
Abstract
Background:
Complications frequently occur after neonatal enterostomy. Enterostomy formation is a common outcome following an emergency neonatal laparotomy. This study investigated whether the incidence of complications after enterostomy could be decreased with a drainage device (composed of foreskin cerclage staple, a condom, and a 0-Mersilk braided nonabsorbable suture) fixed in the proximal ostomy bowel tube to improve proximal enterostomy in newborns.
Methods:
This study was a retrospective case note review of the incidence of emergency neonatal enterostomy incidence over a 3-year period (2/2016–2/2019) at the authors’ center. A single surgeon conducted all surgeries. The incidence of intraoperative and postoperative complications was compared between modified and traditional surgery groups.
Results:
All 47 surgeries were successfully completed (32 boys and 15 girls; sex ratio: 2.13:1). The mean (±SD) birth weight, gestational period, and daily age were 2.64 ± 0.81 kg 35.62 ± 3.76 weeks and 3.49 ± 5.61 days, respectively. The patients were divided into modified surgery groups (20 cases) and traditional surgery groups (27 cases). The modified surgery group had significantly lower rates of total complications, unplanned reoperations, wound-related complications, and stoma-related complications than the traditional group (p <0.05).
Conclusions:
The preliminary observations suggested that the simple drainage device was a safe and effective operation device that reduced the risk of stoma-related complications.
Introduction
Enterostomy is important in treating several severe neonatal gastrointestinal diseases. Enterostomy improves survival rates among extremely low-birth-weight infants and infants with meconium obstruction of prematurity, spontaneous intestinal perforation (SIP), congenital anorectal malformations (ARMs), congenital intestinal atresia (CIA), necrotizing enterocolitis (NEC), or severe gastrointestinal malformation to the greatest extent possible and stabilizes infants for further treatment.1–3 Early management of such infants is critical and lifesaving. However, enterostomy is subjected to risks. For example, stoma-related complications (incision hernia, intestinal prolapse, perioral dermatitis, and surgical site infection4–6 ) frequently occur after neonatal enterostomy and can seriously endanger the newborn’s life. All of these complications are related to the early leakage of ostomy fluid or high-output ileostomy, where the seeping intestinal fluid can corrode the local skin and wounds and cause infection. This study describes a modified neonatal enterostomy procedure involving a simple drainage device to prevent complications by isolating the ostomy from the surrounding tissue and draining it to a safe area outside the wound. Herein, we report our operative experience.
Patients and Methods
This retrospective study was approved by the Dongguan Maternal and Child Health Hospital Ethics Committee. The hospital registry was retrospectively reviewed for infants who had undergone neonatal enterostomy at the center between February 2016 and February 2019 (47 cases). The patients were divided into modified surgery groups (20 cases) and traditional surgery groups (27 cases). A single surgeon had performed all surgeries. The modified surgery group was treated with “a simple drainage device for neonatal enterostomy”. The present study involved 32 boys and 15 girls. The patient demographics, clinical features, operative time, enterostomy complications, hospital stay, and outcomes were investigated.
Operative procedure
The traditional surgery group underwent conventional single- or double-lumen enterostomy. The modified surgery group featured the addition of a simple drainage device on the proximal enterostomy.
