
Abstract
Background:
A preliminary analysis from the COVID-Advanced Gastrointestinal Cancer Surgical Treatment (AGICT) study showed that the rate of minimally invasive surgery (MIS) for elective and urgent procedures did not decrease during the pandemic year. In this article, we aimed to perform a subgroup analysis using data from the COVID-AGICT study to evaluate the trend of MIS during the COVID-19 pandemic period in Italy.
Methods:
This study was conducted collecting data of MIS patients from the COVID-AGICT database. The primary endpoint was to demonstrate whether the SARS-CoV-2 pandemic scenario reduced MIS for elective treatment of gastrointestinal cancer (GIC) in Italy in 2020. The secondary endpoint was to evaluate the impact of the pandemic period on perioperative outcomes in the MIS group.
Results:
In the pandemic year, 62% of patients underwent surgery with a minimally invasive approach, compared to 63% in 2019 (P = .23). In 2020, the proportion of patients undergoing elective MIS decreased compared to the previous year (80% versus 82%, P = .04), and the rate of urgent MIS did not differ between the 2 years (31% and 33% in 2019 and 2020 - P = .66). Colorectal cancer was less likely to be treated with MIS approach during 2020 (78% versus 75%, P < .001). Conversely, the rate of MIS pancreatic resection was higher in 2020 (28% versus 22%, P < .002). Conversion to an open approach was lower in 2020 (7.2% versus 9.2% - P = .01). Major postoperative complications were similar in both years (11% versus 11%, P = .9).
Conclusion:
In conclusion, although MIS for elective treatment of GIC in Italy was reduced during the COVID-19 pandemic period, our study revealed that the overall proportion of MIS (elective and urgent) and postoperative outcomes were comparable to the prepandemic period. ClinicalTrial.gov (NCT04686747)
Introduction
During the early phase of the COVID-19 pandemic, feasibility and safety of minimally invasive surgery (MIS) was debated and discouraged to minimize the risk of inhalation of the surgical plume.1–4 We conducted a multicentric Italian study to evaluate the impact of the COVID-19 pandemic on perioperative outcomes in more than 8000 patients undergoing surgery for gastroesophageal, pancreatic, and colorectal cancer in 2019 and 2020. 5
Overall, a preliminary analysis of the COVID-Advanced Gastrointestinal Cancer Surgical Treatment (AGICT) study showed that the rate of MIS for elective and urgent procedures did not decrease during the pandemic year compared to the previous one (63% versus 62%, P = .23). In this article, we aimed to perform a subgroup analysis using data from the COVID-AGICT study to evaluate the trend of MIS during the COVID-19 pandemic period in Italy.
Methods
Ethical Statement
The COVID-AGICT study was approved by the ethics committee of the coordinating center (reference number 18886).
This study was conducted collecting data of MIS patients from the COVID-AGICT database. It was an Italian multicentric retrospective cohort study, including adult patients who underwent surgery for colorectal, gastroesophageal, and pancreatic cancer in 62 Italian surgical services from January 2019 to December 2020. Laparoscopic, robotic, and transanal total mesorectal excision approaches were included in the minimally invasive group (MIS).
Demographic data (age, sex, body mass index [BMI], ASA, Charlson Comorbidity Index [CCI] score), perioperative outcomes (e.g., proportion of elective and urgent MIS in the 2 years, and for each cancer group, conversion rate), and early postoperative outcomes (i.e., length of hospital stay- LOS, major postoperative complications, 30 days readmission, and 30 day mortality rate) were used to compare the MIS groups in 2019 and 2020.
The primary endpoint was to demonstrate whether the SARS-CoV-2 pandemic scenario reduced MIS for elective treatment of gastrointestinal cancer (GIC) in Italy in 2020. The secondary endpoint was to evaluate the impact of the pandemic period on perioperative outcomes in the MIS group. This article was written according to the STrengthening the Reporting of Observational Studies in Epidemiology checklist. 6
Statistical analysis
Quantitative variables included in the study are presented as mean ± standard deviation at the general level and divided by year. Qualitative (categorical) variables are represented as percentages and absolute values, both at a general level and divided by year. Quantitative variables of interest were compared using two-tailed Student's t-test (in case of heteroskedasticity of variances). A comparison between qualitative variables of interest was carried out to evaluate the association among them through an extension of the chi-square test, suitable for multicentric studies (the Cochran–Mantel–Haenszel test). A ≤ 0.05 P-value was considered statistically significant. Missing data were excluded listwise, which could have affected some numerical discrepancies in the calculation of frequencies.
