
Abstract
Background:
Performing an intracorporeal esophagojejunostomy during laparoscopic-assisted total or proximal gastrectomy is challenging. We developed an ingenious method of overlapping esophagojejunostomy using a linear stapler to avoid stapler-related intraoperative complications.
Methods:
Following lymph node dissection, the esophagus was transected anterior-posteriorly. A linear stapler was used to divide the jejunum ∼20 cm distal to the Treitz ligament. A small enterotomy was then created 5 cm distal to the elevated jejunal stump to insert the linear stapler cartridge. An electronic knife was used to make a full-thickness incision, with the tip of the nasogastric tube (NGT) pressed against the posterior wall of the esophageal stump as a guide. Full-thickness sutures were placed on both the anterior and posterior walls of the entry hole in the esophageal stump to prevent the anvil fork from being misinserted into the submucosal layer of the esophagus. The thread on the posterior wall was guided through the port to the outside of the abdominal cavity, where the linear stapler was inserted to perform the side-to-side anastomosis. A 45-mm cartridge fork and an anvil fork were inserted into the elevated jejunum and esophageal stump entry holes, respectively, following which the esophageal stump was gently grasped. The thread on the posterior wall side was pulled from outside the abdominal cavity through the port. This step is necessary to close the gap between the esophageal and jejunal walls. After confirming that the anvil fork was not misinserted into the submucosal layer of the esophagus and that there was no gap between the esophagus and the elevated jejunum, the linear stapler was fired to create the anastomosis. The insertion hole was closed with hand-sewn sutures or linear staples to complete the esophagojejunostomy.
Results:
Eleven patients underwent this procedure with no anastomotic complications.
Conclusions:
This method enables us to perform an easier and more stable esophagojejunostomy.
Introduction
The Japan Clinical Oncology Group study JCOG1401, a single-arm confirmatory trial of laparoscopy-assisted total or proximal gastrectomy (LATG or LAPG, respectively) with nodal dissection for clinical stage I gastric cancer, was conducted in Japan with the primary endpoint being anastomotic leakage incidence in esophagojejunostomy. 1 As a result, the incidence of suture failure with grades 2–4 (the primary endpoint) in the esophagojejunostomy was 2.5%, and the incidence of in-hospital complications with grades 3–4 was 29%. There were no treatment-related deaths, indicating the safety of both LATG and LAPG. Based on these findings, the Japanese Gastric Cancer Treatment Guideline recommended LATG and LAPG as surgical treatment options for stage I proximal gastric cancer. The use of these surgical procedures is expected to rise in the future. 2
However, intracorporeal esophagojejunostomy is a complicated procedure yet to be standardized.3–6 Intraoperative anastomosis complications are likely to result in postoperative anastomotic leakage, which can be fatal. Hence, an anastomosis method that is both safe and simple is required to facilitate the widespread clinical application of this procedure. 7
We present a method for avoiding intraoperative complications after laparoscopic total gastrectomy (LTG) or laparoscopic proximal gastrectomy (LPG) using a linear stapler. 8
Methods
Esophageal transection
Anastomosis could be performed more easily if the abdominal esophagus was dissected all the way around along the adventitia to increase its mobility. Before esophageal transection, the center of the anterior esophageal wall was marked with a pigment so that the anterior and posterior esophageal walls could be distinguished. The esophagus was transected in the anterior-posterior direction (Fig. 1) because the insertion hole of the linear stapler faced the ventral side (for easy closure) by overlapping anastomosis of the elevated jejunum with the posterior wall of the esophagus. The tip of the nasogastric tube (NGT) to the thoracic esophagus was removed during esophageal transection to prevent the NGT from crossing over the esophageal transection line. Working in cooperation with the assistant, the surgeon aligned the esophagus in the anterior-posterior direction, and dissected the esophagus using a linear stapler.

The anterior wall of the esophagus was marked with a pigment, and the esophagus was transected in the anterior-posterior direction.
