
Abstract
Background:
Complex ventral hernia remains a challenging situation for any surgeon. In this study, our aim was to analyze the effect of laparoscopic intraperitoneal onlay mesh (IPOM) repair in the treatment of complex abdominal wall hernia, with the assistance of preoperative progressive pneumoperitoneum (PPP) and botulinum toxin A (BTA).
Methods:
In this retrospective study, we included 13 patients with complex ventral hernia between May 2021 and December 2022. All patients undergoing PPP and BTA protocol before hernia repair. The length of abdominal wall muscles and abdominal circumference were measured from CT scan. All hernias were repaired with laparoscopic or laparoscopic-assisted IPOM.
Results:
Thirteen patients received PPP and BTA injections. PPP and BTA administration time was over 8.8 ± 2.5 days. Before and after PPP and BTA, imaging showed that the length of lateral muscle on each side increased from 14.3 to 17.4 cm (P < .05). The abdominal circumference increased from 81.8 to 87.9 cm (P < .05). Complete fascial closure was obtained in 13 patients (100%), and no patient experienced postoperative abdominal hypertension and ventilatory support. No patient suffered from recurrent hernia to date.
Conclusions:
Preoperative PPP combined with BTA injection plays a role similar to component separation technique, avoids the abdominal hypertension after laparoscopic IPOM repair of complex ventral hernia.
Introduction
Incisional hernia (IH) is a common complication after abdominal surgery, with a risk of undergone IH ranging from 5% to 20% as previously reported,1,2 and as high as 69.1% in some high-risk patients. 3 Despite rapid advances in surgical techniques and materials, it is difficult, if not impossible, to obtain ideal surgical repair of IH with lower recurrence and complications. 4 Some hernias gradually evolved into complex ventral hernias, particularly those with large chronic defects with loss of domain, are a huge challenge. 5 In patients with complex abdominal hernia, lateral muscle retraction leads to smaller abdominal volume, which can easily lead to the abdominal hypertension postoperatively. 6 Hence, in these patients, careful preparation before surgery is vital. 7
The aim of this article is to present our experience before elective repair of complex ventral hernia with the assistance of preoperative progressive pneumoperitoneum (PPP) and botulinum toxin type A (BTA).
Patients and Methods
Patients
Between May 2021 and December 2022, 13 patients admitted to our center for complex ventral hernia were retrospectively analyzed. All patients met the diagnostic criteria for complex abdominal hernia according to a consensus article on the definition of complex ventral hernia. 8 Informed consent was obtained from each patient for inclusion in the study.
Abdominal wall imaging
Before and after PPP and BTA, the changes in the lateral abdominal wall muscle length and abdominal circumference were measured from CT scan at the same vertebral level. 9
BTA and PPP technique
Patients received BTA and PPP procedure ∼1–2 weeks before surgery. The patient was in the lateral decubitus position, BTA was administered and received a dose of 100 or 150 U of BTA (for injection, BOTOX®, Allergan, Ireland), which was diluted to 2 U/mL with 0.9% saline and divided into six equal amounts. Using real-time ultrasound guidance, three sites were identified on each side of the abdomen along the anterior axillary line equidistant from the costal margin at the level of the ninth rib and a point anterior to the anterior superior iliac spine, as previously identified. 10 Next, the patient returned to supine position, a 14F deep venous catheter was introduced as an intraperitoneal catheter under real-time ultrasound guidance. We insufflated 400 mL of air daily using a 50-mL syringe. After the insufflation, the length of lateral muscle and abdominal circumference were evaluated again by CT scan the day before the patient was programmed for surgery.
Surgical procedure
All patients underwent laparoscopic intraperitoneal onlay mesh (IPOM) or laparoscopic-open-laparoscopic (LOL) IPOM repair. The patient was supine and a catheter was routinely inserted after general anesthesia. A routine 12-mm camera port and two 5-mm working ports were inserted as required contralateral to the defect under direct vision. The hernia contents were returned to the abdominal cavity. For those with dense adhesions that were difficult to separate, temporarily switch to LOL repair. Fascial closure was achieved using slow-absorbable sutures in a transverse shoelace pattern along the length of the defect. A composite anti-adhesion mesh (Bard Sepramesh™ or Parietex™) was used to completely cover the defect >5 cm in all directions and was fixed with a nail gun.
Postoperatively, all patients were asked to worn an abdominal binder for >3 months to reduce the tension in the abdominal wall. Patients received intravenous prophylactic antibiotics to prevent infection and continued for 72 hours.
