
Abstract
Background:
Hilar cholangiocarcinoma (HCCA) has a high degree of malignancy and poor prognosis, and the best long-term prognosis can only be achieved by radical resection. However, the surgical steps are complicated, and the operating space is limited, making it hard to complete laparoscopically. So our team proposes a new surgical approach for laparoscopic left-liver-first anterior radical modular orthotopic right hemihepatectomy (Lap-Larmorh). In this way, we can simplify the operation steps and reduce the difficulty.
Materials and Methods:
We recorded and analyzed the clinical data of 26 patients with type IIIa HCCA, who underwent laparoscopic radical resection in our department from December 2018 to January 2023. According to the laparoscopic surgical approach, we divided the patients into the new approach (NA) group (n = 14) using the Lap-Lamorh and the traditional approach (TA) group (n = 12) not using the Lap-Lamorh.
Results:
All surgeries in this study were completed laparoscopically with no conversion to open surgery. The operation time in the NA group and TA group had statistically significant differences, which was 372.5 (332.8, 420.0) minutes versus 423.5 (385.8, 498.8) minutes (P = .019). The two groups showed no significant difference in other characteristics (P > .05). Only 1 patient suffered from transient liver failure due to portal vein thrombosis. Patients with pleural effusion or ascites were cured by catheter drainage and enhanced nutrition.
Conclusion:
Lap-Larmorh reduces the difficulty of serving the vessels at the second and third hepatic hilum by splitting the right and left livers early intraoperatively. The new approach is more suitable for the narrow space of laparoscopic surgery and reflects the no-touch principle of oncology.
Introduction
According to anatomic location, cholangiocarcinoma can be divided into intrahepatic, hilar, and extrahepatic types. The most common type is hilar cholangiocarcinoma (HCCA), or Klatskin tumor, which accounts for about two-thirds of cholangiocarcinoma. 1 It has a high degree of malignancy and poor prognosis, and the best long-term prognosis can only be achieved by radical resection. 2 It has been reported that the 1-year and 5-year survival rates after R0 resection are 72.4% and 30.4%. 3
Chen et al. reported 1-, 3-, and 5-year survival rates of 80%, 42%, and 27% in patients with HCCA who underwent major hepatectomy. 4 Radical resection of Bismuth IIIa HCCA requires resection of the right liver and caudate lobe. The key to the operation is to confirm intraoperatively that the tumor does not invade the left hepatic vessels and to ensure R0 resection with sufficient future liver remnant (FLR). However, in laparoscopic surgery, when the right perihepatic ligament and caudate lobe are first dissociated according to conventional surgical procedures, the operation space is limited, which makes it challenging to complete laparoscopically. Moreover, it is easy to tear the short hepatic veins when pulling the right liver and exposing the third hepatic hilum.
To simplify laparoscopic surgical procedures, our team proposed a new approach for laparoscopic left-liver-first anterior radical modular orthotopic right hepatectomy (Lap-Larmorh). The innovative point of the new approach is to split the left and right liver after severing the right hepatic vessels, thus exposing the deep caudate lobe and inferior vena cava (IVC) to the surgical field. The shallow operation area makes cutting off the short hepatic vessels and the right hepatic vein (RHV) more convenient. The right perihepatic ligament is dissociated after the resection of the right liver and caudate lobe. Furthermore, the application of the new approach has achieved good results so far, and the report is as follows.
Materials and Methods
Initial population
We recorded and analyzed the clinical data of 26 patients with type IIIa HCCA who underwent laparoscopic radical resection in our department from December 2018 to January 2023. According to the laparoscopic surgical approach, we divided the patients into the new approach (NA) group (n = 14) using the Lap-Lamorh and the traditional approach (TA) group (n = 12) not using the Lap-Lamorh. All surgeries were performed by the same surgical team. Inclusion criteria were as follows: (1) All patients were diagnosed with Bismuth-Corlette IIIa HCCA by contrast-enhanced computed tomography (CECT) or magnetic resonance imaging of the upper abdomen before surgery.
Patients suspected of lymph node metastasis underwent positron emission tomography/computed tomography (PET/CT) to confirm no distant metastasis; (2) all patients underwent preoperative three-dimensional (3D) reconstruction of the liver, ensuring that FLR is >30% in patients with normal liver function and >40% in patients with obstructive jaundice or cirrhosis; (3) the general condition was good and could tolerate surgery. Exclusion criteria were as follows: Patients with distant metastasis, insufficient FLR, poor general condition, and unclear preoperative diagnosis were excluded from the study.
The study was approved by the Ethics Committee of the Second Hospital of Hebei Medical University (No. 2022-R740). Written informed consent to participate was waived for its retrospective nature, and the data set was deidentified to protect patient privacy.