Since the majority of outcomes were provided for about 75%–100% of patients, after data aggregation and before the analysis, patients with more than 25% of missing data of a specific outcome were excluded from the analysis of the single outcome. Moreover, we reported the rate of patients with available data for any outcomes.
Results
Overall, the COVID-AGICT study enrolled 8250 patients, of whom 4370 (53%) and 3880 (47%) underwent surgery in 2019 and 2020, respectively. Of these, 730 (9%) patients underwent surgery for gastroesophageal cancer, 1816 (22%) for pancreatic cancer and 5704 (69%) for colorectal cancer. Over the 2 years, 62% of patients had surgery with MIS (5145 of 8250 patients).
Primary outcome
In the pandemic year, 62% of patients underwent surgery with a minimally invasive approach, compared to 63% in 2019 (Table 1). This difference was not statistically different (P = .23%–99% of patients with available data). In 2020, the proportion of patients undergoing elective MIS decreased compared to the previous year, and this difference was statistically significant (80% versus 82%, P = .04%–99% of patients with available data). The rate of urgent MIS did not differ between the 2 years: 31% and 33% in 2019 and 2020, respectively (P = .66%–100% of patients with available data) (Fig. 1).
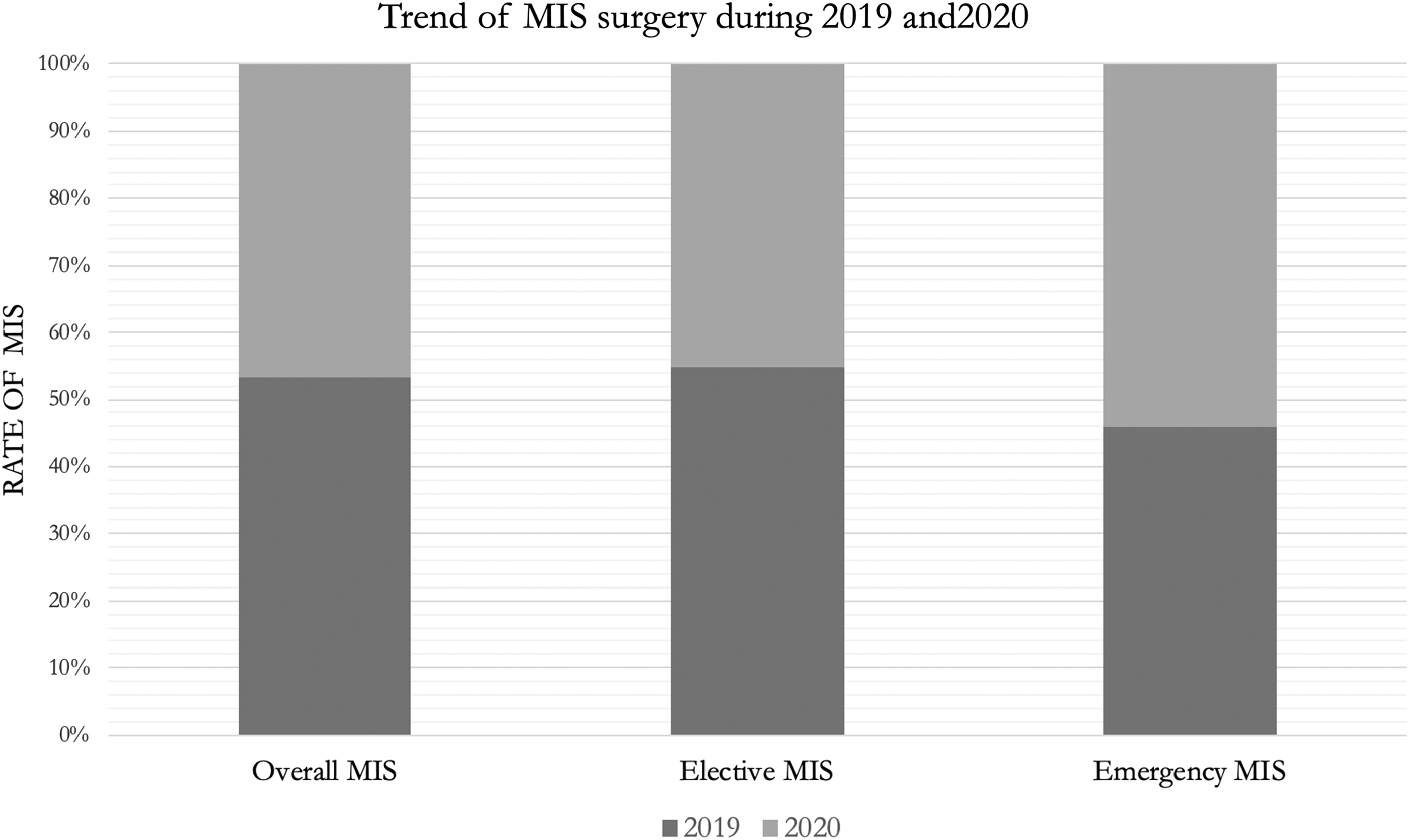
Trend of MIS during 2019 and 2020. MIS, minimally invasive surgery.
