric neoplasm were enrolled in this study, including 328 patients with LC and 1288 patients without LC. After analysis, there was no significant difference in short-term outcomes between LC and NLC patients after ESD; however, LC patients had a higher long-term recurrence rate of gastric cancer.
Coagulation disorders, including prolonged prothrombin time and thrombocytopenia, are common in LC patients. 23 LC also impairs immune function, leaving patients more susceptible to bacterial infections, which can trigger liver failure. 24 Therefore, LC may influence the postoperative outcomes after surgery for some cancers, including esophageal, lung, and pancreatic cancers.25–27 For gastric neoplasms, several studies have been carried out regarding the clinical outcomes of laparoscopic surgery or open surgery for LC patients.28–31 However, the results may be different for patients receiving ESD.
Although ESD is less invasive than open surgery and laparoscopic surgery, most studies have revealed an adverse effect of LC on gastric neoplasm patients. Choe, Choi, and Kato all found a significantly higher mortality risk and worse overall survival in LC patients13,14,16; however, there were no significant differences in short-term outcomes. Only Kwon conducted a 912-patient study and indicated that immediate bleeding tended to occur more frequently in LC patients. 17 Moreover, Choi did not show any significant differences in short-term or long-term outcomes between the LC group and the control group. Therefore, this study attempted to address the current controversy and provide more accurate results.
In this study, LC patients exhibited a higher long-term recurrence rate of gastric cancer. LC is a kind of chronic liver damage with its loss of architecture and functional failure, which can affect the body's substance metabolism, immune system, and coagulation function.32,33 Therefore, LC may create a microenvironment that promotes tumor cell growth by affecting the metabolism of carcinogens and some hormones.34–36 In addition, changes in the immune system and an increased risk of bacterial infection may also be associated with cancer development.37,38 However, the exact mechanisms of which LC causes gastric cancer recurrence are unclear and need to be explored in more animal trials.
However, this study found no significant difference in short-term outcomes between LC and NLC patients after ESD. The mechanism is unclear, but it might be that ESD is a less invasive treatment method, allowing even patients with LC to tolerate with ESD surgery.39,40
The present pooling-up analysis was the first designed to focus on the safety and feasibility of ESD in gastric neoplasm patients with LC, and the results were highly reliable with low heterogeneity and publication bias. However, the patients included in this study were all from Korea and Japan, which means that the findings may be guiding for Asians only. Moreover, the studies included were all retrospective. Therefore, more prospective studies need to be conducted worldwide for further exploration.
In conclusion, we hope that surgeons performing ESD will pay more attention to its long-term effects in LC patients.
Footnotes
Acknowledgment
The authors acknowledged all the authors in this study.
Data Availability Statement
The data was accessed in the databases.
Authors' Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by F.L., Z.-W.L., X.-Y.L., and W.Z. The first draft of the article was written by X.-R.L. and L.-S.L., the final draft of the article was written by D.P., and all authors commented on previous versions of the article. All authors read and approved the final article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.