Statistical analysis
We used descriptive statistics, including means and standard deviations for continuous variables. The difference in lateral abdominal wall length and abdominal circumference were analyzed using the Student's t-test in SPSS version 26.0 software (IBM Corp, Armonk, NY, USA). A P value <.05 was considered to be statistically significant.
Results
Demographic and characteristics of patients
From May 2021 and December 2022, a total of 13 patients (4 males and 9 females) underwent PPP and BTA preparation. The baseline data of patients are listed in Table 1. The patients' mean age was (60.4 ± 13.3) years with a mean body mass index of (25.6 ± 3.8) kg/m2. Nine patients (69%) presented with midline defects, 3 patients (23%) presented with lateral defects, and 1 (8%) patient presented with midline and lateral defects. One patient had recurrent hernia and undergone two herniorrhaphy. The mean time since occurrence of the hernia was 20.8 months (range 1–120). The smallest defect size was 6 × 8 cm, whereas the largest was 12 × 14 cm.
Demographics and Characteristics of the Patients with Complex Ventral Hernia
BMI, body mass index; BTA, botulinum toxin A; PPP, preoperative progressive pneumoperitoneum.
Description of the PPP and BTA
The mean insufflated air volume for PPP was (3400 ± 876) mL (range 1200–4400 mL) PPP and BTA administration time was over 8.8 ± 2.5 days (range 3–13 days). Two patients developed abdominal pain (n = 2, 15.4%). One patient developed back pain (n = 1, 7.7%). No complication required intervention.
Changes in lateral abdominal wall muscle