Main Outcomes
mean ± standard deviation.
In italic is represented the p value. In bold italic when p value was < .05, when the difference was statistically significative.
ASA, American Society of Anesthesiologists; BMI, body mass index; CCI, Charlson Comorbidity Index; CR, colorectal; GE, gastroesophageal; MIS, minimally invasive surgery; Pan, pancreatic.
Secondary outcomes
Demographic data showed no differences in mean age, sex, mean BMI, preoperative ASA score, and CCI score between the two groups.
The MIS trend in the different cancer groups showed that patients in the colorectal group were less likely to be treated with a minimally invasive approach during the pandemic year compared to the previous year (78% versus 75%, P < .001%–99% of patients with available data). Interestingly, the rate of MIS pancreatic resection was higher in 2020 compared with the year before (28% versus 22%, P < .002%–99% of patients with available data). Conversely, there was no difference in MIS between the 2 years for gastroesophageal cancer groups.
The rate of curative and palliative procedures performed with a minimally invasive approach was similar over the 2 years with no statistical difference (P > .05%–85% of patients with available data).
Conversion to an open approach was lower in 2020 compared to 2019 (7.2% versus 9.2%), and this difference was statistically significant (P = .01%–94% of patients with available data). To better assess these findings, we analyzed the subgroup of patients with colorectal cancer, as this was the most common cancer included in the study. Conversion rate was significantly lower in the pandemic year than in 2019 (6.9% versus 8.7%, P = .03%–93% of patients with available data).
Mean LOS (9.7 ± 2.8 versus 9.6 ± 1.4 days, P = .7%–99% of patients with available data) and major postoperative complications (grade III–V, according to the Clavien-Dindo classification system 7 ) were similar in both years (11% versus 11%, P = .9%–99% of patients with available data). Similarly, the 30-day readmission rate (2.7% versus 3.2%; P = .3) and the 30-day mortality rate were comparable in 2020 and 2019 (1.9 versus 2.5, P = .09).
Discussion
Overall, the results of our study showed that the rate of MIS for GIC treatment (urgent and elective surgery) did not decrease in 2020 in Italy. However, if we consider elective surgery alone, the proportion of patients undergoing MIS in 2020 decreased significantly compared to 2019, whereas MIS for urgent surgery was comparable in both years. Subgroup analysis showed a significant reduction in MIS for the colorectal cancer (CRC) group and a significant increase of MIS pancreatic cancer group during the 2020, without no significant difference for gastroesophageal cancers. In addition, this study showed that the conversion rate to open surgery was significantly reduced in 2020, as confirmed in the CRC subgroup.
To minimize the risk of inhalation of the surgical plume, the feasibility and safety of MIS was called into question, especially during the early phase of the COVID-19 pandemic.1–5 As a result, surgical practice changed significantly during the pandemic period, and the reduction of MIS for GIC treatment, although in accordance with COVID-19 guidelines, 1 was one of the most important aspects. At the same time, several measures were taken by the “international MIS community” to increase the level of awareness and prevention of possible transmission during surgery, as well as to provide the same standard of care for oncologic patients.