Creation of an elevated jejunum
The jejunum was easily elevated to the cranial side, ∼20 cm distal to the Treitz ligament. It was divided using a linear stapler, and the jejunal mesentery was dissected toward the mesenteric root for reconstruction. The distal side of the jejunum was brought up through the antecolic route, and the anastomosis of the esophagojejunostomy was checked for excessive tension. Seromuscular sutures were used to cover the staple line at the blind end of the elevated jejunum. A small enterotomy was created 5 cm distal from the elevated jejunal stump for linear stapler cartridge insertion on the antimesenteric side. To facilitate intracorporeal insertion of the cartridge into the jejunal lumen and prevent misinsertion of the cartridge fork into the submucosal layer of the esophagus, four full-thickness sutures were placed at regular intervals over the enterotomy hole.
A hole was created on the antimesenteric side of the jejunum 40 cm distal to the esophagojejunostomy to perform the Y limb jejunojejunostomy for Roux-en-Y reconstruction, while another hole was created on the antimesenteric side of the stapling line of the previously transected proximal jejunum. The endoscopic linear stapler cartridges were inserted into the proximal and distal jejunum, and a side-to-side anastomosis was performed.
Creation of a small entry hole in the esophageal stump
A small hole was created on the posterior wall of the esophageal stump, which was transected in the anterior-posterior direction. The NGT that had been removed up to the level of the thoracic esophagus was inserted into the anal side of esophagus to press the gastric tube against the esophageal stump. Next, the NGT was guided to the posterior wall side of the esophageal stump, and an electric knife was used to make a full-thickness incision by pressing the tip of the NGT against the esophageal stump for guidance. An NGT was then inserted and guided into the abdominal cavity from the esophageal stump (Fig. 2).

A full-thickness incision was created with an electric knife and the nasogastric tube was further inserted into the abdominal cavity from the esophageal stump.