A comparison of CT scans before and after BTA showed an increased abdominal muscle length and simultaneous decreased muscle thickness (Fig. 1). The mean length of the lateral muscle increased from 14.3 to 17.4 cm (Table 2), which is equivalent to an increase of 3.1 cm per side (P < .05). The mean thickness of the lateral muscle decreased from 2.2 to 1.5 cm, with a mean decrease of 0.7 cm per side (P < .05). The abdominal circumference increased from 81.8 to 87.9 cm (Fig. 2), with a mean increase of 6.1 cm (P < .05). Furthermore, CT image comparison of pre- and post-PPP demonstrating spontaneously reinstate the herniated contents (Fig. 3), and the remaining abdominal adhesion is clearly identifiable (Fig. 4).

Changes in length and thickness of lateral abdominal wall muscle before and after PPP and BTA. BTA, botulinum toxin A; PPP, preoperative progressive pneumoperitoneum.
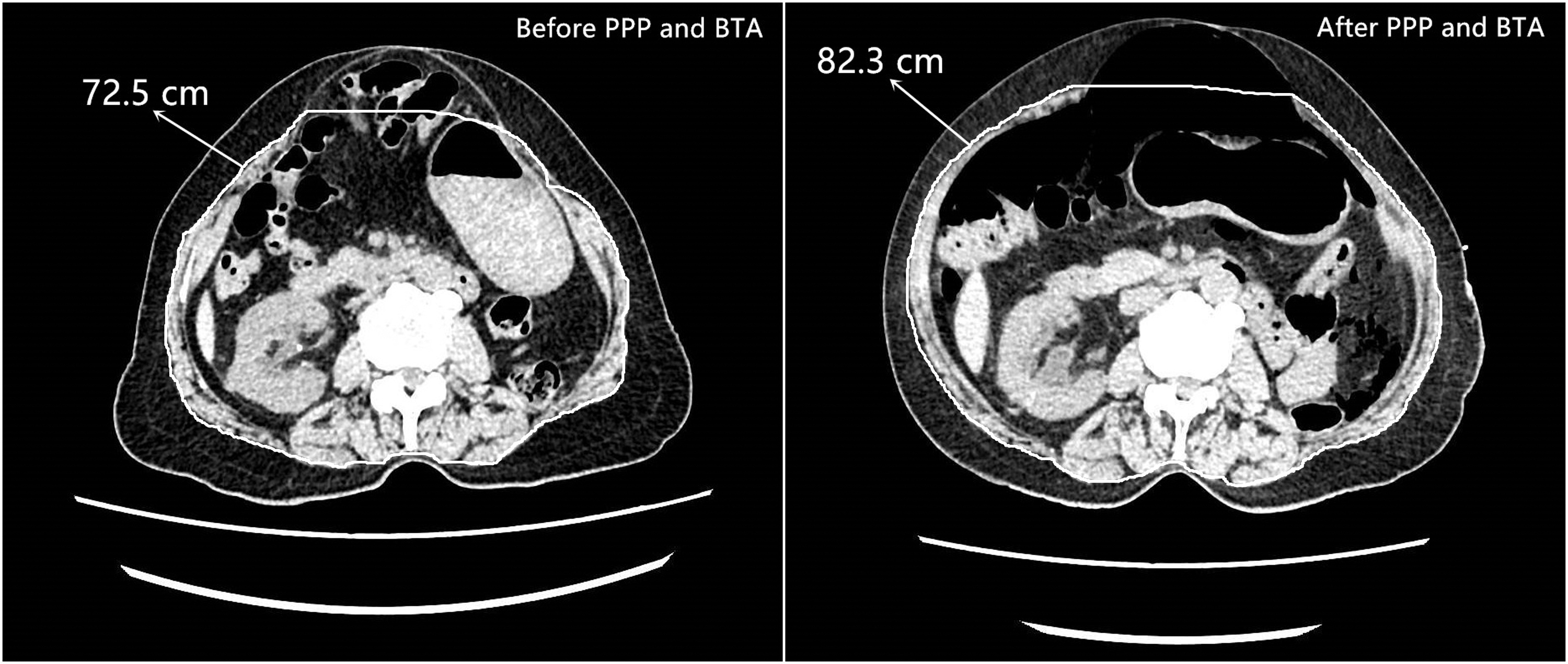
Changes in abdominal circumference of lateral abdominal wall muscle before and after PPP and BTA. BTA, botulinum toxin A; PPP, preoperative progressive pneumoperitoneum.

After PPP and BTA, a part of the hernia contents spontaneously returned to the abdominal cavity. BTA, botulinum toxin A; PPP, preoperative progressive pneumoperitoneum.
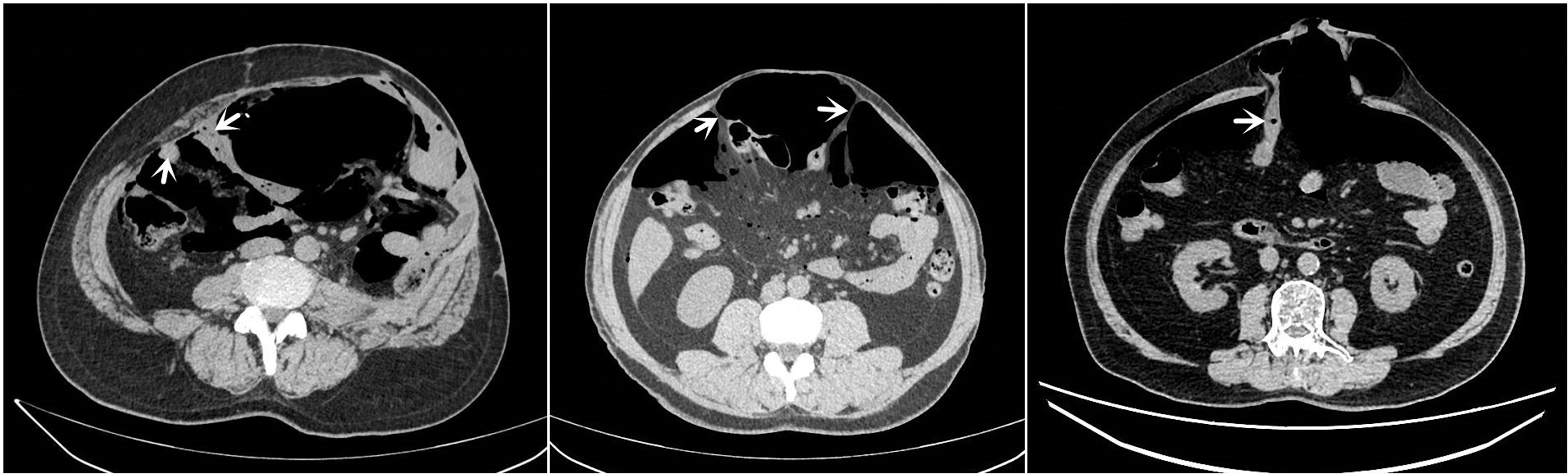
The preoperative imaging after PPP can clearly identify the adhesion area of abdominal wall (white arrow), which is helpful for the surgeon to establish initial port entry into the abdomen. PPP, preoperative progressive pneumoperitoneum.
Abdominal Computed Tomography Measurements of Lateral Muscle Length Undergoing Preoperative Progressive Pneumoperitoneum and Botulinum Toxin A Injection
Comparison of lateral abdominal muscle length before and after the preoperative combined use of PPP and BTA injection are shown, as measured on CT imaging.