Some surgeons performed laparoscopy according to good surgical practice, such as avoiding abdominal desufflation without smoke evacuation. Others, based on the experience of expert MIS centers, introduced new rules or devices to improve the safety of the operating room staff.4,8–10 As a result, some expert Italian centers on MIS, showed that the rate of laparoscopic surgery was not affected by the pandemic period.4,11
The reduction in elective MIS in Italy, as shown by our study, could reflect both the consequence of the restrictions proposed by several guidelines and a consequence of elective surgical activity reduction.2,3,12,13 Better patient selection for MIS in 2020 may explain the lower conversion rate in the overall patient cohort and in the CRC subgroup. 12 However, these changes in surgical practice did not affect postoperative outcomes, which were comparable in both years.
The results of this study should be interpreted with caution because of its limitations, which should be acknowledged. First, it was retrospective in nature. Second, some data were not detailed and may have influenced the final results. Third, this study included five types of GICs: perioperative and postoperative outcomes could be influenced by the differences between these cancers. Finally, 69% of the patients included in our cohort had colorectal cancer, which may have influenced the final results.
Conclusion
In conclusion, although MIS for elective treatment of GIC in Italy was reduced during the COVID-19 pandemic period, the overall proportion of MIS (elective and urgent) and postoperative outcomes were comparable to the prepandemic period. To date, we are in a different era with vaccines and there is no clear evidence of transmission of viral particles through surgical smoke.2,3 These results should be considered in a future pandemic before changing our surgical practice to provide the same standard of care to our patients.
Footnotes
Acknowledgments
The study was preregistered without an analysis plan. This article reports the results of NCT04686747 preregistered studies, which can be accessed at ![]() . The COVID–AGICT study group is an Italian collaboration, hosted centrally from the Misericordia Hospital, Grosseto. MIS–COVID–AGICT collaborative group: Lucia Salvischiani, MD (Department of General and Emergency Surgery, Misericordia Hospital, Azienda Usl Toscana Sud Est. School of Robotic Surgery, Grosseto, Italy), Francesco Santelli, PhD (Department of Economics, Business, Mathematics and Statistics (DEAMS), University of Trieste, Trieste, Italy), Angelo Restivo, MD (Department of Surgery, Colorectal Surgery Center, University of Cagliari, Cagliari, Italy), Andrea Casaril, MD (Department of Surgery, “Pederzoli” Hospital, Peschiera del Garda, Verona, Italy), Gianluigi Moretto, MD (Department of Surgery, “Pederzoli” Hospital, Peschiera del Garda, Verona, Italy).
. The COVID–AGICT study group is an Italian collaboration, hosted centrally from the Misericordia Hospital, Grosseto. MIS–COVID–AGICT collaborative group: Lucia Salvischiani, MD (Department of General and Emergency Surgery, Misericordia Hospital, Azienda Usl Toscana Sud Est. School of Robotic Surgery, Grosseto, Italy), Francesco Santelli, PhD (Department of Economics, Business, Mathematics and Statistics (DEAMS), University of Trieste, Trieste, Italy), Angelo Restivo, MD (Department of Surgery, Colorectal Surgery Center, University of Cagliari, Cagliari, Italy), Andrea Casaril, MD (Department of Surgery, “Pederzoli” Hospital, Peschiera del Garda, Verona, Italy), Gianluigi Moretto, MD (Department of Surgery, “Pederzoli” Hospital, Peschiera del Garda, Verona, Italy).
Antonio De Leo, MD (General Surgery Unit, Sandro Pertini Hospital, ASL Roma 2, Via dei Monti Tiburtini, 385, 00157, Rome, Italy), Marco Catarci, MD (General Surgery Unit, Sandro Pertini Hospital, ASL Roma 2, Via dei Monti Tiburtini, 385, 00157, Rome, Italy), and Renza Trapani, MD (Department of General Surgery, Ospedale San Biagio, ASL VCO, Domodossola, Italy).