Preoperative preparation
After admission, the preoperative examination was completed, and the possible blood electrolyte disorders were corrected. When preoperative serum total bilirubin (TBIL) was >170 μmol/L, we performed percutaneous transhepatic cholangial drainage (PTCD) to relieve jaundice, and surgery after serum TBIL was <100 μmol/L. Patients with serum albumin <35 g/L were given intermittent human serum albumin and adequate nutritional support. For patients with a smoking history, atomization therapy was given before surgery to reduce the risk of postoperative pulmonary infection.
Surgical procedures
Body position and trocar distribution
After successful anesthesia, the patient was placed supine with legs apart, and the head was elevated 30°. The surgeon was positioned on the patient's right side, and the assistant and endoscopic operator were separated on the left side and between the legs. A 10 mm trocar was placed 1 cm below the umbilicus as an observation hole, followed by abdominal exploration to exclude intraperitoneal metastasis. The remaining four trocars were distributed around the observation hole in a V-shape. And the pneumoperitoneum pressure was maintained at 12–15 mmHg and adjusted according to intraoperative needs.
Resection of specimens
After abdominal exploration, the Kocher maneuver was used to dissociate the duodenum. The No. 13 lymph nodes were then excised, and an intraoperative frozen section (IFS) was performed. Patients with positive No.13 lymph nodes were further removed with No.16 lymph nodes. Radical surgery would be abandoned if the No. 16 lymph nodes were still positive. Then, the common bile duct (CBD) was dissected and severed against the upper edge of the pancreas. Radical resection of HCCA was performed in the patient with a negative margin of the stump of the CBD. However, if the margin of CBD was positive, laparoscopic pancreaticoduodenectomy should be combined when the margin of left hepatic duct (LHD) was also negative.
The hepatoduodenal ligament was resected from the foot side along the longitudinal axis of the hepatic artery (Fig. 1A), and No. 3, 5, 7, 8, and 9 lymph nodes were resected en bloc. After confirming that the left hepatic artery and the left portal vein were not invaded, the roots of the right hepatic artery and the right portal vein were dissected and severed (Fig. 1B, G). The LHD was severed with scissors, and the stump was sent for IFS to ensure R0 resection. Then, the pre-resection line was marked along the ischemic line on the liver surface.
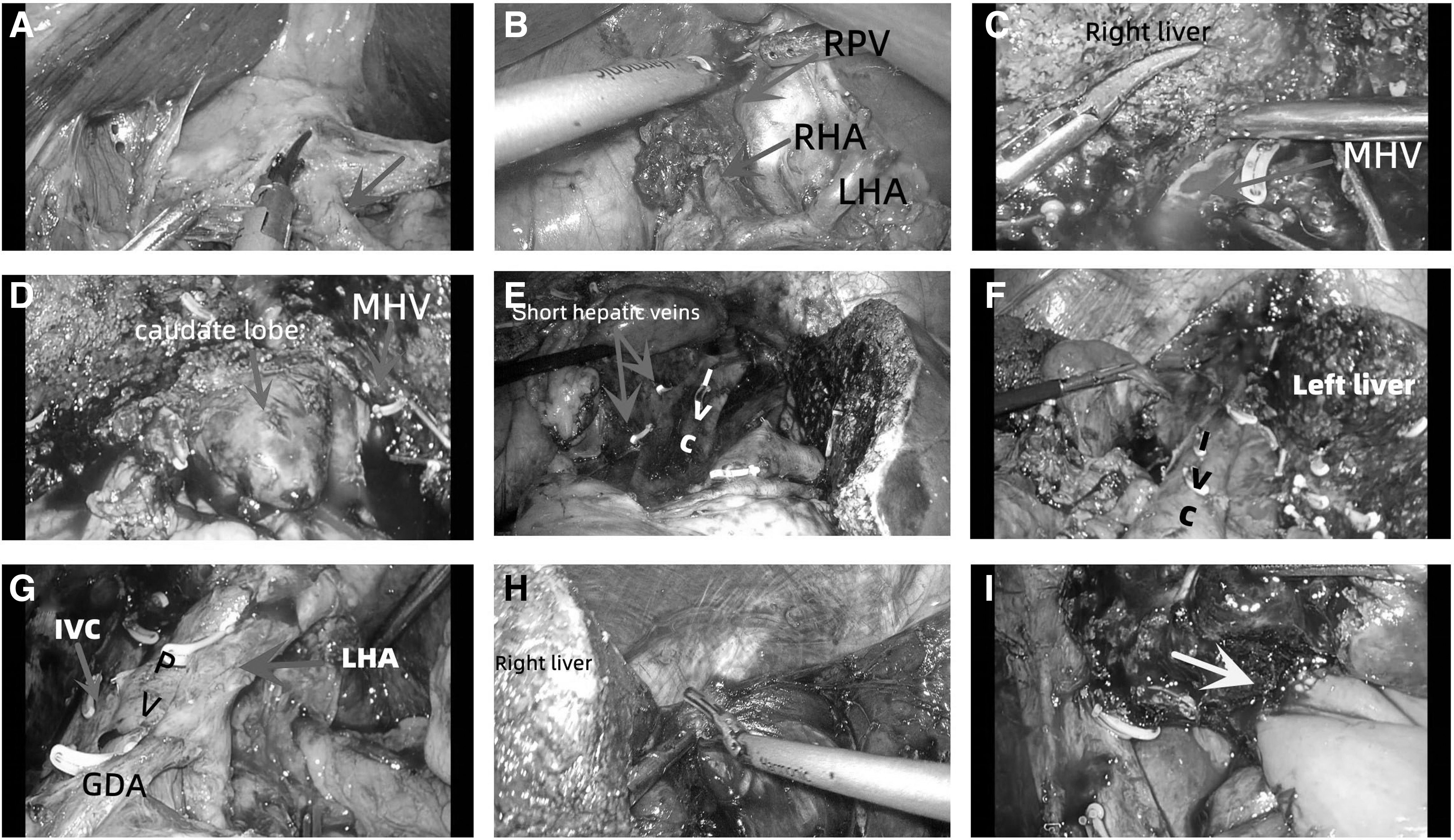
