
Abstract
Background:
Three-dimensional (3D) laparoscopy provides stereopsis and may reduce operating time (OT) and morbidity. However, there is a paucity of literature on its use in laparoscopic liver resection (LLR). This study aims to compare outcomes between 3D and two-dimensional (2D) LLR.
Materials and Methods:
PubMed, Embase, Scopus, and the Cochrane Library were systematically searched from inception to November 2022. The inclusion criterion was studies comparing intraoperative characteristics and/or postoperative outcomes between 3D and 2D LLR. Studies on the use of 3D image reconstruction techniques for preoperative planning were excluded. Primary outcomes were OT, estimated blood loss (EBL), and overall morbidity. Secondary outcomes were other postoperative complications, need for reoperation, and in-hospital mortality.
Results:
Four studies with 361 patients (3D: n = 159, 2D: n = 202) were included. There were 65.3% males (overall: n = 236/361). Age, sex, body–mass index, incidence of diabetes mellitus, hepatitis B and/or C carrier, receipt of neoadjuvant chemotherapy, tumor size, and incidence of multiple tumors were comparable between 3D and 2D LLR. No studies reported on Child–Pugh status. One study included only patients with hepatocellular carcinoma, two studies included patients with mixed histopathology, and one study did not report on histopathology. There was no significant difference in OT (mean difference [MD] −31.6 minutes, 95% confidence interval [CI]: −89.7 to 26.5), EBL (MD −454.1 mL, 95% CI: −978.8 to 70.6), need for reoperation (odds ratio [OR] 0.91, 95% CI: 0.18–4.61), and in-hospital mortality (OR 0.52, 95% CI: 0.06–5.50) between 3D and 2D LLR. Overall morbidity was lower in 3D LLR (OR 0.56, 95% CI: 0.32–0.98, P = .04). However, the learning curve (LC) was not described in the included studies and may confound outcomes.
Conclusions:
3D LLR may reduce overall postoperative morbidity compared with 2D LLR, but results may be confounded by the lack of standardization of surgeons' experience and the LC of 3D LLR.
Introduction
Technological advancements and diffusion of surgical expertise have resulted in widespread adoption of minimally invasive surgery. Adoption of laparoscopic liver resection (LLR) was slow, but it has expanded globally in recent decades.1,2 Current literature has shown that LLR has superior short-term postoperative outcomes compared with open liver resection.3,4 Technological advancements have led to increasing use of robotic surgery.
Although evidence for the use of robotic liver resection has shown similar postoperative outcomes compared with LLR, 5 the use of robotic surgery in gastrointestinal surgeries such as total and distal gastrectomy has been shown to result in better postoperative outcomes and lymph node harvest compared with laparoscopic surgery.6,7 This may be due to the benefits offered by robotic surgery—three-dimensional (3D) depth perception, elimination of hand tremors, and a wider range of manipulation with robotic arms. 8
However, to what extent are the benefits of robotic surgery due to the availability of 3D depth perception? 3D laparoscopy serves as a bridge between conventional two-dimensional (2D) laparoscopy and robotic surgery by providing added stereopsis for depth perception, but at a much lower cost compared with robotic surgery. 9 Meta-analyses on the use of 3D versus 2D laparoscopy for right colectomy, gastrectomy, and various urological surgeries showed reduced operating time (OT) and reduced morbidity with 3D laparoscopy10–12 ; this has been postulated to be due to better visualization of critical structures with stereopsis, allowing for faster and more precise appreciation of surgical anatomy and dissection.
The European Association for Endoscopic Surgery (EAES) consensus development conference in 2018 recommended the use of 3D laparoscopy to reduce OT (grade of recommendation low). 13 A recommendation (high grade) was made for future research to investigate the benefit of 3D laparoscopy in reducing postoperative morbidity. However, regarding the role of 3D laparoscopy in LLR, there was only one study identified in the 2018 EAES consensus. 14 This shows the lacuna of evidence on the role of 3D laparoscopy in LLR.
Hence, this review aims to systematically review evidence on the intraoperative and postoperative outcomes of 3D LLR versus 2D LLR.
Materials and Methods
Study selection and search strategy
This systematic review and meta-analysis was performed according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 15 The study protocol was registered at PROSPERO (Ref No.: CRD42022372474). Four databases (PubMed, Embase, Scopus, and the Cochrane Library) were systematically searched for studies published from inception to November 6, 2022.
