
Abstract
Background:
Cryoanalgesia uses the application of cold temperatures to temporarily disrupt peripheral sensory nerve function for pain control. This review outlines the principles of cryoablation, clinical applications, and clinical data for its use in pediatric thoracic surgery.
Methods:
A comprehensive PubMed search was performed using the principal terms and combinations of cryoablation, cryoanalgesia, Nuss, Nuss repair, pectus, pectus excavatum, thoracic surgery, thoracotomy, and chest wall. Pediatric articles were reviewed and included if relevant. Adult articles were reviewed for supporting information as needed. Reference lists of included articles were reviewed for possible additional sources.
Discussion:
The scientific and clinical principles of cryoablation are outlined, followed by a focused review of current clinical application and outcome data.
Conclusion:
Postoperative pain is a major challenge following thoracic surgery. Cryoanalgesia is emerging as an adjunct in pediatric thoracic surgery, particularly for the Nuss procedure or minimally invasive repair of pectus excavatum. It effectively controls pain, decreasing postoperative opioid use and hospital length of stay with few short-term complications. Although more long-term studies are needed, early evidence suggests there is reliable return of sensation to the chest wall and long-term neuropathic pain is rare.
Introduction
The modern form of cryosurgery was described in 1962 by the neurosurgeon, Irving S. Cooper, who designed a cryosurgical probe that used liquid nitrogen to ablate the ventrolateral thalamus to alleviate tremors in Parkinson's patients. 1 Shortly thereafter, Lloyd et al. reported the successful treatment of 52 patients with intractable pain following cryoablation of peripheral nerves, including intercostal nerves, sacral nerve roots, and facial nerves. 2 Cryoanalgesia is increasingly used in thoracic surgery for postoperative pain control. Its mechanism of action relies on the temporary disruption of nerve function to provide analgesia, with subsequent nerve regeneration and return of sensation.
This review outlines the principles of cryoablation, its clinical applications, and the available outcome data for its current use in adult and pediatric thoracic surgery.
Methods