Also, Sandro Zonta, MD (Department of General Surgery, Ospedale San Biagio, ASL VCO, Domodossola, Italy), Patrizia Marsanic, MD (Surgical Department, E. Agnelli Hospital, 10064 Pinerolo, Italy), Andrea Muratore, MD (Surgical Department, E. Agnelli Hospital, 10064 Pinerolo, Italy), Gregorio Di Franco, MD (General Surgery Unit, Department of Translational Research and New Technologies in Medicine and Surgery, University of Pisa, Via Paradisa 2, 56125, Pisa, Italy), Luca Morelli, MD (General Surgery Unit, Department of Translational Research and New Technologies in Medicine and Surgery, University of Pisa, Via Paradisa 2, 56125, Pisa, Italy), Alessandro Coppola, MD (Dipartimento di Chirurgia, Sapienza Università di Roma, Rome, Italy), and Damiano Caputo, MD (Research Unit of Generale Surgery, Department of Medicine and Surgery, University Campus Bio-Medico di Roma, Via Alvaro del Portillo 200, 00128 Rome, Italy; Operative Research Unit of General Surgery, Fondazione Policlinico Universitario Campus Bio-Medico, Via Alvaro del Portillo, 200, 00128 Roma, Italy).
Jacopo Andreuccetti, MD (Second General Surgery, ASST Spedali Civili di Brescia, Brescia, Italy), Giusto Pignata, MD (Second General Surgery, ASST Spedali Civili di Brescia, Brescia, Italy), Laura Mastrangelo, MD (Division of General and Emergency Surgery, IRCCS Azienda Ospedaliero-Universitaria di Bologna, Bologna, Italy), Elio Jovine, MD (Division of General and Emergency Surgery, IRCCS Azienda Ospedaliero-Universitaria di Bologna, Bologna, Italy), Michele Mazzola, MD (Division of Minimally Invasive Surgical Oncology, ASST Grande Ospedale Metropolitano Niguarda, Piazza Ospedale Maggiore, 3 20162 Milan, Italy), Giovanni Ferrari, MD (Division of Minimally Invasive Surgical Oncology, ASST Grande Ospedale Metropolitano Niguarda, Piazza Ospedale Maggiore, 3 20162 Milan, Italy), Lorenzo Mariani, MD (General Surgery, San Giovanni Battista Hospital, USL Umbria 2, Foligno, Italy), and Graziano Ceccarelli, MD (General Surgery, San Giovanni Battista Hospital, USL Umbria 2, Foligno, Italy).
Rocco Giuseppe, MD (Hepatobiliary, Pancreatic and General Surgery Unit, Department of Surgery, Azienda Unità Sanitaria Locale Area Vasta Romagna, Santa Maria delle Croci—Ravenna Hospital, Ravenna, Italy), Stefano Bolzon, MD (Hepatobiliary, Pancreatic and General Surgery Unit, Department of Surgery, Azienda Unità Sanitaria Locale Area Vasta Romagna, Santa Maria delle Croci—Ravenna Hospital, Ravenna, Italy), Mariateresa Grasso, MD (S.C. Chirurgia Generale, Ospedale S.Andrea, Vercelli, Italy), Silvio Testa, MD (S.C. Chirurgia Generale, Ospedale S.Andrea, Vercelli, Italy), Paola Germani, MD (Surgical Clinic Unit, University Hospital of Trieste, Trieste, Italy), Nicolò de Manzini, MD (Surgical Clinic Unit, University Hospital of Trieste, Trieste, Italy), Serena Langella, MD (Department of General and Oncological Surgery, Mauriziano Hospital, Largo Turati 62, 10128, Turin, Italy), and Alessandro Ferrero, MD (Department of General and Oncological Surgery, Mauriziano Hospital, Largo Turati 62, 10128, Turin, Italy).
Alfredo Genovese, MD (Department of General and Emergency Surgery, Misericordia Hospital, Azienda Usl Toscana Sud Est. School of Robotic Surgery, Grosseto, Italy), Dario Sirimarco, MD (Department of General and Emergency Surgery, Misericordia Hospital, Azienda Usl Toscana Sud Est. School of Robotic Surgery, Grosseto, Italy), Angela Tribuzi, MD (Department of General and Emergency Surgery, Misericordia Hospital, Azienda Usl Toscana Sud Est. School of Robotic Surgery, Grosseto, Italy), Martina Maruccio (Department of General and Pancreatic Surgery, The Pancreas Institute, University of Verona Hospital Trust, Piazzale L.A. Scuro, 10, 37134, Verona, Italy), Federico Faustini (Department of General and Pancreatic Surgery, The Pancreas Institute, University of Verona Hospital Trust, Piazzale L.A. Scuro, 10, 37134, Verona, Italy), Giorgio Lisi (Department of General Surgery, S. Eugenio Hospital, Piazzale dell'Umanesimo, 10, 00144, Rome, Italy), and Fabrizio Allisiardi (Department of General Surgery, S. Eugenio Hospital, Piazzale dell'Umanesimo, 10, 00144, Rome, Italy).