The simple drainage device consisted of a foreskin cerclage staple (Chong Qing BORN Biological Technology Co. Ltd., Sichuan, China), a condom, and a 0-Mersilk silk braided nonabsorbable suture (ETHICON 15 × 60 cm) (Fig. 1A). The condom was fixed to the foreskin ring with the 0-Mersilk silk braided nonabsorbable sutures (Fig. 1B). The inner diameter of the proximal stoma intestinal tube was measured before the device was constructed and a foreskin ring suitable for the intestinal tube inner diameter was selected. The lubricant was removed from the membrane, and a notch was cut out at the end of the membrane (Fig. 1C and D
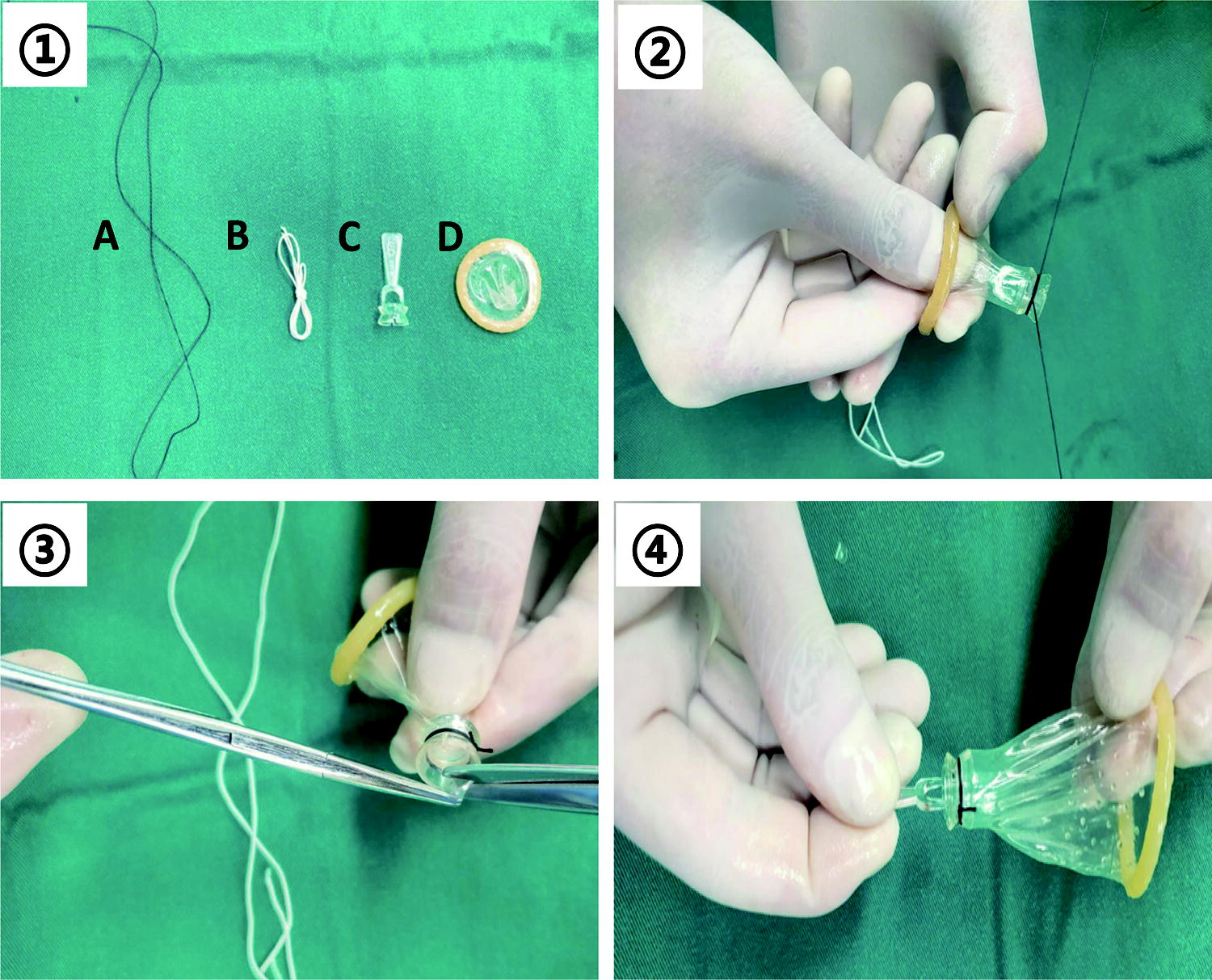
The prepuce ring was inserted into the stoma tube and secured to the proximal tube using elastic thread. The handle on the wrapping ring was broken, and the end of the condom was fastened with the small clip. A latex finger sleeve was placed over the small clip and secured with a rubber band to prevent the metal clip from harming the infant's skin (Figs. 2 and 3). All abdominal wall layers were closed using the in-dwelling abdominal drainage tube, and the exposed intestinal tube stoma was covered with Vaseline gauze. In cases where the child had a double-chamber stoma, the distal orifice was constructed 5–8 cm from the proximal orifice to allow it to fit the artificial pocket.