A combination of search terms (((“3D” OR “3-dimension*”) OR (“2D” OR “2-dimension*”)) AND (“liver resection” OR “hepatectomy”)) was used. The complete search strategy for each database is appended in Supplementary Table S1.
The inclusion criterion for our study was randomized controlled trials (RCTs) or non-RCTs comparing intraoperative characteristics and/or postoperative outcomes between 3D and 2D LLR. Exclusion criteria were (a) studies that were not relevant to 3D LLR, (b) single-arm studies or studies comparing 3D laparoscopy with other types of surgical access (e.g., open or robotic surgery), (c) studies on preoperative planning using 3D image reconstruction techniques, (d) studies on mixed reality or augmented reality, or (e) based on types of articles (conference abstracts, case report or series, editorials, expert opinions, review articles without original data, and non-English studies).
After removal of duplicates, abstracts were independently screened for potential inclusion by two authors (K.S.C. and V.G.S.) based on the defined inclusion and exclusion criteria. The authors subsequently reviewed the full texts. There were no studies reporting data on the same cohort of patients. Any discrepancies were resolved by consensus between the two authors.
Data extraction
Data extraction was independently conducted by two authors (K.S.C. and V.G.S.). The following details were extracted from each study: publication details (name of the first author, publication year, and country), study characteristics (sample size, sex, age, sex, comorbidities, previous abdominal surgery, Child–Pugh score, alpha-feto protein (AFP), extent of LR, and presence of preoperative treatment), histopathological characteristics (histopathology, size of tumor, number of lesions, and Barcelona Clinic Liver Cancer staging), intraoperative factors (OT, liver parenchyma transection time, estimated blood loss [EBL], and need for open conversion), and postoperative outcomes (overall morbidity, major morbidity, posthepatectomy liver failure [PHLF], length of hospitalization stay [LOS], need for reoperation, and mortality).
Liver parenchymal transection time was defined as the time from the beginning of liver transection to division of liver outflow. Overall morbidity was defined as the presence of any postoperative complications included by the authors, for example, intra-abdominal collection, bile leak, infectious complications, pulmonary complications, and pneumonia. Major morbidity was defined as Clavien–Dindo ≥ Grade 3A morbidity. 16 PHLF was determined using the 50–50 criteria on postoperative day 5 in all included studies (Kawai et al. 17 and Velayutham et al. 18 ). 19
Our primary outcomes were OT, EBL, and overall morbidity. Our secondary outcomes were specific postoperative complications, need for reoperation, and in-hospital mortality.
Assessment of study quality
The quality of the included observational studies was assessed by two independent authors (K.S.C. and V.G.S.) using the modified Newcastle–Ottawa scale (Supplementary Table S2). 20 Disagreements between authors were resolved by consensus.
Statistical analyses
Study variables were extracted to Microsoft® Excel 365 (Microsoft, Washington, DC, USA). Results were subsequently transposed to Stata (version 17.0, StataCorp) for the meta-analysis. For studies that performed case matching or propensity score matching, only the data on the matched cohort were recorded and analyzed. Categorical variables are described as n (%), and continuous variables are described as mean ± standard deviation or median (range) unless otherwise specified.
For studies that only expressed median and range/interquartile range (IQR), mean and standard deviation were estimated using methods described by Wan et al. for the quantitative analysis. 21 Dichotomous outcomes were pooled and analyzed using the Mantel–Haenszel method and expressed as odds ratio (OR) with 95% confidence interval (CI). Continuous outcomes were pooled and analyzed using the inverse variance method and expressed as mean difference (MD) with 95% CI. P < .05 was used to define statistical significance.
Heterogeneity was assessed using Cochrane's Q and quantified by I2. Heterogeneity was defined by I2 > 50%. A fixed-effects model was used when I2 ≤ 50%, and a random-effects model using restricted maximum likelihood was used when I2 > 50%. Funnel plots and Egger's regression test were used to test for publication bias. 22 Sensitivity analysis was also performed to identify the presence of any study with a dominant effect. All statistical analyses were reviewed by the senior author (V.G.S.) who has statistical expertise.