A comprehensive PubMed search of discussion topics was performed using the principal terms and combinations of cryoablation, cryoanalgesia, Nuss, Nuss repair, pectus, pectus excavatum, thoracic surgery, thoracotomy, and chest wall. Pediatric articles were reviewed and included if relevant. Articles were excluded if they did not discuss cryoanalgesia or thoracic surgery. Adult articles were reviewed for supporting information as needed. Reference lists of included articles were reviewed for possible additional sources.
This review focuses on the history, principles, and current clinical applications of cryoablation for postoperative pain control in thoracic surgery.
Discussion
Scientific principles of cryoablation
History and biology
Cryoanalgesia capitalizes on the remarkable potential of peripheral nerve regeneration following injury. Within a nerve, each axon is surrounded by a layer of connective tissue called the endoneurium. Groups of axons are bundled together into fascicles and wrapped in perineurium. The entire nerve is wrapped in an outermost layer of connective tissue called the epineurium (Fig. 1). Following damage to the axon of a peripheral neuron, the axon can regenerate if the cell body of the neuron is intact. Axonal injury, be it mechanical or thermal, results in Wallerian degeneration distal to the site of injury. The injured axon loses cell membrane integrity, and the axonal cytoskeleton breaks down. The myelin sheath next undergoes degeneration followed by infiltration of macrophages and Schwann cells, which clear the cellular debris, leaving behind the connective tissue sheaths: the endoneurium, perineurium, and epineurium.3,4
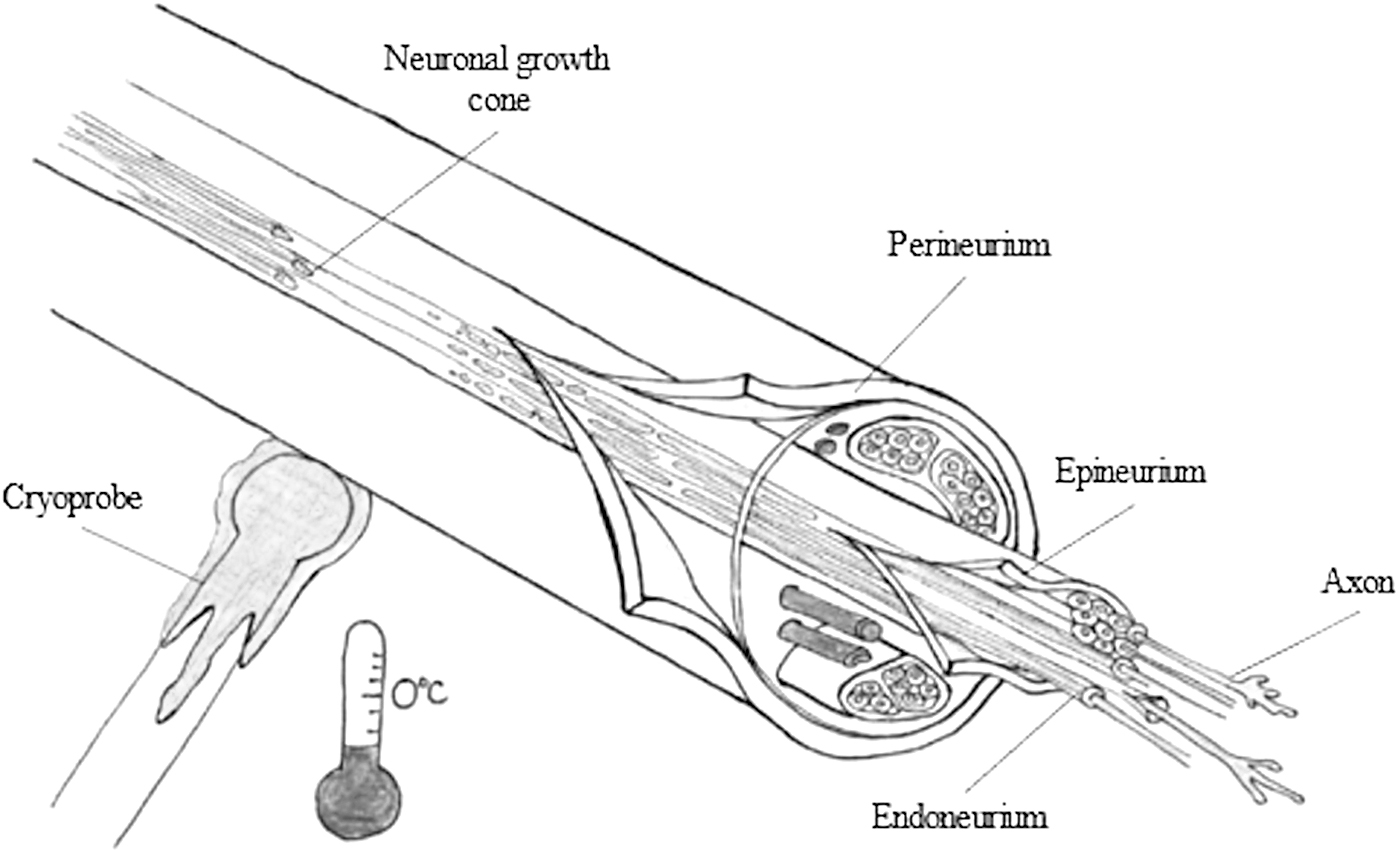
Axonotmesis induced by cryoablation. Axon thermal injury at the point of cold probe contact results in downstream Wallerian degeneration of the axon. The endoneurium, perineurium, and epineurium remain intact. Within days of axonal injury, the growth cone forms and axonal regeneration begins.
Schwann cells proliferate, aligning along the connective tissue tubes (Büngner bands), and produce neurotrophic factors that promote and guide axonal regeneration. Within days of injury, a growth cone forms at the distal tip of the axon, proximal to the injury site. The growth cone migrates toward the Büngner bands, paving the way for axonal regeneration. 3 Peripheral nerves regenerate at a rate of 1–2 mm/day in more distal segments and up to 2–3 mm/day in proximal segments, eventually reinnervating the target tissue.