The critical steps in Lap-Larmorh for Bismuth IIIa HCCA.
Next, the left and right liver were split by dividing the liver parenchyma along the right edge of the middle hepatic vein and the pre-resection line using an ultrasonic scalpel (Fig. 1C). At this time, the left and right liver were naturally separated, and after pushing the left liver to the left side of the abdominal cavity, the deep caudate lobe and the anterior space of the IVC were exposed (Fig. 1D). Then the short hepatic veins and the RHV were dissected, and the caudate lobe was excised (Fig. 1E–G). Finally, the right perihepatic ligament was dissociated to complete radical resection (Fig. 1H).
Cholangiojejunostomy
The continuous suture was used for mucosa-to-mucosa cholangiojejunostomy (Supplementary Video S1). We used two 4-0 absorbable sutures to successively suture the posterior and anterior walls of the anastomosis (Fig. 1I), and Roux-en-Y reconstruction was performed afterward. Finally, the falciform ligament of the left liver was fixed by an absorbable suture to avoid postoperative rotation and displacement of the left liver. After placing drainage tubes behind the cholangiojejunostomy anastomosis and beside the liver, the operation was completed.
Chemotherapy
One month after discharge, the patients were treated with the chemotherapy regimen of tegafur (S-1), gemcitabine, and oxaliplatin.
Follow-up and statistical analyses
After discharge, patients were followed up by telephone or as outpatient. The patients were instructed to review CECT and tumor markers 3 months after surgery. SPSS 26.0 software and R software were used to process data. The normal distribution measurement data are expressed as (
Results
All surgeries in this study were completed laparoscopically with no conversion to open surgery (Tables 1–3.). Four patients received PTCD, respectively, in each group. The operation time in the NA group and TA group had statistically significant differences, which was 372.5 (332.8, 420.0) minutes versus 423.5 (385.8, 498.8) minutes (P = .019). The two groups showed no significant difference in age, FLR, TBIL, estimated blood loss, the incidence of postoperative complications, and so on (P > .05). In the NA group, one patient suffered from portal vein thrombosis (PVT), which caused transient liver failure and was relieved after anticoagulant therapy. Patients with pleural effusion or ascites were cured by catheter drainage and enhanced nutrition. The 1-year survival rates were 77.9% in the NA group and 83.3% in the TA group (Fig. 2), and the 3-year survival rates were 40.1% in the NA group and 31.2% in the TA group (P = .81).