Results
The study selection is summarized in the PRISMA diagram (Fig. 1). After screening of titles and abstracts as well as scrutiny of selected full-text articles, four articles were eligible for analysis based on the specified inclusion and exclusion criteria.14,17,18,23 One study used propensity score matching 23 and one performed case matching based on clinical variables. 18 Funnel plots are appended in Supplementary Figure S1. None of the study variables or outcomes showed significant publication bias using Egger's regression test, except for OT (P < .001) and EBL (P = .0355).

PRISMA flowchart for study selection. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study characteristics, patient demographics, and tumor characteristics
The individual study characteristics and patient demographics are summarized in Table 1. A total of 4 studies with 361 patients (3D n = 159, 2D n = 202) were included. There were two retrospective studies,17,23 one prospective study, 14 and one study with both retrospective (2D cohort) and prospective (3D cohort) cohorts . 18 Of the patients, 65.3% were males (overall n = 236/361, 3D n = 98/159 [61.6%], 2D n = 138/202 [68.3%]).
Baseline Characteristics and Patient Demographics of the Included Studies
All continuous variables are expressed in mean ± standard deviation or median (range) unless otherwise stated.
All categorical variables are expressed as n (%) unless otherwise stated.
Values included is this study have been obtained after propensity score/case–control matching.
2D, two-dimensional; 3D, three-dimensional; BMI, body–mass index; NR, not reported; PSM, propensity score-matched.
Demographics (age, sex, body–mass index, incidence of diabetes mellitus, hypertension, hepatitis B carrier, and hepatitis C carrier) and effects of neoadjuvant chemotherapy were comparable between 3D and 2D LLR (Table 2). None of the studies reported on Child–Pugh status. One study reported that 40% (n = 12/30) and 46.7% (n = 21/45) in 3D and 2D LLR groups, respectively, received preoperative portal vein embolization. 17
Summary of Effect Size Comparing the Demographics and Intraoperative and Postoperative Outcomes Between Three-Dimensional and Two-Dimensional Liver Resection in the Included Studies
Odds ratio and 95% confidence interval have been used for dichotomous outcomes, while mean difference and 95% confidence interval have been used for continuous outcomes.
Values that are shown in bold are statistically significant, that is, P < .05.
2D, two-dimensional; 3D, three-dimensional; CI, confidence interval; FE, fixed-effects; I2, heterogeneity; MD, mean difference; NA, not applicable; OR, odds ratio; RE, random-effects.
One study reported comparable preoperative AFP, total bilirubin, and the international normalized ratio between 3D and 2D LLR. 23 Preoperative liver function was comparable between 3D and 2D LLR in studies by Au et al. 23 and Velayutham et al. 18 and was not reported in the studies by Kawai et al. 17 and Qiu et al. 14 (Table 1).
Table 2 summarizes the sample size, effect size, and heterogeneity of the included studies for pooled demographics, histopathological characteristics, and intraoperative and postoperative outcomes. One study exclusively included patients with hepatocellular carcinoma, 23 two studies included a mixed tumor histopathology (Table 3),17,18 and one study did not report on histopathology. 14 Tumor size and incidence of multiple tumors were comparable between 3D and 2D LLR (Table 2).
Histopathological and Intraoperative Characteristics of All Included Studies
All continuous variables are expressed as mean ± standard deviation or median (interquartile range) unless otherwise stated. All categorical variables are expressed as n (%) unless otherwise stated.
Values included is this study have been obtained after propensity score/case–control matching.
2D, two-dimensional; 3D, three-dimensional; CRLM, colorectal cancer with liver metastases; EBL, estimated blood loss; FNH, focal nodular hyperplasia; HCC, hepatocellular carcinoma; NR, not reported; PSM, propensity score-matched; TMN, tumor–node–metastasis.
Intraoperative and postoperative outcomes
Pooled overall OT, EBL, and incidence of open conversion were comparable between 3D and 2D LLR (Table 2; Fig. 2). There was a trend toward lower EBL in 3D LLR; however, it did not reach statistical significance (MD: −454.14 mL, 95% CI: −978.90 to 70.63, P = .09; Fig. 2b). Liver parenchymal transection time (defined as the time from the beginning of liver transection to division of the right hepatic vein) was reported to be shorter by Kawai et al. 17 for 3D LLR compared with 2D LLR (138 ± 25 minutes versus 151 ± 32 minutes, P = .089), but did not reach statistical significance.