The goal of cryoanalgesia is controlled thermal injury to the targeted nerve, resulting in disruption of the axons, while preserving the neural sheaths and allowing subsequent axonal regeneration (Fig. 1). Cryoablation induces thermal nerve injury at the site of probe contact through formation of intracellular and extracellular ice crystals, leading to changes in cellular osmolality and permeability and subsequent axonal injury. 5 The neural sheaths comprise fibrous connective tissue that are more resistant to damage from freezing. 6 Seddon classified the degree of nerve injury according to the extent of demyelination and prognosis for neuroregeneration. 7
Alternatively, Sunderland classified nerve injury by the extent of damage to individual elements of the nerve (Table 1). 8 Zhou et al. studied the effects of freezing sciatic nerves of rabbits to temperatures between −20°C and −180°C. 6 The morphology of the frozen nerves were studied using light and electron microscopy, while the nerve function was assessed using somatosensory evoked potentials, sensory conduction velocity, and electromyogram at various intervals after freezing. There was no morphologic or functional change in nerves at −20°C. Cryoinjury to temperatures between −60°C and −100°C resulted in “axonotmesis” per Seddon taxonomy, with axonal degeneration and neural sheath preservation, and subsequent functional recovery. At these temperatures, the endoneurium, perineurium, and epineurium remained intact, resulting in a Sunderland Grade II injury.
Summary of Nerve Injury
Adapted from Menorca 2013, Ilfeld 2020.
At −140°C and colder, there was destruction of basal membranes of the nerve sheath and permanent nerve damage. 6 Similarly, Hsu and Stevenson found that cold application at −60°C to the rat tibial nerve resulted in the loss of hind limb motor function, with axonal demyelination and degeneration, but preservation of the epineurium and perineurium seen on pathologic review at 2 weeks. 9 There was complete axonal regeneration, remyelination, and functional recovery by 16 weeks. Peripheral nerve cryoablation to temperatures between −60°C and −100°C “transects” the axons from within, while preserving the nerve sheath to allow for axonal regeneration (Fig. 1).
To investigate factors influencing duration and efficacy of cryoablation, Evans et al. studied different freezing cycles applied to rat sciatic nerves. 10 They manipulated the freezing temperature and the duration of freezing and monitored for sensory and motor recovery. At temperatures warmer than −20°C, the number of days to return of sensation was significantly fewer than colder temperatures. However, when cooled to less than −20°C, temperature did not influence recovery time. Duration of cryoablation similarly had no significant impact on the return of sensation when temperatures were −20°C or colder.
The authors specifically note the unpredictability of sensory and motor effects observed when temperatures applied ranged from 0°C to −20°C. More recently, Moorjani et al. performed cryoablation of intercostal nerves in dogs at a temperature of −50°C for 30, 60, 90, and 120 seconds, and subsequently biopsied the nerves at regular intervals over 6 months. 11 Axonal degeneration with intact endoneurium (axonotmesis injury) was observed for all cryoablation durations tested. Histologically, axonal regeneration was complete after 1 month in the 30- and 60-second groups. Increased time to the start of regeneration and subsequent neuronal recovery were observed among the 90- and 120-second groups; however, the timing of this process was not reported by the authors. Their findings suggest that duration of cold application affects the rate of axonal regeneration, but no mechanism is offered to explain this finding.
Beazley et al. documented the timeline of peripheral nerve regeneration following facial nerve cryoablation in primates. 12 A cryoprobe was applied to the right facial nerve at −40°C for a total of 4 minutes. Following this application, complete nerve palsy was observed; recovery of normal nerve function began at 5 weeks with complete recovery observed at 9 weeks post-cryoablation. Axonal regeneration occurred at a rate of 1–3 mm per day. The histological studies performed in the literature were conducted on animals with different never fiber diameters; it is unclear how these findings translate to humans. These studies demonstrate that there is a temperature threshold for achieving axonal injury with nerve sheath preservation. However, the effects of the duration of cryoablation, repeated exposure, and nerve size are less clear.
Mechanism of cooling
Commercially available cryoprobes consist of an inner single-walled aluminum tube, covered with an insulating outer tube. The inner layer is thermally conductive and serves as the conduit down which pressurized gas (usually nitrous oxide or carbon dioxide) travels (Fig. 2). Rapid cooling of the cryoprobe tip results from the Joule-Thomson effect; as gas is released into the larger diameter, low-pressure outer tube, it rapidly expands and absorbs surrounding heat, thereby cooling the tip of the probe. 13

Pressurized gas travels down the inner tube. Rapid cooling of the probe tip occurs as the gas is released into the larger diameter outer tube at relatively lower pressures, absorbing surrounding heat (Joule-Thomson effect).