To prevent the anvil fork from being misplaced in the esophageal stump, full-thickness sutures were placed on the anterior and posterior walls of the small entry hole. The thread on the anterior wall was shortened, while the thread on the posterior wall side was guided through the port to the outside of the abdominal cavity, where the linear stapler was inserted to perform side-to-side anastomosis of overlap esophagojejunostomy (Fig. 3A, B).
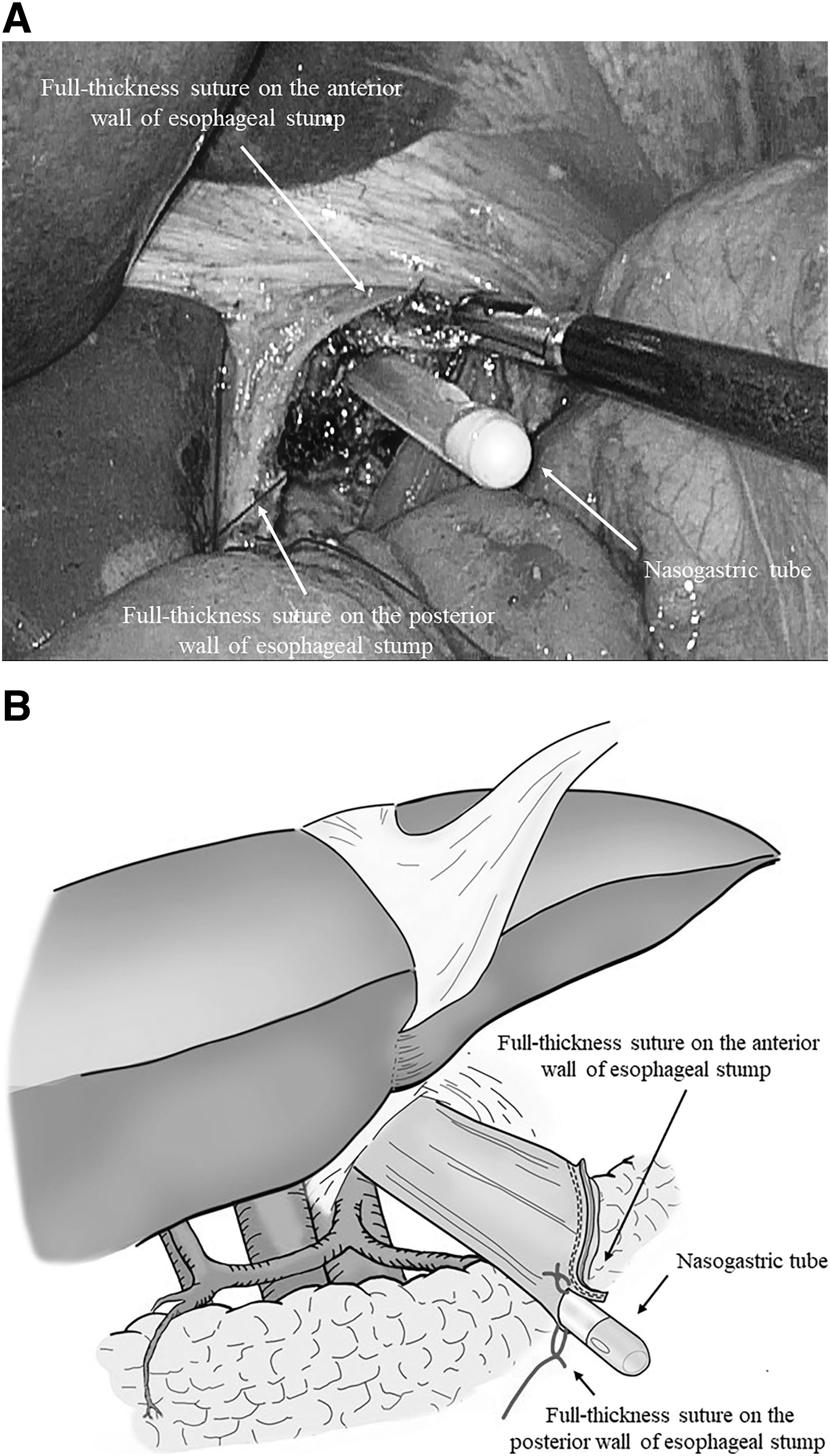
The thread on the posterior wall side was guided to the outside of the abdominal cavity through the port.
Overlap side-to-side esophagojejunostomy
From the port on the right lower abdomen, a 45-mm linear stapler was inserted, and the cartridge fork was inserted into the small entry hole created in the elevated jejunum toward the jejunal stump. The jejunum was moved to the cranial side near the esophageal stump, and an anvil fork was inserted through the small entry hole created in the stump. During the procedure, the anvil fork was inserted into the esophageal lumen through a small entry hole at the esophageal stump. The esophageal lumen was examined using the NGT that had previously been placed in the abdominal cavity as a guide. The NGT inserted up to the thoracic esophagus was removed to avoid accidental involvement when the linear stapler was fired and ensure that the linear stapler did not perforate the esophagus and elevated jejunum.
The most important aspect of this procedure was closing the gap between the esophageal and jejunal walls in an overlap esophagojejunostomy side-to-side anastomosis. The esophageal stump was gently grasped to avoid injuring the esophagus. To close the gap between the esophageal and jejunal walls in the side-to-side anastomosis, the thread on the posterior wall side was pulled from outside the abdominal cavity through the port. After confirming that the anvil fork had not been misinserted into the submucosal layer of the esophagus and that there was no gap between the esophagus and the elevated jejunum, the linear stapler was fired to create anastomosis (Fig. 4A, B). The reliability of the anastomosis and absence of bleeding at the anastomotic site were confirmed.