Representative photograph of a patient with tube stoma. The device uses a condom as a cannula, thus avoiding corrosion of the open tract by the proximal intestinal duct.

Wound condition at 5 days after the enterostomy.
Results
A single surgeon performed all surgeries. Assessment of the infants’ attributes revealed that their mean birth weight and age were 2.64 ± 0.81 kg, and 4.80 ± 1.6 days, respectively. This study included 32 male patients and 15 female patients (male:female ratio: 2.13:1). The gestational age, birth weight, and weight at surgery were not significantly different between the two surgery groups (Table 1).
Patients’ Details at Birth and Time of Laparotomy Where Stomas Were Created
Mann–Whitney test used for comparison between groups. IQR, interquartile range.
In the modified surgery group, eight patients were diagnosed with ARMs, six with NEC, and three with SIP requiring laparotomy. Additionally, the modified surgery group contained one patient each with CIA, IIH, and HD (Fig. 4). Furthermore, the modified surgery group involved nine double-lumen stomas, 10 single-chamber stomas, and one Bishop-Koop intestinal anastomosis. The mean surgical duration was 88.30 ± 16.75 minutes. The modified surgery group had a slightly longer operation duration than the traditional surgery group (86.07 ± 17.27 minutes, but was not significantly different (p > 0.05). The rates of total complications, unplanned reoperation, wound-related complications, and stoma-related complications were significantly different between the two groups (p <0.05) (Table 2). The group with stomas sited through a drainage device appeared to have a reduced likelihood of complications requiring further surgical intervention.
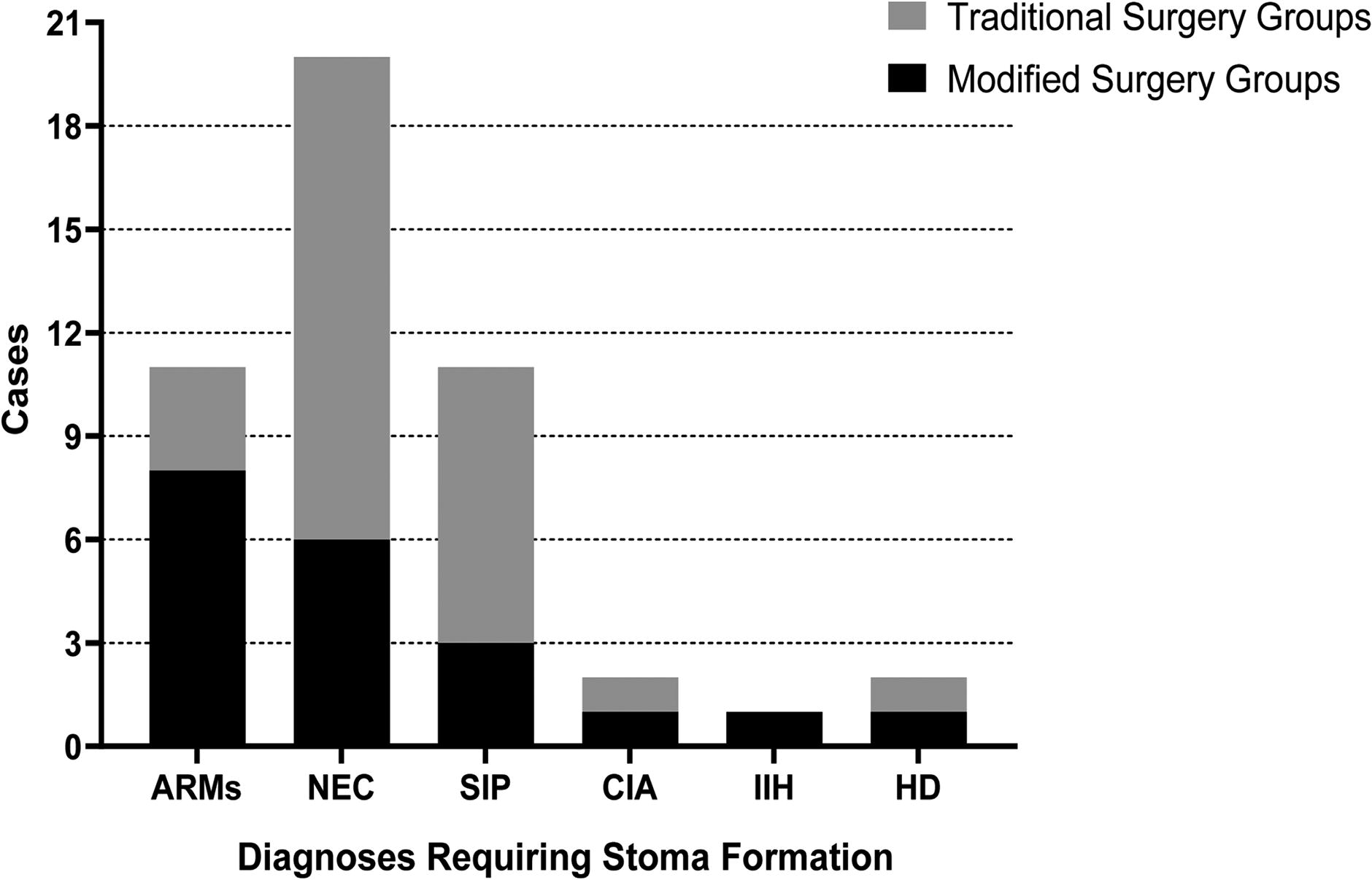
Diagnoses requiring stoma formation.
Complications in Each Group
Difference between groups compared using Chi-squared unless single values were less than five, where Fisher’s exact test was used.
The patients were fed 5% glucose 5–7 days after the operation, and the foreskin ring that was fixed to the proximal intestinal tube was removed 6–7 days after the operation. The abnormal drainage tube was removed if the abdominal color Doppler examination to assess abdominal fluid detected no abnormalities. The sutures on the abdominal wall wound were removed 7–9 days postoperatively. The average duration of postsurgery hospitalization in the modified surgery group was 20.05 ± 4.47 days, which was significantly shorter compared with that of the traditional surgery group (25.52 ± 12.06 days). Follow-up evaluations were conducted 3–6 months after discharge, and subsequent surgical interventions were performed based on re-evaluation. Only one case of intestinal prolapse occurred in the modified surgery group.