The effect of cryoablation on tissues surrounding the desired point of contact is mitigated by the heat sink phenomenon, where adjacent blood flow within adjacent vessels quickly disperses and equilibrates local temperature change. 14 After cooling is complete, the cryoprobe undergoes an active defrosting phase to permit detachment of the probe from the tissue without causing mechanical injury. 15 This defrost phase is controlled to prevent reheating of the frozen tissue, as slow thawing of frozen tissue is associated with maximal axonal injury effect. 16
Clinical principles of cryoanalgesia
Cryoablation affects both motor and sensory nerves. Thoracic surgery is painful and well suited for intercostal nerve cryoablation, as the motor component is almost exclusive to the intercostal muscles, which are not vital to quiet respiration.17,18 In addition, the intercostal nerves are easily accessible and identified below the ribs. In contrast, nerves to the abdomen and extremities are usually deep in the tissue and loss of motor innervation would result in disability.
The myotomes and dermatomes of the thoracoabdominal cavity are key considerations. The nerve roots at T1 and T2 are associated with the cervical sympathetic chain and provide sensory and motor innervation to the upper extremity. 19 Cryoablation of the T1 and T2 can result in Horner's syndrome or functional deficits to the upper extremity and should be avoided. The intercostal nerves from T3 to T8 contain sensory and motor nerves. The motor nerves of T3–T8 provide innervation of intercostal muscles. Loss of intercostal muscle function is well tolerated.17,18 Cryoablation of intercostal nerves T3–T8 results in the loss of sensation from the manubrium to just below the xiphoid and provides analgesia for most thoracic operations.
Cryoablation of intercostal nerves T9 and lower should be undertaken with caution, as these nerves provide motor innervation to the abdominal musculature and can theoretically result in laxity of the abdominal wall. Nerve function is disrupted distal to the site of cold application; therefore, the more proximal the cryoprobe is applied on the nerve, the greater the resulting area of analgesia. There is theoretical concern that applying the cryoprobe near the nerve root as it emerges from the neural foramen could result in injury to the spinal cord. Manufacturer recommendations suggest placing the cryoprobe a minimum of 4 cm from the base of the spine, or 2 cm from the ganglia. 20 In general, it is recommended to perform cryoablation at the intercostal level of the thoracotomy incision as well as at two intercostal levels above, and two levels below the incision.
The cryoprobe can be applied to the intercostal neurovascular bundle through an intrathoracic or extrathoracic approach. An intrathoracic approach is generally employed for an open thoracotomy or video-assisted thoracoscopy. Cryoanalgesia is increasingly used during thoracoscopic operations and the cryoprobe is similarly applied under direct thoracoscopic visualization. Alternatively, the cryoprobe can be applied extrathoracically; the cryoprobe is tunneled subcutaneously and applied to the intercostal neurovascular bundle. To date, there is no head-to-head comparison of external versus internal application of cryoanalgesia.
Thoracic cryoanalgesia in adults
Briefly, the literature in adults describes more varied applications of cryoanalgesia. Recently, Park et al. published a systematic review and meta-analysis of cryoablation for postoperative analgesia in adults, which included 20 articles pertaining to thoracotomies. 21 In general, cryoablation was associated with decreased opioid use compared to intercostal nerve blocks, but not compared to epidurals. There was variation in the technique, ranging from −20°C to −70°C for 30–120 seconds over 3–8 intercostal nerves. However, most articles were published over 10 years ago and cryoanalgesia devices and technology have evolved in the interim. Cha et al. reached a similar conclusion in their systematic review on the efficacy of intercostal nerve cryoablation as an analgesic adjunct to other modalities. 22 They provided a recommendation that cryoablation leads to decreased postoperative narcotic use and pain scores (grade 2A and 2C evidence respectively) in patients undergoing a thoracotomy.