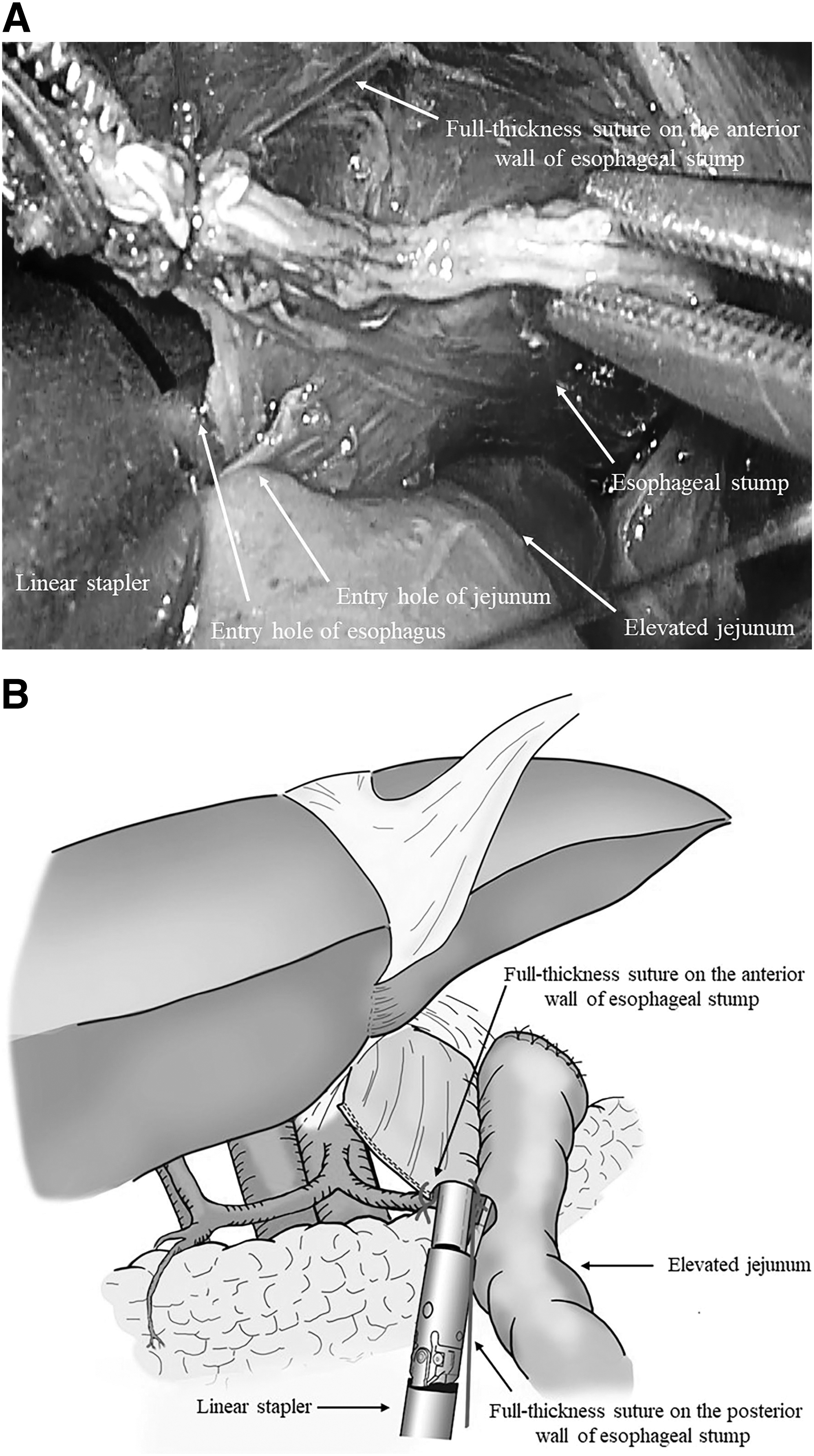
Each fork was inserted into jejunum and esophagus. The thread on the posterior wall side was pulled from outside of the abdominal cavity through the port. Confirm that there was no gap between the esophageal wall and the jejunal wall in side-to-side anastomosis. The linear stapler was fired to create side-to-side anastomosis.