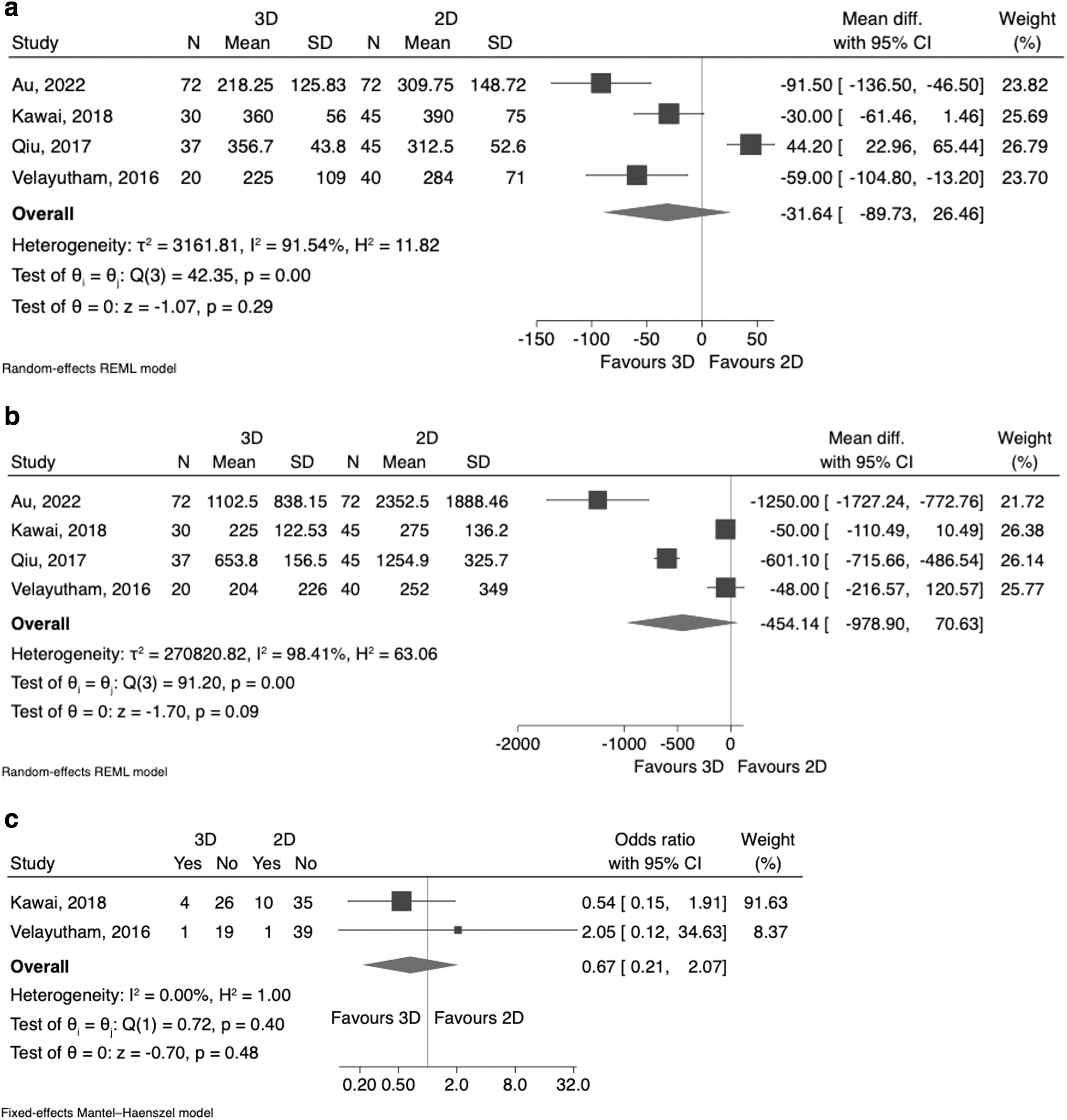
Intraoperative outcomes comparing between 3D and 2D liver resection:
Qiu et al. 14 reported comparable time spent for intrahepatic Glisson's sheath vascular disconnection for the porta hepatis (3D LLR: 42.3 ± 12.5 minutes versus 2D LLR: 35.6 ± 8.9 minutes, P = .723).