Discussion
Neonatal enterostomy is commonly employed in pediatric patients presenting with a critical acute abdomen. Most of these stomas are temporary, encompassing techniques such as loop enterostomy, double-barrel enterostomy, exteriorization, and single-port surgeries. 5 The primary objective of neonatal enterostomy is to facilitate defecation through the proximal enterostomy, alleviate intestinal pressure, manage infection, and stabilize infants for subsequent therapeutic interventions. Nevertheless, this therapeutic approach is subject to drawbacks, as it is associated with notable complications that include postoperative incision infection, incisional hernia, inflammation in the surrounding area, and intestinal prolapse.
Some complications tend to occur long after surgery. Incision infection and surrounding inflammation are the two most common complications, for the following reasons: (1) the stoma and wound positions are too close and (2) the distance from the ligament of Treitz influences peristomal dermatitis.7,8 A higher stoma position is accompanied by more alkaline intestinal fluid, which promotes the development of skin disorders. Peripheral dermatitis and incision infection account for >50% of all complications,5,9,10 which seriously endanger the infants’ health and life. Furthermore, the incidence of postoperative SSI is 0.7%–16.6%, which could directly lead to prolonged hospitalization and increase the risk of death.11,12
Given the numerous complications linked to exposure to intestinal fluid, the present inquiry focused on the feasibility of entirely isolating the intestinal fluid from the wound. The authors’ inspiration stemmed from the principles underlying circumcision procedures, which involve the gradual severing of elastic lines and subsequent shedding of the circumcision ring. This process ultimately leads to the formation of a standardized incision that facilitates healing.13–16 Accordingly, the authors assembled a simple intestinal ostomy drainage device with a foreskin cerclage staple, elastic thread a condom, and mousse thread. The foreskin ring was fixed on the stomata with an elastic line and automatically fell off 5–7 days after the operation. During this period, the stoma fluid was drained to the area outside the wound through the condom, which was completely isolated from the surgical incision, thus effectively preventing complications such as wound infection, incisional hernia, and peripheral dermatitis.