Closing the entry hole with linear stapler
Hand-sewn sutures and a linear stapler were used to close the insertion hole. The insertion hole for the linear stapler was temporarily closed by several hand-sewn sutures at full thickness. The thread was then pulled toward the ventral side to fire the linear stapler (Fig. 5). To complete the esophagojejunostomy, the entry hole was simultaneously resected and closed securely using a linear stapler (Fig. 6), and reinforced with seromuscular sutures as needed. Finally, the air was injected through the NGT to ensure no leakage, the mesenteric gap created by the elevated jejunum and Y limb anastomosis site, and Petersen's defect was closed using a 3–0 nonabsorbable suture. 9
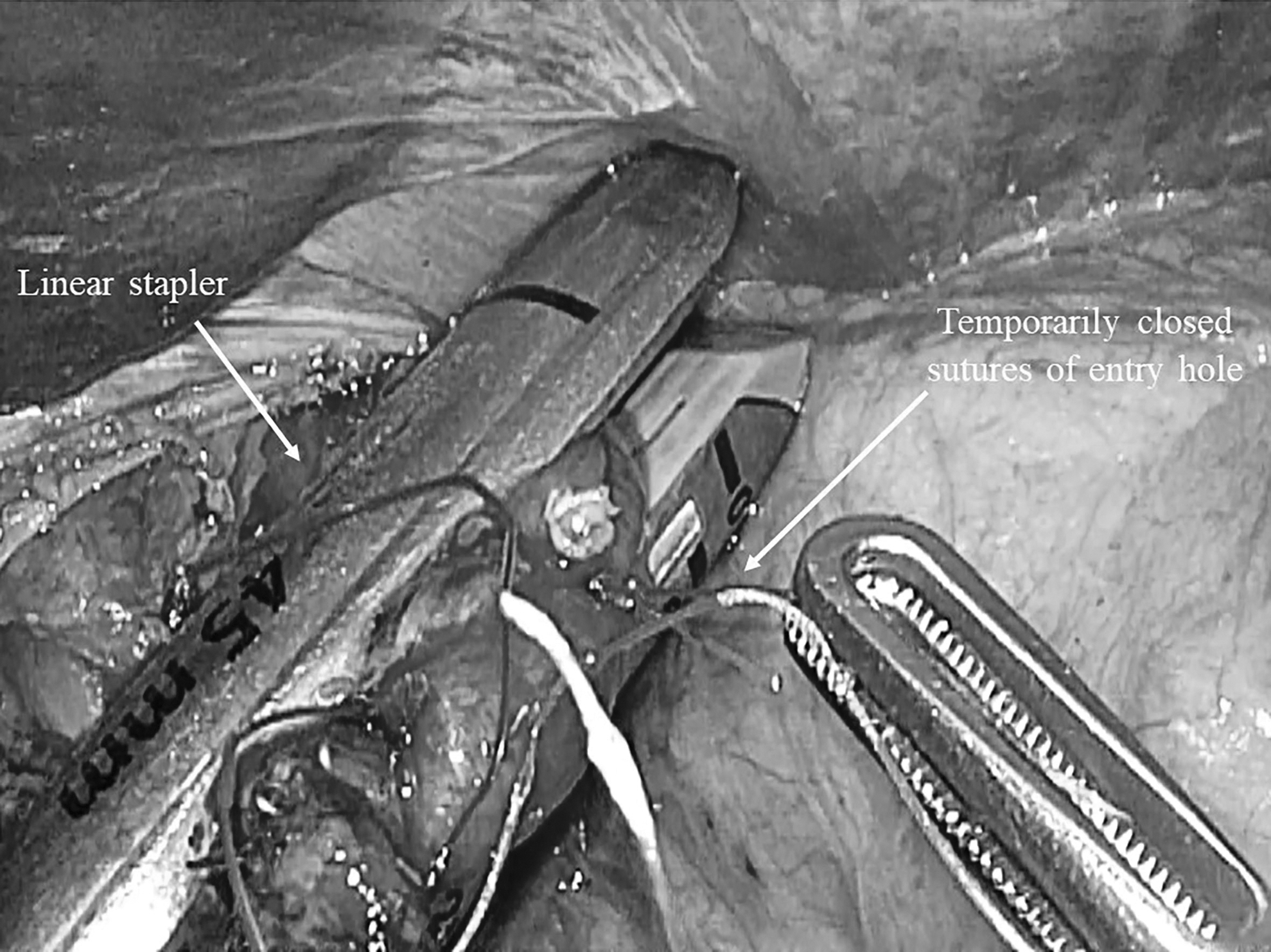
The insertion hole was temporarily closed by several hand-sewn sutures in full-thickness. Subsequently, the thread was pulled toward the ventral side to fire the linear stapler.