Michele Grieco (Department of General Surgery, S. Eugenio Hospital, Piazzale dell'Umanesimo, 10, 00144, Rome, Italy), Carolina Righetti, MD (Department of Surgery—General Surgery Unit, Hospital of Biella, Biella, Italy), Marco Frisini (APSS, Department of General Surgery & HPB Unit, Largo Medaglie d'oro 9, 38122, Trento, Italy), Alberto Brolese (APSS, Department of General Surgery & HPB Unit, Largo Medaglie d'oro 9, 38122, Trento, Italy), Michele Grassia (Division of Surgery, Ospedale “Ceccarini”, AUSL Romagna, Riccione, Italy), Andrea Lucchi (Division of Surgery, Ospedale “Ceccarini”, AUSL Romagna, Riccione, Italy), Giulia Bagaglini (University of Rome Tor Vergata, Department of Surgery, Rome, Italy), Giuseppe S Sica (University of Rome Tor Vergata, Department of Surgery, Rome, Italy), Michele Manara (Surgical Oncology Unit—Treviglio Hospital ASST Bergamo Ovest), and Luca Turati (Surgical Oncology Unit—Treviglio Hospital ASST Bergamo Ovest).
Lorenzo Macone (ASST Bergamo Est, P.O. Pesenti Fenaroli, General Surgery Unit, Alzano Lombardo, Bergamo, Italy), Roberta Carminati (ASST Bergamo Est, P.O. Pesenti Fenaroli, General Surgery Unit, Alzano Lombardo, Bergamo, Italy), Pierpaolo Mariani (ASST Bergamo Est, P.O. Pesenti Fenaroli, General Surgery Unit, Alzano Lombardo, Bergamo, Italy), Gianluca Rizzo (UOC Chirurgia dell'Apparato Digerente e del Colon-Retto Ospedale Fatebenefratelli Isola Tiberina—Gemelli Isola, Rome, Italy), Claudio Coco (U.O.C. Chirurgia Generale 2—Fondazione Policlinico Universitario Agostino Gemelli IRCCS; Università Cattolica del Sacro Cuore, Rome, Italy U.O.C. Radioterapia Oncologica—Fondazione Policlinico Universitario Agostino Gemelli IRCCS; Università Cattolica del Sacro Cuore, Rome, Italy), and Francesca Pennetti Pennella (Department of Surgical Specialties, SC General Surgery and Surgical Specialties, St Maria Hospital, Terni, Italy).
Fabio Rondelli (Department of Surgical Specialties, SC General Surgery and Surgical Specialties, St Maria Hospital, Terni, Italy), Lucia Romano (Department of Biotechnological and Applied Clinical Sciences, San Salvatore Hospital, Università Degli Studi dell'Aquila, L'Aquila, Italy), Antonio Giuliani (Department of Biotechnological and Applied Clinical Sciences, San Salvatore Hospital, Università Degli Studi dell'Aquila, L'Aquila, Italy), Raffaele Palaia (Department of Abdominal Oncology, Division of Gastro-esophageal and Pancreatic Surgical Oncology, Istituto Nazionale Tumori, Fondazione G. Pascale, IRCCS, Naples 80131, Italy), Andrea Belli (Department of Abdominal Oncology, Division of Gastro-esophageal and Pancreatic Surgical Oncology, Istituto Nazionale Tumori, Fondazione G. Pascale, IRCCS, Naples 80131, Italy), Vittorio Albino (Department of Abdominal Oncology, Division of Gastro-esophageal Surgical Oncology, Istituto Nazionale Tumori, Fondazione G. Pascale, IRCCS, Naples 80131, Italy), and Maddalena Leongito (Department of Abdominal Oncology, Division of Gastro-esophageal Surgical Oncology, Istituto Nazionale Tumori, Fondazione G. Pascale, IRCCS, Naples 80131, Italy).