Lau et al. randomized patients undergoing minimally invasive thoracotomy heart valve surgery to cryoablation plus standard-of-care opioids or standard-of-care opioids alone. 23 The primary endpoint was forced expiratory volume in 1 second (FEV1), which was noted to be significantly higher in the cryoablation group up to 48 hours postoperatively only. While there was a 13% decrease in overall opioid use during hospital stay for the cryoablation group, it was not statistically significant. In another study, Tung et al. used cryoablation as an adjunct to their institutional standard multimodal regimen in 10 patients undergoing robotic-assisted pulmonary resection. 24 Both inpatient and outpatient opioid use were significantly lower in the cryoablation group. Seven patients who received cryoablation were discharged home without an opioid prescription.
Several studies examine cryoablation for rib fractures, which are associated with significant morbidity and mortality. Finneran et al. used ultrasound-guided percutaneous cryoablation in a series of 5 patients with traumatic rib fractures, demonstrating decreased pain scores and opioid use and increased incentive spirometry volumes. 25 At 3-month follow-up, no patient reported neuropathic pain. When combining cryoablation with surgical stabilization of rib fractures, there is conflicting evidence on its effect on postoperative opioid use.26,27 When looking at pain scores as a clinical endpoint, Zhao et al. found significant improvement in postoperative pain scores in 13 patients. 28 However, this study lacked objective measures such as opioid use and fails to distinguish whether the improvement in pain score was the result of cryoanalgesia or the concomitant rib stabilization procedure.
Thoracic cryoanalgesia in children
Minimally invasive repair of pectus excavatum
Minimally invasive repair of pectus excavatum (MIRPE), or the Nuss procedure, is the most commonly reported application of cryoanalgesia in the pediatric population. MIRPE is typically associated with significant postoperative pain, as the chest is instantaneously remodeled with insertion of bars behind the sternum. 29 Numerous regimens of multimodal analgesia are described, including combinations of thoracic epidural, intravenous patient-controlled analgesia (PCA), indwelling catheter infusions, local or regional nerve blocks, and oral analgesia (opioids, anti-inflammatories, and gabapentinoids).30–35 A standardized approach to perioperative pain management has not been established.
Cryoanalgesia as a pain-control strategy following MIRPE was first reported by Keller et al. in 2016. 36 This retrospective study compared 26 patients with cryoanalgesia to 26 patients with a thoracic epidural. The cryoprobe was tunneled subcutaneously and applied to the intercostal neurovascular bundle from outside the chest wall with thoracoscopic visualization of the intrathoracic formation of a “frost ball.” Cryoanalgesia patients used less postoperative opioids and had a shorter hospital length of stay (LOS). In 2019, Graves et al. reported a randomized controlled trial comparing cryoanalgesia to thoracic epidural in patients undergoing MIRPE. 37
Each treatment arm included 10 patients, all of whom received a PCA postoperatively. Cryoanalgesia was performed bilaterally to the intercostal nerves, T3–T7, for a 2-minute duration at each nerve, at a temperature of −60°C. Pain scores were similar between the study cohorts; however, the cryoanalgesia group required 61% less opioid overall than the epidural group.
Furthermore, the median LOS for the cryoanalgesia group was 3 days compared to 5 days for the epidural group. These findings were substantiated by Parrado et al. who compared cryoanalgesia to thoracic elastomeric pain pumps and found similar pain scores between groups, with decreased opioid requirements in the cryoanalgesia group. 38 Table 2 provides a summary of the pediatric experience using cryoanalgesia in the repair of pectus excavatum. Most were small, single-institution retrospective studies, with the largest pediatric cohort of 350 patients.
Summary of Cryoablation Used During the Repair of Pectus Excavatum and Pectus Carinatum
The cryoablation group had shorter time to discontinuation of oral opioid analgesia.
EPP, elastomeric pain pump; ICB, intercostal nerve block; LOS, length of stay; MIRPE, minimally invasive repair of pectus excavatum; MM, multimodal medication; n/a, not available; PCA, patient-controlled analgesia; TE, thoracic epidural.
Overall, most groups found that cryoanalgesia provided equally effective pain control compared to other strategies such as PCA, thoracic epidural, and elastomeric pain pumps. Importantly, cryoanalgesia was associated with decreased inpatient opioid use and shortened LOS. Of the studies that tracked postoperative neuropathic pain, no patient had lasting effects. There was more uniformity in the cryoablation technique in the pediatric experience compared to techniques reported in the adult literature. In children, cryoanalgesia was generally applied to 4–5 intercostal nerves to a temperature of −60°C for 2 minutes.