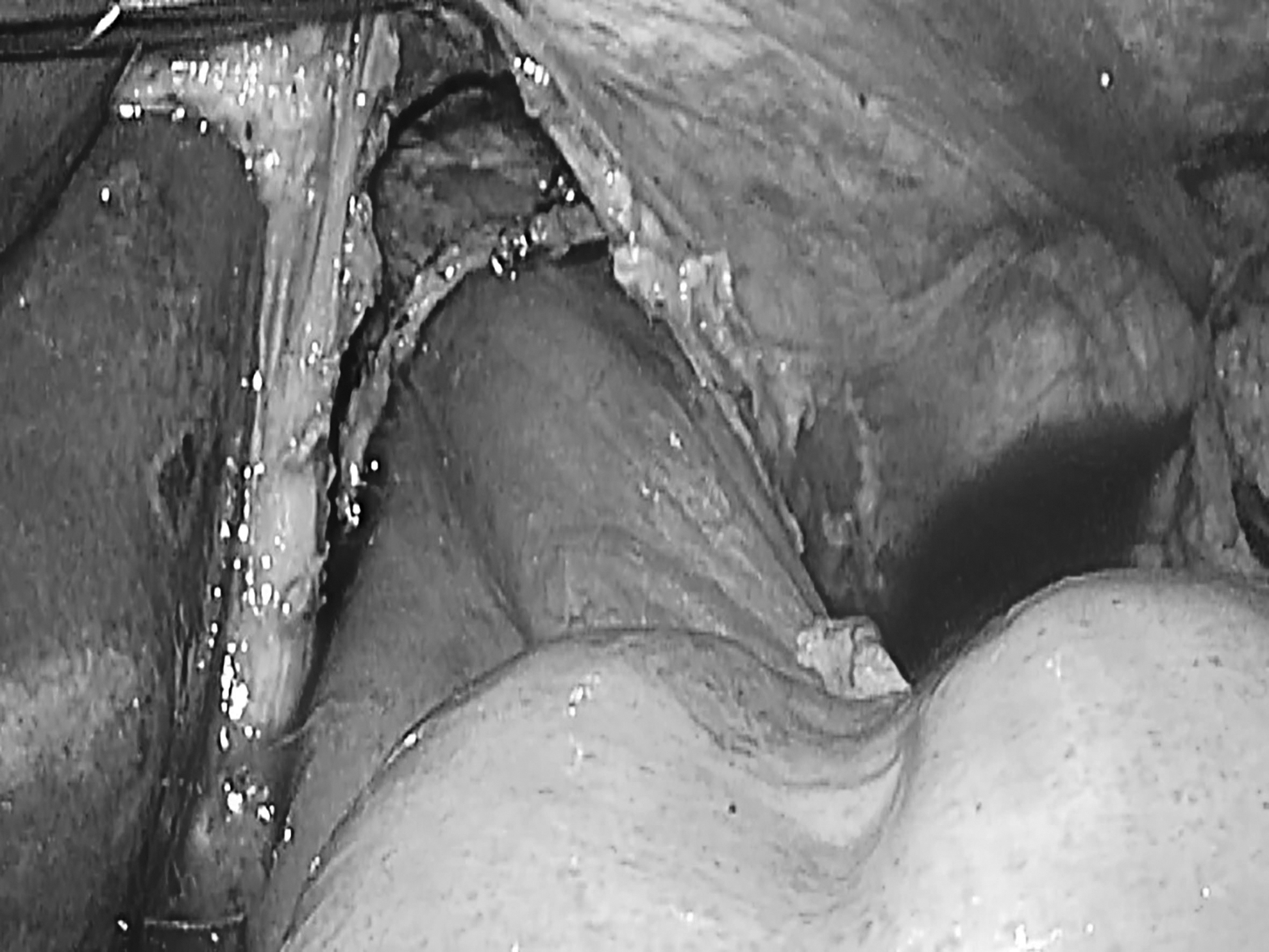
Completion of overlap esophagojejunostomy using linear stapler.