The overall incidence of any morbidity was 21.3% (n = 77/361). The incidence of any morbidity was significantly lower in 3D LLR compared with 2D LLR (OR 0.56, 95% CI: 0.32–0.98, P = .04; Fig. 3a). The incidence of major morbidity (Fig. 3b), bile leak/fistula, surgical site infection, PHLF, respiratory complications, need for reoperation, and in-hospital mortality (Fig. 3c) was similar between 3D LLR and 2D LLR. LOS was shorter by 3.36 days (95% CI: −7.55 to 0.83, P = .12) in 3D LLR compared with 2D LLR, but did not reach statistical significance (Fig. 3d).

Postoperative outcomes comparing between 3D and 2D liver resection:
Sensitivity analysis showed that studies by Au et al. 23 and Qiu et al. 14 found a significant effect contributing to significantly lower overall morbidity in 3D LLR (Fig. 4).
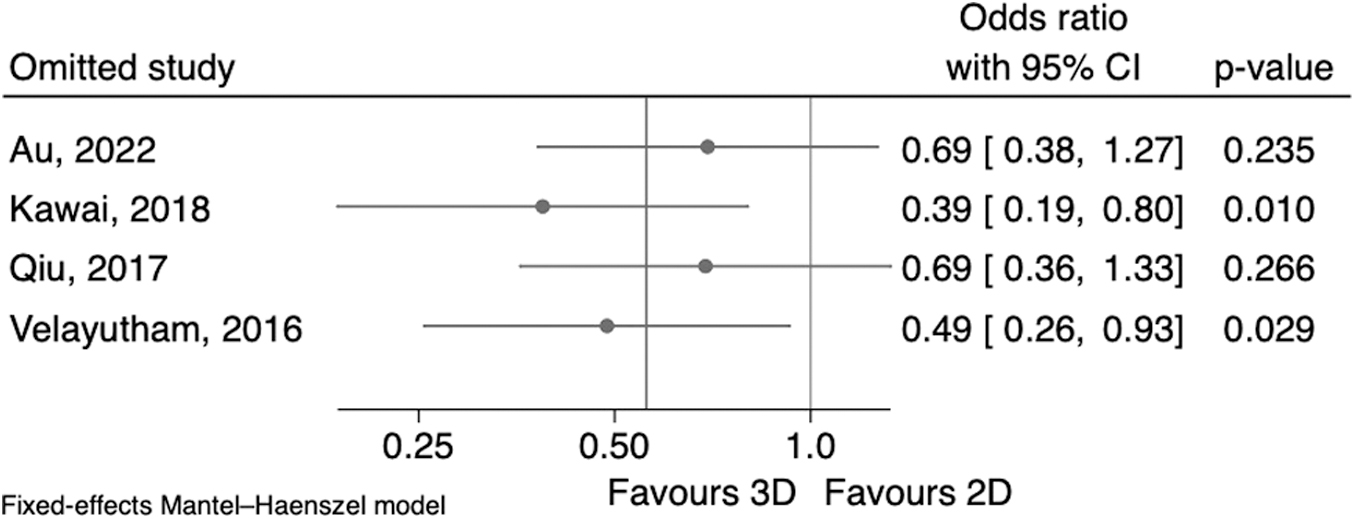
Sensitivity analysis showing the effect of exclusion of individual studies on the overall effect size for overall morbidity. Dark gray line: overall effect size without exclusion of any studies. Light gray line: null effect.
Impact of surgical experience
Two studies reported on the performing surgeon and surgeon's experience.17,18 The same two surgeons performed both 3D and 2D LLR in the study by Kawai et al., 17 and the same single surgeon performed both 3D and 2D LLR in the study by Velayutham et al. 18 Of note, the study period for 3D LLR was later than 2D LLR in both studies.17,18 However, none of the included studies reported on the surgical experience of the performing surgeons.
Discussion
Technological developments and advances in 3D video imaging have shown promising results for 3D laparoscopy.11,12 This is the first systematic review and meta-analysis to compare clinical outcomes between 3D and 2D LLR. This study demonstrated reduced overall postoperative morbidity in 3D LLR. EBL and LOS may be lower in 3D LLR, but the differences were not statistically significant.
2D imaging in surgical laparoscopy is the norm. It is accepted as the standard of care and is considered safe. 3D imaging is relatively new, and data comparing 3D with 2D imaging are emerging. Using an analogy of driving a car, 2D laparoscopy is akin to driving a vehicle with one eye closed, while 3D laparoscopy equates to driving a vehicle with both eyes open. Considering this fact, it can be suggested that 3D laparoscopy should be more precise and safer compared with 2D laparoscopy. However, this remains to be established.