The use of cryoablation has repeatedly been associated with decreased LOS; many studies have demonstrated the ability for safe discharge on postoperative day 1.39–43 In 2022, Rettig et al. 41 conducted a retrospective study of 30 patients undergoing the MIRPE with cryoablation to determine the safety of same-day discharge. On postoperative day 0, 10 patients were discharged home after meeting appropriate criteria (tolerate oral intake, pain adequately controlled with oral pain medications, able to void spontaneously, and no major pneumothorax). Of the 10 patients, 1 returned to an urgent care for constipation.
An additional potential benefit of using cryoablation in the MIRPE is decreased overall hospital costs; however, there are conflicting reports in literature, which may be due to differences in charges between hospital systems. Graves et al. commented that the increased operating room costs including equipment and operative time were offset by a decreased LOS. 37 Three separate groups have quantified a cost benefit, noting ∼$2,000–$7,000 less in cryoablation patients; $14,072 versus $21,021, 42 $21,924 versus $23,694, 43 $15,976 versus $18,336. 44 However, Mehl et al. reported cryoablation being associated with increased total hospital costs in comparison to PCA ($11,145 versus $8975, P < .01), but there was no significant cost difference when compared to epidural or PCA with peripheral nerve block. 45 Operating room supplies was the primary factor for increased cost with cryoablation.
Other chest wall procedures
Cryoanalgesia is also reported in open thoracic surgery in children. A prospective study of 9 patients by Pilkington et al. 46 demonstrated that intercostal nerve cryoablation reduced LOS by 2 days following the modified Ravitch for pectus deformities compared to thoracic epidural analgesia (Table 2). There was an initial benefit with improved pain control scores in the cryoanalgesia group on POD#2, but no significant difference overall in total postoperative opioid use or discharge prescription. The LOS was shortened by 2 days with cryoablation.
Similarly, Gologorsky et al. retrospectively reviewed the postoperative pain scores of 5 patients who underwent open repair of pectus carinatum with cryoablation. 47 The median LOS was 1 day and only one patient reported a pain score higher than 0. One week postoperatively, all patients reported scores of 0 and none developed neuropathic pain by 1 year.
Chen et al. 48 performed a retrospective study of 32 patients who underwent 53 thoracotomies for oncological resection. The use of cryoablation was employed in 14 of the 53 thoracotomies; patients with cryoanalgesia used significantly less opiates during hospitalization and at discharge. They also found significantly lower pain score among those with cryoanalgesia by postoperative day 4.
The use of cryoanalgesia has also been reported in the treatment of slipping rib. Krista Lai et al. 49 conducted a retrospective review of 98 patients who underwent treatment for slipping rib with cartilaginous rib excision. Of these patients, intercostal nerve cryoanalgesia was employed in 30. The researchers similarly found a decrease in opiate use and length of hospitalization with the use of cryoanalgesia.
Complications
There is a range of potential complications arising from the use of cryoablation. While short-term complications are described in the articles previously referenced, there is a paucity of literature dedicated to long-term effects. In Park et al.'s systematic review of thoracic cryoanalgesia in adults, pooling of two studies in the meta-analysis showed cryoablation significantly improved persistent pain at 1 month postoperatively. 21 However, they noted incomplete and inconsistent reporting of adverse events, which precluded any further pooling and analysis of other complications. The increase of cryoablation during MIRPE in the pediatric population discussed in the literature has led to a more robust understanding of complications associated with cryoablation.