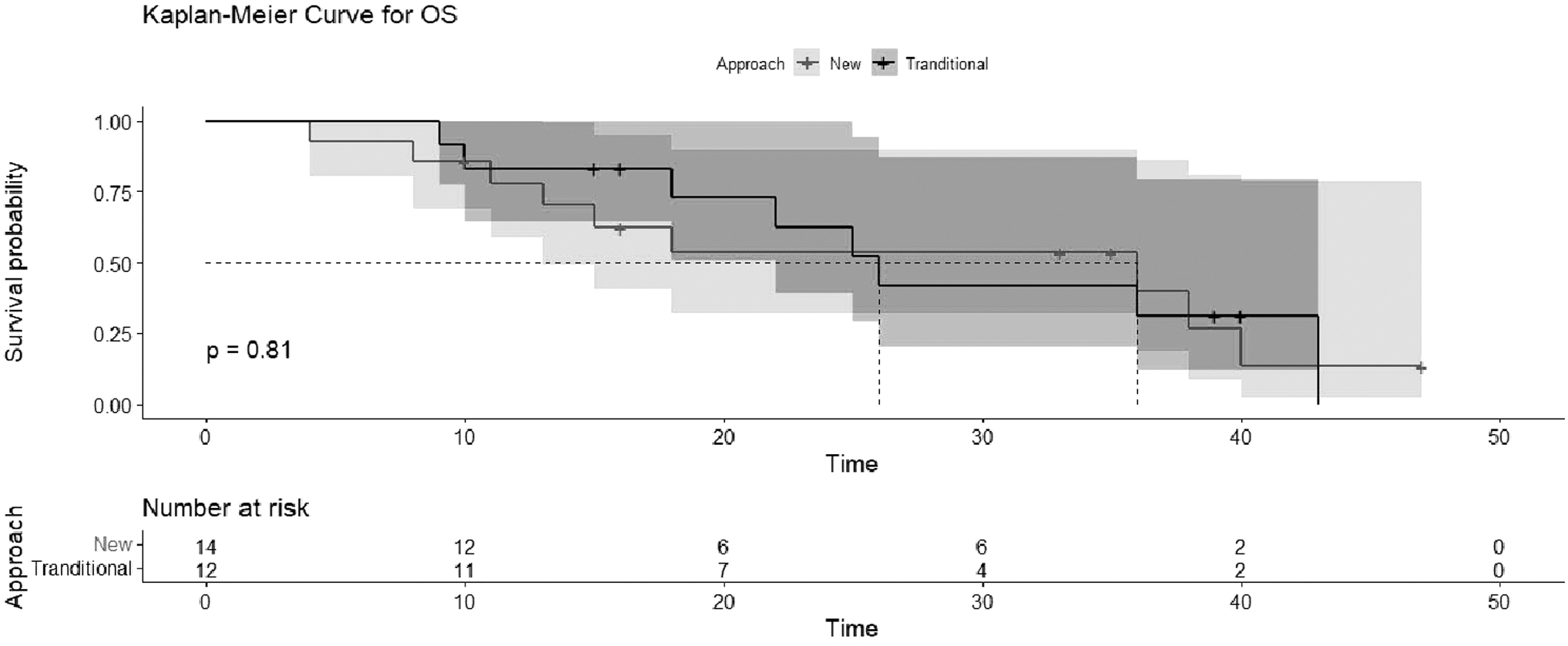
Overall survival of patients in the new approach group and traditional groups. The 1-year and 3-year survival rate was 77.9% and 40.1%, and 83.3% and 31.2% for traditional group.
Preoperative Characteristics
ALB, albumin; ASA, American Society of Anesthesiologists classification; BMI, body mass index; FLR, future liver remnant; NA, new approach; PTCD, percutaneous transhepatic cholangial drainage; TA, traditional approach.
Intraoperative Indicators
NA, new approach; TA, traditional approach.
Postoperative Characteristics
AJCC, American Joint Committee on Cancer; NA, new approach; PVT, port vein thrombosis; TA, traditional approach.
Discussion
A study in 2015 shows that combined caudate lobectomy can improve the rate of R0 resection. 5 In our center, except for type 1 HCCA, the caudate lobe is removed during radical operation. Most current reports on laparoscopic radical resection of HCCA are limited to removing bile ducts, but few are on hepatectomy and lymph node dissection.6,7 When the radical resection of type IIIa is performed by laparotomy, the top-down view is not conducive to severing the third hepatic hilum. After the right liver is mobilized, the short hepatic veins and IVC are exposed by pulling the right liver to the assistant.
However, in laparoscopic surgery, the operating space is small due to the limitation of the thorax. Dissociating the right perihepatic ligament and transecting the short hepatic veins first is challenging. Moreover, frequent compression of the right liver during the above steps may increase the risk of tumor cell dissemination, contrary to the no-touch principle of oncology. 8
Therefore, to solve the above shortcomings, we propose a new approach of Lap-Larmorh (Supplementary Video S2). The improvements in surgical procedures are as follows: (1) Prioritize dissection and protection of the left hepatic vessels to reduce the risk of accidental injury during operation. Moreover, the right hepatic vessels are not overdissected to reduce contact with the tumor; (2) after the right hepatic vessels and LHD are severed, the left and right livers are preferentially split. (3) Finally, the right perihepatic ligament is dissociated.