Furthermore, all surgeons are traditionally trained with 2D imaging and have thus already adapted to its limitations. The added depth perception with 3D imaging may not be appreciated or desired by some surgeons. Paradoxically, if 3D imaging is packaged as a part of a robotic platform, it is preferred by surgeons as it comes with the additional benefits of reducing tremors and increasing the range of movements. 8 Many surgeons propose 3D imaging as an advantage of robotic platforms.
However, stand-alone comparison of 3D with 2D imaging is not common due to barriers of availability, accessibility, affordability, and adoption of 3D technology, among others. Embracing the patient-centric safety ethos of health care delivery requires that surgeons come out of their comfort zone and consider adopting 3D imaging. The advantages of using 3D laparoscopy in reducing OT, EBL, and/or postoperative morbidity in gastrectomy and various urological surgeries have been reported.11,12
In laparoscopic gastrectomy, 3D laparoscopy has also been shown to improve lymph node harvest, which may improve oncological outcomes. 11 The 2018 EAES consensus showed that 3D laparoscopy reduces OT and overall postoperative morbidity. However, with regard to the hepato-pancreato-biliary (HPB) system, only one prospective study evaluated the role of 3D versus 2D laparoscopy for liver resection. 14 This calls for an update in evidence to assess the role of 3D laparoscopy in LLR.
One common benefit shown in the meta-analysis of 3D versus 2D laparoscopy in other gastrointestinal or urological surgeries is the reduced OT with 3D laparoscopy.11,12 3D vision allows for a more stereoscopic view, which may aid in identifying critical structures and intraoperative dissection. 24 Easier identification of critical structures allows the operating surgeon to be decisive and may reduce OT. Additionally, this may guide surgeons to quickly identify sources of intraoperative bleeding and limit blood loss, reducing EBL.
This hypothesis is validated by Zu et al. 11 who performed a meta-analysis comparing 3D versus 2D laparoscopic gastrectomy in gastric cancer, showing reduced OT (weighted mean difference [WMD] −16.5, 95% CI: −25.6 to −7.48, P < .001) and EBL (WMD −21.1, 95% CI: −32.2 to −9.9, P < .001). This contradicts our review's findings, where OT was statistically insignificant between 3D LR and 2D LLR. The lack of statistical significance may be due to a small sample size (n = 4 studies with 361 patients) and the inability to detect a small effect. 25
However, while 3D laparoscopy provides clear vision and depth perception, the entire field of vision is decreased and may also result in visual fatigue. 26 The camera assistant may need to adjust the scope more often and this may increase OT. In our experience, in 3D laparoscopy, the lens has a higher likelihood of fogging or smudging over it, which requires cleaning of the lens more often than in 2D laparoscopy due to blurring of the image; this may also increase OT, although less significantly.
In addition, the 3D laparoscopy system camera has a flexible tip, requiring higher skills for the camera assistant to target the area of surgery. It is more common for hospitals to have a majority of camera systems with 2D imaging and only a handful of 3D units, thus increasing the learning curve (LC) due to their limited availability and opportunities for use.
The meta-analysis in the 2018 EAES consensus showed significantly lower OT (MD −11 minutes, 95% CI: −1.72 to −20.29) in 3D laparoscopy. 13 However, 11 minutes may not be clinically significant, especially for longer surgeries of more than 2 hours. Hence, further well-designed prospective studies are required to identify the true effect of 3D laparoscopy on intraoperative outcomes.
The 2018 EAES consensus showed a significant reduction in postoperative complications (relative risk 0.50, 95% CI: 0.25–0.97, P = .04) with 3D laparoscopy in their subgroup analysis of six RCTs on urological and gynecological surgeries (n = 467). 13 Our study similarly showed reduced overall morbidity in the pooled analysis (OR 0.56, 95% CI: 0.32–0.98, P = .04). Pooled demographics and tumor characteristics of the included studies were comparable between 3D LLR and 2D LLR (Table 2).