Results
We used this technique on 11 patients (9 men and 2 women) who underwent Roux-en-Y reconstruction (Table 1). 10 All the patients had a preoperative histological diagnosis of gastric cancer, and their ages ranged from 67 to 81 years, with a median of 74 years. This procedure was completed without any intraoperative or postoperative anastomotic leakage, stenosis, or bleeding complications (Table 2). 11
Patient Demographics
Pathological stage was classified according to the Japanese Classification of Gastric Carcinoma, 3rd English Edition. 10
EGJ, esophagogastric junction; proximal, laparoscopic proximal gastrectomy; proximal+lower, laparoscopic transhiatal proximal gastrectomy with lower esophagectomy; total, laparoscopic total gastrectomy; U, upper third; UM, upper-middle; UML, upper-middle-lower.
Surgical Outcomes
Morbidity is indicated by Clavien-Dindo classification grade ≥2. 11
All patients tolerated normal meals easily and were discharged after a successful recovery. The median follow-up period was 95 days (range = 28–232 days). During the follow-up period, none of the patients developed complications related to the esophagojejunostomy.
Discussion
Esophagojejunostomy methods are divided into side-to-side anastomosis using a linear stapler and end-side anastomosis using a circular stapler.12,13 Owing to the difficulty in manipulating the circular stapler in laparoscopic surgery, the number of facilities using linear staplers is increasing. 14 Linear stapler anastomosis methods are primarily divided into functional end-to-end anastomosis and overlap anastomosis. Several facilities perform overlapping anastomosis with relatively good jejunal elevation.8,15 However, it is difficult to close the insertion holes of the cartridge and anvil forks in overlap anastomosis, and misinsertion of the anvil fork into the submucosal layer of the esophagus is also an intraoperative complication. 7 Insertion holes can be hand-sewn or closed with linear stapler.16–18
The esophagus is transected anteriorly and posteriorly in both methods. The anvil fork insertion hole is created at the edge on the posterior wall side because insertion holes facing the ventral side are easier to close. 19 We present a novel method of overlap esophagojejunostomy using a linear stapler following LTG and LPG.
The following factors were considered for side-to-side anastomosis: (1) no perforation of the esophageal and jejunal walls with an anvil fork or a cartridge fork, (2) no accidental involvement of the diaphragmatic leg with a linear stapler, (3) no accidental involvement of the NGT with a linear stapler, (4) no injury to the esophageal wall due to strong traction of the esophageal stump, (5) the axes of the esophagus and the elevated jejunum were aligned, (6) no misinsertion of the anvil fork into the submucosal layer of the esophagus, (7) no accidental involvement of other organs such as the greater omentum or transverse colon, and (8) no gap between the esophageal and jejunal walls in side-to-side anastomosis of overlap esophagojejunostomy. The difficulty of esophagojejunostomy varies greatly between surgical cases, and the physique and height of the esophageal transection line of the patient highly influence it.