Giulia David (Chirurgia Generale—Sant'Anna Como (San Fermo Della Battaglia) ASST-Lariana), Pasquale Misitano (Chirurgia Generale—Sant'Anna Como (San Fermo Della Battaglia) ASST-Lariana), Silvia Pasulo (Surgical Clinic, Department of Experimental and Clinical Sciences, University of Brescia, 25123 Brescia, Italy), Gian Luca Baiocchi (Surgical Clinic, Department of Experimental and Clinical Sciences, University of Brescia, 25123 Brescia, Italy), Roberta La Mendola (Hepato-Bilio-Pancreatic Minimally Invasive Surgery, Poliambulanza Foundation Hospital, Brescia, Italy), Mohamnad Abu Hilal (Hepato-Bilio-Pancreatic Minimally Invasive Surgery, Poliambulanza Foundation Hospital, Brescia, Italy).
Ludovica Baldari (Department of Surgery, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico di Milano, University of Milan, Milan, Italy), Elisa Cassinotti (Department of Surgery, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico di Milano, University of Milan, Milan, Italy), and Luigi Boni (Department of Surgery, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico di Milano, University of Milan, Milan, Italy).
Gabriella Teresa Capolupo (Colorectal Surgery Unit, Fondazione Policlinico Campus Bio-Medico, Università Campus Bio-Medico di Roma, Rome, Italy), Marco Caricato (Colorectal Surgery Unit, Fondazione Policlinico Campus Bio-Medico, Università Campus Bio-Medico di Roma, Rome, Italy), Enrico Pinotti (Department of Surgery, Ponte San Pietro Hospital, Bergamo, Italy), Mauro Montuori (Department of Surgery, Ponte San Pietro Hospital, Bergamo, Italy), Cristina Bombardini (Department of Surgery, Section of Chirurgia 1, Sant'Anna University Hospital of Ferrara, Cona, Italy), Gabriele Anania (Department of Surgery, Section of Chirurgia 1, Sant'Anna University Hospital of Ferrara, Cona, Italy), Rigers Dibra (Department of Emergency and Organ Transplantation, University “Aldo Moro” of Bari, Piazza G Cesare, 11, 70124, Bari, Italy), Gennaro Martines (Department of Emergency and Organ Transplantation, University “Aldo Moro” of Bari, Piazza G Cesare, 11, 70124, Bari, Italy).
Leonardo Solaini (Department of Medical and Surgical Sciences, University of Bologna, Morgagni-Pierantoni Hospital, Forlì, Italy), and Giorgio Ercolani (Department of Medical and Surgical Sciences, University of Bologna, Morgagni-Pierantoni Hospital, Forlì, Italy).
Renato Oliva (IRCCS Regina Elena National Cancer Institute, Rome, Italy), Maria Vittoria Carati (IRCCS Regina Elena National Cancer Institute, Rome, Italy), Gian Luca Grazi (IRCCS Regina Elena National Cancer Institute, Rome, Italy), Giacomo Ghio (Department of Surgical Oncology and Gastroenterology Sciences, First Surgical Clinic, University of Padua, Padua (PD), Italy), Francesco Marchegiani (Department of Surgical Oncology and Gastroenterology Sciences, First Surgical Clinic, University of Padua, Padua (PD), Italy), Salvatore Pucciarelli (Department of Surgical Oncology and Gastroenterology Sciences, First Surgical Clinic, University of Padua, Padua (PD), Italy), Filippo La Torre (Department of Surgical Sciences, Policlinico Umberto I University Hospital, Sapienza University of Rome, Rome, Italy), Immacolata Iannone (Department of Surgery, “Pietro Valdoni,” “Sapienza” University of Rome, Italy”), Dimitri Krizzuk (Unit of General Surgery—Aurelia Hospital, Rome, Italy), and Francesco Sammartino (Unit of General Surgery—Aurelia Hospital, Rome, Italy).
Nicola Cillara (Generale PO Santissima Trinità ASL Cagliari—Cagliari), Antonello Deserra, (Generale PO Santissima Trinità ASL Cagliari—Cagliari), and Alessandro Cannavera (Generale PO Santissima Trinità ASL Cagliari—Cagliari).