In this study, one patient died of multiple organ failure because of postoperative septic shock, and one patient underwent stoma surgery before the procedure because of excessive orifice wear and excessive intestinal fluid flow. The remaining patients experienced no obvious complications. In clinical patients, the authors determined that the enterostomy drainage device had the following advantages: (1) The surgical incision could be effectively isolated and the healing time is adequate; (2) delayed shedding of the wrapping ring prevented the need to replace the artificial pocket, not only decreasing medical costs but also reducing the nursing workload; (3) the transparency of the condom enabled observation of the intestinal fluid and exhaust characteristics, facilitating nursing; and (4) circumcision-style detachment allowed the formation of a more regularly shaped intestinal tube, which was conducive to pocket closure.
Owing to the inherent complexity of neonatal enterostomy, the approach frequently necessitates the expertise of seasoned medical practitioners. However, the authors’ proposed approach streamlines ostomy tubes, management, rendering it a straightforward and easily attainable skill, even for novice surgeons. The surgical techniques employed can be summarized as follows: (1) An appropriate foreskin ring should be chosen according to the intestinal tube diameter; typically the circumcision ring diameter should be slightly smaller than the intestinal tube diameter; (2) the condom used should be colorless and transparent, and thus convenient for postoperative observation; (3) an elastic line must be used rather than a mousseline, and the line knot must not be too tight. A line knot that is too tight can easily cause the prepuce ring to fall off prematurely, and thus impede effective wound isolation; (4) the exposed orifice tube should be 2–3 cm long, where a longer length can cause intestinal tube prolapse; and (5) the orifice tube should be wrapped with Vaseline gauze after the operation to avoid excessive drying and to protect the intestinal tube from mechanical damage.
Although the present study included a small number of patients, periostomy dermatitis occurred in only one patient (incidence rate: 5.26%), suggesting the effectiveness of the procedure. The authors believe that this method has no significant effect on long-term complications such as intestinal prolapse and improvement of stoma flow. However, whether it improves the incidence of intestinal prolapse and other complications requires confirmation by multicenter and larger sample studies. Furthermore, the alterations in the patient's condition result in a higher potential for NEC to contribute to postoperative complications. Nevertheless, the present study requires thorough examination and validation.
Conclusion
Our modified technique using ‘‘a simple drainage device’’ avoids complications and is safe and effective for use in infants. The follow-up results revealed that the operation method was effective and safe. We determined that our modification would be more affordable, have a lower postoperative complication rate, and be more popular with nursing staff.
Footnotes
Acknowledgments
This work was supported by the grants from Guangdong Provincial Medical Science and Technology Research Fund project (No. B2023296).
Authors’ Contributions
K.W. and J.C, analyzed the data and wrote the article; X.W.L. and G.M.Z. helped to design the study; G.Q.W. performed the surgeries and contributed significantly to the analysis and article preparation; J.K.Y. and G.Q.W. helped to perform the analysis with constructive discussions. All the authors reviewed the article.
Disclosure Statement
K.W., J.C., J.K.Y., X.W.L., G.M.Z., and G.Q.W. have no conflicts of interest or financial ties to disclose.
Disclaimer
The funders had no role in designing the study, collecting or analyzing the data, deciding to publish, or preparing the article.
Funding Information
Open access funding was provided by the grants from Guangdong Provincial Medical Science and Technology Research Fund project (No. B2023296).