Sensation
Long-term sensory loss is a concern following cryoablation, but as of yet, prospective data regarding the duration of symptoms are limited. A number of retrospective studies have investigated numbness and hypoesthesia following intercostal nerve cryoablation with an incidence of persistent hypoesthesia ranging from 15% to 38% at 6 months.11,40,50–53 A retrospective study performed in 2022 of 40 patients treated with cryoanalgesia during MIRPE found that at 6 months postoperatively, 15% of patients had residual chest wall hypoesthesia. On physical examination, a 2 cm band of residual numbness below the nipple was observed in 66% of patients with persistent hypoesthesia at 6 months. By 1 year postoperatively, all patients had return of chest wall sensation. 40 A 2019 randomized trial also found complete chest wall sensation return in patients 14–31 years of age, who underwent the MIRPE with cryoablation at 1 year postoperatively. 37
More recently, Zobel et al. observed a difference in return of normal chest wall sensation following intercostal cryoablation during the MIRPE based on patient age. 54 Adult patients experienced prolonged numbness relative to pediatric patients (10.7 versus 3.4 months, P = .003). Among all patients, the frequency of numbness lasting longer than 12 months following cryoablation was 9.3%, and only 3.3% among children. These data support the premise that nerve healing and regeneration are accelerated in younger patients, which has been corroborated by numerous studies examining the effect of age on the recovery rate following peripheral nerve reconstruction/injury.55–57
Neuropathic pain
Neuropathic pain is a reported complication following cryoablation. The pathophysiology of neuropathic pain is likely due to failure of peripheral nerve fibers to fully regenerate within the remaining axonal sheath following Wallerian degeneration. The incidence may vary based on patient age. Zobel et al. employed the S-LANSS, a validated questionnaire designed to quantify neuropathic symptoms, in adult and pediatric patients who underwent cryoablation during MIRPE. The incidence of neuropathic pain was significantly lower for patients younger than 21 years. 54
Specifically, no patient younger than 21 years experienced neuropathic pain, defined as an S-LANSS score greater than 12. Among the 5 (38.5%) adult patients with neuropathic pain at 1 month, 40% resolved with the initiation of gabapentin alone; in total, 23% of the patients older than 21 years experienced neuropathic pain more than 6 months postcryoablation. In another study of pediatric patients with cryoablation during MIRPE, Sun et al. reported that 6% of patients experienced allodynia, between 3 months and 1 year after surgery; they observed complete resolution of symptoms in all patients by 1 year postcryoablation, using medical management or biofeedback. 58
The incidence of neuropathic pain following cryoablation varies within adult literature. Lau et al. reported that 1.6% (1/63) of patients who underwent minimally invasive cardiac surgery with cryoanalgesia had allodynia at 6 months, symptoms were self-limited, and improved without intervention by 10 months postoperatively. 23 Tung et al. similarly observed 10% (1/10) of patients who underwent cryoablation for minimally invasive thoracic surgery, who experienced neuralgia postoperatively, which resolved after 1 month of gabapentin therapy. 24 In contrast, higher rates of neuropathic pain have been reported in open thoracic surgery.
Mustola et al. studied adult patients who underwent thoracotomy with the utilization of cryoanalgesia. They reported rates of neuropathic pain in 55% of patients at 8 weeks; symptoms persisted in 30% of patients at 6 months 52 Yang et al. reported a similar incidence of neuropathic pain of 40% at 6 months in patients who underwent thoracotomy with cryoanalgesia. 51 In summary, neuropathic pain is a potential consequence of cryoablation, although the risk of development of neuropathic pain in pediatric patients is reported to be lower than adults. Symptoms in most patients can be managed medically with a high rate of resolution of symptoms.
Delayed pneumothorax
Delayed pneumothorax is uncommon, but can be a significant complication following intrathoracic cryoablation with reported rates of 0%–11% of cases.38,39,58,59 In most cases, delayed pneumothorax is thought to be attributed to unintentional contact of the lung tissue with the cryoprobe. The site of injury does not immediately lead to bronchial-alveolar communication to the thoracic cavity. Over time, the site of cryoinjury results in tissue necrosis and a delayed air leak. Parrado et al. reported a 9% incidence of delayed pneumothorax requiring postoperative thoracostomy tube placement. 38 The investigators suggest that aside from direct contact with the cryoprobe, lung injury occurs as a result of contact between the lung and frozen chest wall. The authors propose allowing the chest wall to thaw for 3 minutes before lung expansion.