Points (1) to (4) could be addressed by the surgeon and the assistant collaborating to gently manipulate the instrument, paying close attention to the axes of the intestinal tract and the stapler in the optimal surgical field. Points (6) to (8) could be addressed by applying the new method described in this study. Simply guiding the NGT into the abdominal cavity from the entry hole of the esophageal stump and inserting an anvil fork into the esophageal lumen along the NGT could not completely prevent the misinsertion into the esophageal submucosal layer. Further, enlarging the insertion hole into the esophagus makes it easier to recognize the lumen of the esophagus and reduces the risk of misinsertion, making insertion hole closure more difficult.16–18,20
The esophageal insertion hole should be as small as possible, and the cartridge should not be misinserted.7,21 One suture was placed on each anterior and posterior wall to prevent the anvil fork from being misinserted into the esophageal submucosal layer. The assistant could support the anastomosis with two forceps. However, because the surgeon used his right hand to operate the linear stapler, he could only use his left hand to operate the forceps. Therefore, there were insufficient forceps to align the axes of the esophagus and the elevated jejunum to gently pull the esophagus to the caudal side and close the insertion hole gap. 15 The full-thickness suture on the posterior wall of the insertion hole was guided from the port, where the linear stapler was inserted into the outside of the abdominal cavity using this method.
Hence, the gap between the esophageal and jejunal walls in side-to-side anastomosis of overlap esophagojejunostomy was easily eliminated by pulling this thread toward the operator from the port. Moreover, while maintaining suture traction, the forceps on the left hand of the operator should be used to spread the surgical field so that the greater omentum and transverse colon are not accidentally involved in the anastomosis. In addition, because the thread and stapler were towed from the same port, the axis did not shift, and no intestinal perforation occurred. Closing the gap was also possible to weaken the traction to the caudal side of the esophagus. This novel method required no additional equipment and allowed for safer and more reliable suturing by leaving and pulling the full-thickness suture.
Different insertion forks are used depending on the type of stapler. For the Powered Echelon Flex® (Ethicon Endo-Surgery, Tokyo) stapler, the tissue is pulled toward the operator upon the cartridge fork closure. 22 Therefore, a cartridge fork was inserted into the esophagus to close the gap between the esophageal and jejunum holes. In addition, because the cartridge fork should not be opened and the esophageal longitudinal axis and the axis of the stapler match, inserting the cartridge fork into the esophageal side is recommended. However, since the cartridge fork was inserted into the esophagus, the linear stapler insertion hole grew and became difficult to close. In contrast, the Signia™ Stapling System (Covidien Japan, Tokyo) does not have a mechanism to pull in the tissue. 23
Since the anvil fork does not open, it could be inserted into the esophageal side where the longitudinal axis of the esophagus and the axis of the anvil fork match. Further, because the cartridge fork to be opened is inserted into the elevated jejunum, the blunt tip of the stapler is less likely to injure the jejunum. The linear stapler insertion hole shrinks and becomes easier to close as the anvil fork is inserted into the esophagus. These two examples highlight the importance of being familiar with the characteristics of the equipment.
This method made esophagojejunostomy easier and more stable; nonetheless, it requires careful interpretation. First, the number of cases was small, and they all had a short postoperative follow-up period. Moreover, the incidence of short- and long-term anastomosis-related outcomes of this technique and the conventional method where traction thread is not used has not been compared.
Reconstruction with LTG is difficult; therefore, it is important to master the procedure and avoid intraoperative complications. The most important guideline for avoiding complications is an early prediction of these events. In addition, since surgeons may be preoccupied with the surgical procedures during the operation, creating an environment conducive to discussion and sharing crisis management experience among surgical staff is essential.
This novel method using a linear stapler allowed easier and more stable esophagojejunostomy. However, it was only applied to a limited number of patients. We will apply this method in future cases and evaluate both its short- and long-term outcomes, including stenosis.
Data Availability Statement
This article is available online as a preprint and the link is available here: https://www.researchsquare.com/article/rs-2047580/v2
Consent for Publication
Patients signed informed consent regarding publishing their data.
Footnotes
Authors' Contributions
N.H. was the lead author and conceived this study. T.M., H.H., S.T., R.H., T.Y., and T.T. collected data and performed analysis. Y.T. reviewed the article. All authors read and approved the final article.
Disclosure Statement
N.H., T.M., H.H., S.T., R.H., T.Y., T.T., and Y.T. have no conflicts of interest or financial ties to disclose.
Funding Information
This study received no external sources of funding.