Giorgia Catalano (General Surgery 2U—Liver Transplant Unit, A.O.U. Città Della Salute e Della Scienza di Torino, University of Turin, Turin, Italy), Paolo Strignano (General Surgery 2U—Liver Transplant Unit, A.O.U. Città Della Salute e Della Scienza di Torino, University of Turin, Turin, Italy), Renato Romagnoli (General Surgery 2U—Liver Transplant Unit, A.O.U. Città Della Salute e Della Scienza di Torino, University of Turin, Turin, Italy), Domenico Piccione (General and Oncological Surgery Unit, Department of Surgery, Annunziata Hospital, Cosenza, Italy), Bruno Nardo (General and Oncological Surgery Unit, Department of Surgery, Annunziata Hospital, Cosenza, Italy), Rossella Reddavid (Division of Surgical Oncology and Digestive Surgery, Department of Oncology, San Luigi University Hospital, University of Turin, Turin, Italy), and Maurizio Degiuli (Division of Surgical Oncology and Digestive Surgery, Department of Oncology, San Luigi University Hospital, University of Turin, Turin, Italy).
Martino Gerosa (Laparoscopic and Oncological General Surgery Department, ASST Monza, Desio Hospital, Via Mazzini 1, Desio, Italy), Dario Maggioni (Laparoscopic and Oncological General Surgery Department, ASST Monza, Desio Hospital, Via Mazzini 1, Desio, Italy), Michele Zuolo (Department of General Surgery, Cles Hospital, Cles, Italy), Marco Rigamonti (Department of General Surgery, Cles Hospital, Cles, Italy), Omar Ghazouani (Department of Surgery, Santa Corona Hospital, Pietra Ligure, Italy), Raffaele Galleano (Department of Surgery, Santa Corona Hospital, Pietra Ligure, Italy), Andrea Percivale (Department of Surgery, Santa Corona Hospital, Pietra Ligure, Italy), Luca Tirloni (Division of Oncologic Surgery and Robotics, Department of Oncology, Careggi University Hospital, Florence, Italy), Luca Moraldi (Division of Oncologic Surgery and Robotics, Department of Oncology, Careggi University Hospital, Florence, Italy), and Nicolò Fabbri (Department of Surgery, Section of General Surgery, Ospedale del Delta, Azienda USL of Ferrara, University of Ferrara, Ferrara 44023, Italy).
Carlo Vittorio Feo (Department of Surgery, Section of General Surgery, Ospedale del Delta, Azienda USL of Ferrara, University of Ferrara, Ferrara 44023, Italy), Samuele Colombo (Department of General Surgery, Ospedale Civile “Madonna del Soccorso”, San Benedetto del Tronto, AP, Italy), Salomone Di Saverio (Department of General Surgery, Ospedale Civile “Madonna del Soccorso”, San Benedetto del Tronto, AP, Italy), Giuseppe Barbato (Digestive Surgery Unit, Department of Clinical and Experimental Medicine, Careggi University Hospital, Florence, Italy), Francesco Coratti (Digestive Surgery Unit, Department of Clinical and Experimental Medicine, Careggi University Hospital, Florence, Italy), Andrea Sagnotta (Department of General Surgery and Surgical Oncology, San Filippo Neri Hospital, Rome 00135, Italy), Stefano Mancini (Department of General Surgery and Surgical Oncology, San Filippo Neri Hospital, Rome 00135, Italy), and Luca Ferraro (Division of General and Robotic Surgery, Dipartimento di Scienze Della Salute, Università di Milano, ASST Santi Paolo e Carlo, 20142 Milano, Italy).
Giampaolo Formisano (Division of General and Robotic Surgery, Dipartimento di Scienze Della Salute, Università di Milano, ASST Santi Paolo e Carlo, 20142 Milano, Italy), Paolo Pietro Bianchi (Division of General and Robotic Surgery, Dipartimento di Scienze Della Salute, Università di Milano, ASST Santi Paolo e Carlo, 20142 Milano, Italy), Simona Messinese, MD (Medical Oncology Unit, Misericordia Hospital, Grosseto, Italy), Carmelo Bengala (Medical Oncology Unit, Misericordia Hospital, Grosseto, Italy), and Michele Di Marino (Department of General and Emergency Surgery, Misericordia Hospital, Azienda Usl Toscana Sud Est. School of Robotic Surgery, Grosseto, Italy).
Authors' Contributions
Concept and design: G.G., C.D., G.F. Acquisition, analysis, or interpretation of data: all authors. Drafting of the article: G.G., E.S. Critical revision of the article for important intellectual content: G.F., C.A. Statistical analysis: S.F., G.G. Supervision: C.A.
Disclaimer
G.G. had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Data will be made available upon reasonable request.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.