However, caution should be exercised when interpreting our results for the following reasons. First, included studies were on a heterogeneous group of patients who underwent various extents of hepatectomy. Second, majority (75%) of the included studies were graded as having moderate-quality evidence. Third, this meta-analysis did not analyze prior surgical experience and effect of LC. Of note, the two studies that showed reduced overall morbidity with 3D LLR did not describe the number of surgeons involved and prior surgical experience.14,23
While the study by Au et al. 23 included the same number of cases with “difficult” LLR (defined as a score of ≥7 using the difficulty score based on liver function, tumor size, location, proximity to major vessels, and type of resection) in each group, 27 it is possible that more experienced surgeons performed the “difficult” LLRs. It is also possible that more experienced surgeons performed the “nondifficult” LLRs, resulting in lower overall postoperative morbidity.
Studies that included the same surgeons for both 3D LLR and 2D LLR showed comparable overall morbidity between the two groups.17,18 However, the study period for 3D LLR groups was later compared with 2D LLR groups. While both 2D LLR and 3D LLR involve laparoscopy, 3D laparoscopy requires 3D goggles and a flexible tip camera system. Operating surgeons and assistants will have to adapt to the stereoscopic view and navigation of the 3D laparoscope, which requires a LC.
Headache, dizziness, and blurring of vision have been reported in the first case of 3D laparoscopy by 6 of 9 surgeons who had no prior experience in 3D laparoscopy. 28 However, it is our own experience that surgeons and trainees slowly adapt to the 3D view and symptoms fade away. The LC will likely be shorter for 3D LLR, especially with prior experience in 2D LLR. 29
Studies have shown that the LC for robotic HPB surgeries is shorter compared with laparoscopic HPB surgeries,30,31 which has been suggested to be due to prior surgical experience in laparoscopic surgery as well as the benefits conferred by the robotic platform. 8
Chua et al. 30 reported that a median of 17 cases (IQR 16–20) was required for robotic minor and major LR, which was 47.1% lower than LLR. Studies by Kawai et al. 17 and Velayutham et al. 18 included 30 and 20 patients who underwent 3D LLR, respectively. We need to determine whether the LC has been overcome in these studies during the 3D LLR. The lack of significant effect on improvement in postoperative morbidity with 3D LLR may be due to the surgery being performed during the initial LC. However, 3D laparoscopy has been reported to have good outcomes even during the initial experience.
Tan et al. 32 reported no open conversion, readmission, or mortality in 27 consecutive patients who underwent laparoscopic common bile duct exploration using 3D laparoscopy, followed by primary repair with barbed suture; only 1 patient (4%) had bile leak and retained stone. Sinha et al. 29 reported a LC of <5 cases for 3D laparoscopy in gynecological surgeries.
Our study did show better overall postoperative morbidity in 3D LLR in the pooled analysis. However, more evidence is necessary in view of the small sample size in our meta-analysis and the considerations as described above. In our view, despite its benefits, the current 3D imaging technology has substantial limitations that pose an impediment to its widespread adoption (Fig. 5).

Benefits and limitations of widespread adoption of 3D laparoscopy in clinical practice. 3D, three-dimensional; SGD, Singapore dollars.
There are strengths and limitations to this study. This is the first study to compare outcomes between 3D LLR and 2D LLR. This is especially relevant with the recent 2018 EAES consensus advocating using 3D LLR to reduce OT and potentially reduce postoperative morbidity. 13 Although pooled demographics were comparable in all included studies, there was a lack of studies evaluating postoperative outcomes for HPB surgeries.
Our study has its limitations. First, a small number of included studies with small sample sizes limit the accuracy of results. Second, only one of the included studies was of high methodological quality. Third, included studies had heterogeneous study populations (e.g., patients with various extents of LR and underlying histopathology) and did not consider the effect of the initial LC for 3D LLR. Last, only short-term postoperative outcomes were reported, and oncological outcomes such as overall and disease-free survival were not studied.
Conclusions
3D LLR may reduce overall postoperative morbidity compared with 2D LLR. However, this result may be confounded by the initial LC of 3D LLR and the lack of standardization of surgeons' experience. OT, EBL, open conversion rate, and other postoperative outcomes were comparable between 3D and 2D LLR.
Further well-designed studies, possibly including cost analysis, are necessary to establish whether 3D LLR has clinical gains over 2D LLR.
Footnotes
Authors' Contributions
K.S.C. conceptualized the study and performed the literature search, data collection, data analysis, and writing of the original article.
V.G.S. performed the literature search, data collection, data analysis, and revision of the article and supervised the entire study.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.