The advantages of the new approach are also apparent: (1) Preferentially, dissecting the left hepatic vessels can detect possible tumor invasion early and clarify the necessity of radical surgery. It can also protect the left hepatic vessels preventively in the early stage of surgery to avoid intraoperative accidental injury causing liver failure. (2) Disconnection of the right hepatic vessels before hepatectomy can reduce intraoperative blood loss and the risk of tumor dissemination. (3) Also, after separating the left liver from the surrounding liver, the left and right liver will be naturally separated.
Then the left liver is pushed to the left side, and the caudate lobe and the anterior space of the IVC are fully exposed to the surgical field. It is more convenient for the resection of the caudate lobe and the transection of the short hepatic veins, reducing the surgical difficulty. (4) After the blood vessels of the right liver and caudate lobe are severed, the overall operating space is enlarged. It also makes it easy to free the perihepatic ligament, avoiding the compression of the right liver when the perihepatic ligament is preferentially dissociated.
HCCA is characterized by infiltrating growth. 9 Moreover, due to the late onset of symptoms, 10 vascular invasion and metastasis are common at diagnosis, leading to poor prognosis. Studies have shown that R0 resection can improve the postoperative survival rate.11,12 However, there was a high vascular and biliary variation rate in the first hepatic hilum. To achieve R0 resection, an adequate preoperative examination is necessary.
3D reconstruction of the liver can provide a multiangle view of the tumor and surrounding tissue. Vascular and biliary variations can be detected in advance, and FLR can be accurately calculated. This provides strong evidence for the formulation of a surgical plan. All patients in this study underwent preoperative 3D reconstruction to ensure FLR >40% in patients with jaundice or cirrhosis and >30% in patients with normal liver function. It can effectively avoid liver failure caused by intraoperative vascular injury and postoperative liver volume deficiency.
Studies have shown that elevated serum TBIL will negatively affect liver function and regeneration, increasing the rate of postoperative complication and mortality.13,14 In addition, jaundice can also damage the intestinal barrier and cause gut-derived infection. 15 Therefore, biliary drainage is necessary for patients with preoperative jaundice. There are two main techniques of biliary drainage: PTCD and Endoscopic Nasobiliary Drainage (ENBD). PTCD can make the liver on the drainage side grow compensatory, which is beneficial to the recovery of liver function. 16
Some studies have also shown that it can improve postoperative survival rate. 17 In addition, compared with ENBD, the risk of complications related to PTCD is lower.18,19 Although PTCD has the risk of planting transfer, 20 planting transfer has yet to occur in the reports of some scholars21,22 and our department. And ENBD has a poor drainage effect on the obstructed side of the liver, 23 and the drainage tube left in the CBD for a long time is likely to cause inflammation in the surrounding tissues. It increases the difficulty of lymph node dissection and affects the intraoperative judgment of tumor resectability, 24 so we rarely use it.
Our center prefers to perform PTCD to reduce serum TBIL levels in jaundice patients. The practice of PTCD in our center is to prioritize drainage of the left hepatic bile duct and determine whether to perform simultaneous drainage of the right bile duct based on the degree of dilation of the right bile duct. If the TBIL is below 100 μmol/L after 2 weeks, the operation should be performed. However, if the TBIL decreases slowly after drainage, the drainage time will be extended.
In conclusion, compared with the TA group in the early stage of radical operation for type IIIa HCCA, patients receiving the new approach had significantly shorter operation times, and the difference was statistically significant. And the operation time of type IIIa was also shorter compared with the other centers.25,26 Although the intraoperative blood loss in the NA group was less than that in the TA group, there was no statistical difference. In terms of postoperative complications, in this study, only 1 patient who suffered from transient liver failure due to postoperative PVT. Furthermore, complications such as abdominal effusion and pleural effusion disappeared after catheter drainage and nutritional support.
Conclusion
This study preliminarily verified the safety and efficacy of the new approach. Lap-Larmorh reduces the difficulty of serving the vessels at the second and third hepatic hilum by splitting the right and left livers early intraoperatively. The improvement of the radical operation of type IIIa HCCA is more suitable for the narrow space of laparoscopic surgery and reflects the no-touch principle of oncology.
Footnotes
Authors' Contributions
X.Z. and A.L. were responsible for data collection and organization. J.L. was responsible for the interpretation of imaging data. X.L. and Z.H. wrote the final article. H.X. and L.S. were responsible for the follow-up. J.L. designed this study. The other authors participated in the surgery. The authors have all read and approved this final article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.