BTA, botulinum toxin A; PT, patient. NA, not available.
Surgical outcomes
Eleven patients successfully underwent laparoscopic IPOM repair. Two patients underwent LOL repair due to dense adhesion. There was no obvious bleeding and bowel injury during surgery. The mean operative time was (257 ± 82) (160–428) minutes. Complete fascial closure was obtained in all patients (100%). Three patients developed incisional infection postoperatively and recovered after anti-infection treatment. One patient developed intestinal leakage on the fourth day and recovered after puncture drainage and anti-infection treatment. No patient had abdominal hypertension and ventilation impairment.
The average length of hospital stay was 21 days and the postoperative stay was 9 days. There are no hernia recurrences with a mean postoperative follow-up of 6.2 months (range 2–20 months).
Discussion
The repair of complex abdominal hernia represents a surgical challenge; preoperative careful preparation is vital. Therefore, the combination of PPP and BTA before surgery is becoming popular for the repair of complex abdominal hernias. 11
Elstner et al. reported on 27 patients with complex abdominal hernias who had 300 U of BTA injected into the abdominal wall muscle, the mean lateral muscle length increased by 4.2 cm. All hernias were successfully repaired and no hernias recurred after 16 months of follow-up. 12 In 2017, these authors again reported the use of 300 U BTA in patients with complex abdominal hernias, with a mean length gain of 4.0 cm/side was obtained. 13 Other studies have also proved that BTA has similar therapeutic effects. In our study, the effect of BTA allows an average increase of 3.1 cm per side in lateral muscle. Owing to such good effect, the abdominal wall defects were completely closed in 13 patients, and there is no complication during BTA management.
PPP has a significant advantage is the pneumoperitoneum's ability of the pneumatic dissection of intra-abdominal adhesions, which reduces the amount of dissection that must be performed during surgery.14,15 It is for this reason PPP also allows the spontaneous reduction of herniated viscera, 5 and this was also confirmed in this study (Fig. 3). Furthermore, the preoperative CT image after PPP can identify the adhesion area on the abdominal wall (Fig. 4), so it can be safer for initial port entry into the abdominal cavity.5,16
Some studies have combined PPP with BTA for the repair of complex abdominal wall hernia. Elstner et al. reported 16 patients with complex abdominal wall hernia, the abdominal circumference increased by 4.9 cm after PPP and BTA injection. All patients experienced successful fascial closure and mesh repair. 5 Bueno-Lledó et al. reported 70 patients with loss of domain hernia, an average reduction of 16.6% of the loss of domain ratio after PPP and BTA was obtained, but most patients undergone component separation technique to complete mesh repair. 6 Therefore, they believe that the combination of PPP and BTA can achieve better results.
We believe that the main advantage of PPP is that it can expand the abdominal cavity, and the patients gradually tolerate the increased abdominal pressure before surgery, which makes the abdominal pressure increase not obvious after the hernia content is fully returned, thus reducing the occurrence of abdominal hypertension and ventilatory impairment. The main advantage of BTA is to lengthen the lateral muscle length, plays the role of surgical component separation and facilitate the closure of intraoperative defects, and reduce the tension of the incision after surgery. In our study, benefiting from the advantages of PPP and BTA, IPOM was successfully performed in 11 patients. No patient had abdominal hypertension and ventilation impairment postoperatively. No patient has recurrent hernia after a mean follow-up of 6 months.
Conclusions
The preoperative combination of PPP and BTA is a feasible and safe approach for laparoscopic IPOM repair of complex ventral hernia. PPP increases the abdominal circumference, avoids postoperative abdominal hypertension and ventilatory impairment. BTA increases the muscle length of the lateral abdominal wall, plays a role similar to component separation technique while preserving primary anatomical structure. In addition, the paralyzing effect of BTA for about 6 months reduces the incisional tension after surgery, which is beneficial to the mechanical reconstruction of the patient's abdominal wall and reduces recurrence.
Footnotes
Acknowledgments
We acknowledge the assistance of Prof Hui Wang and Tai-Cheng Zhou, MD, in designing the study, and Ning Ma, MD, and En-Ming Huang, MD, in editing the article. Furthermore, we thank Prof Shuang Chen and Tao Ma, MD, for language editing in this study.
Disclosure Statement
No competing financial interests exist.
Funding Information
Our research is supported by National Key Clinical Discipline. This research was supported by Guangdong Science and Technology Plan Project (Grant No. 2021A1515410004).