An additional strategy to reduce parenchymal contact with the probe is single-lung ventilation using a double-lumen endotracheal tube; however, Graves et al. still observed the development of a delayed pneumothorax in 1 patient (1/10) with this strategy. 37 Morikawa et al. described a novel strategy for avoiding direct contact with pulmonary tissue and the cryoprobe by placing a cut 20-French chest tube over the cryoprobe to reduce potential contact surface area; with this strategy, they report no postoperative pneumothorax in their cohort of 6 patients. 60 Surgeons should be mindful of the cryoprobe location when performing intrathoracic cryoablation, given the risk of delayed pneumothorax due to direct pulmonary parenchymal contact with the cold cryoprobe.
Wound complications
A theoretical risk of cryoablation is increased wound complications due to the association of perioperative patient hypothermia and wound complications.60,61 The development of patient hypothermia during cryoablation is likely mitigated by the “thermal sink” effect of the intercostal vessels. In 4 studies, 3 of which were conducted in pediatric patients undergoing MIRPE58,59,62,63 found no significant difference in the incidence of surgical site infection between the patients with received cryoablation and those who did not. Bundrant et al. reviewed perioperative core body temperatures of 35 patients who underwent MIPRE with and without cryoablation. 64 The authors found that patients with cryoablation had a significantly lower median body temperature in the recovery room than those without cryoablation; however, they found no difference in surgical site infection between patient with and without cryoablation.
While a thermal injury similar to frostbite has been reported with the use of cryoablation to treat an aneurysmal bone cyst, 65 there is no specific mention of this complication in the chest wall literature. Careful application of the cryoablation probe to tissue is key to preventing wound complications. While the shaft of the probe does have a protective covering layer, it is not completely insulating, and caution should be taken to prevent contact of the probe tip and shaft with lung intrathoracically and skin extrathoracically.
Bar slippage
Following MIRPE, bar displacement resulting in inadequate chest wall correction and reoperation occurs in 2%–3% of patients.66–68 Bar stabilization techniques and activity restrictions may help mitigate the risk of bar displacement. Two studies found significantly increased rates (8%–12%)36,58 in cryoablation groups compared to controls, while another reported a rate of 0.6% in a series of 350 cryoablation patients. 39 The slippage is potentially explained by decreased pain and increased movement postoperatively. Care should be taken to ensure bar stabilization and compliance with activity restrictions.
Pulmonary function
Intercostal muscles play a complementary role in quiet respiration, 17 making intercostal nerve cryoablation an attractive method of analgesia with potentially minimal effect on pulmonary function. Lai et al. examined incentive spirometry volumes as a measure of pulmonary function following MIRPE procedure and found no difference between the cryoablation, elastomeric pain pump, and multimodal regimen alone groups. 69 Within adult thoracotomy literature, Rooney et al. compared the pulmonary function tests of patients who received either transcutaneous nerve stimulation (TNS) or cryoablation as an analgesic adjunct. 70
The cryoablation group had lower forced vital capacity (FVC), FEV1, and negative inspiratory force (NIF) pressures on POD#1 compared to the TNS and control groups. However, by POD#5, the cryoablation group had recovered with significantly better FVC and FEV1 volumes than both groups and improved NIF than the control group. In more recent studies, the cryoablation group achieved better FVC and FEV1 volumes throughout the postoperative period, but the differences were not significant. 11 Yang et al. also reported improved FVC and FEV1 volumes postoperatively with cryoablation added to a thoracic epidural. 51 However, only the POD#7 FVC reached significance.
Conclusion
Cryoanalgesia is particularly well suited to thoracic surgery. Numerous studies in adults and children show cryoablation is effective at controlling postoperative pain and decreasing opioid use and LOS for both thoracoscopic and open operations. Although more long-term studies are needed, early evidence suggests there is reliable return of sensation to the chest wall and long-term neuropathic pain is rare.
Footnotes
Acknowledgments
Research was conducted by the authors of the article.
Authors' Contributions
K.L.: investigation and writing—original draft preparation, R.S.E.: investigation and writing—review and Editing, M.Z.: investigation and writing—original draft preparation, A.H.-V.: investigation, A.O.: investigation, and B.E.P.: supervision and writing—reviewing and editing.
Disclosure Statement
B.E.P. is an educational consultant for Atricure. K.L., R.S.E., M.Z., A.H.-V., and A.O. have no disclosure.
Funding Information
No funding was received for this article.