
Abstract
Objective:
This study aimed to investigate the feasibility, efficacy, and safety of laparoscopic transabdominal preperitoneal (TAPP) repair in the treatment of inguinal hernia in patients on peritoneal dialysis, and the optimal timing for initiating postoperative peritoneal dialysis.
Methods:
We conducted a retrospective analysis of the clinical data pertaining to patients on peritoneal dialysis with inguinal hernias treated with TAPP repair in the First Affiliated Hospital of Shandong First Medical University from July 15, 2020 to December 15, 2022. Follow-up observations of the treatment effect were also analyzed.
Results:
A total of 15 patients underwent TAPP repair with success. Contralateral occult hernias were found in 3 cases intraoperatively and were treated simultaneously. During the operation, it was found that the peritoneal dialysis tube was completely wrapped in the omentum majus in 1 case and incompletely wrapped in 5 cases and was separated smoothly under laparoscopy.
Conclusion:
For patients on peritoneal dialysis with inguinal hernia, TAPP repair has the advantages of less trauma, simultaneous treatment of contralateral occult hernias, adjustment and fixation of peritoneal dialysis tubes, lower incision complication rates, and lower recurrence rates, compared with open surgery. With the gradual resumption of peritoneal dialysis 7 days postoperatively, TAPP repair can be performed safely and effectively in this population group; thus it is a procedure worth promoting.
Introduction
Chronic kidney disease incidence is a growing global health concern, with a considerable number of new and existing patients requiring dialysis annually, specifically for end-stage disease. Continuous ambulatory peritoneal dialysis (CAPD) is a widely accepted alternative to hemodialysis for patients with end-stage renal failure. It has the advantages of protecting residual renal function, maintaining circulatory stability, and having high economic value and ease of application.1–3 The increase of intra-abdominal pressure from continuous peritoneal dialysate infusion (2000 mL/time, 4–6 times per day, 4–6 hours per time) is a major cause of inguinal hernia.4–7 As the duration of peritoneal dialysis is prolonged, inguinal herniation may gradually increase in severity, leading to risk of hernia content chimerism and necrosis. As these conditions can be life-threatening, timely intervention is critical, especially for early-stage CAPD patients.
In the past, open surgeries, such as Lichtenstein, were preferred for inguinal hernia repair complicated by peritoneal dialysis. 8 However, open surgery has many shortcomings, such as large trauma, slow recovery, more incision complications, and inability to simultaneously treat contralateral occult hernias. 9 With the development of laparoscopy, transabdominal preperitoneal (TAPP) repair has become the main method of inguinal hernia repair, with the advantages of less trauma, lower recurrence rates, fewer wound complications, and the ability to deal with occult hernias simultaneously .9–11 For patients on peritoneal dialysis with inguinal hernia, laparoscopic techniques can be used to adjust and fix the peritoneal dialysis tube at the same time to ensure optimal dialysis. However, TAPP repair involves cutting the peritoneum, dissociating the myopectineal orifice, placing a mesh, and then closing the peritoneum.
Once the dialysate enters the repair area through the peritoneal incision, it can inevitably affect the mesh and surrounding tissues, leading to serious consequences such as mesh infection and hernia recurrence. Therefore, this study aimed to investigate the feasibility, efficacy, and safety of laparoscopic techniques for treating inguinal hernias in patients on peritoneal dialysis and to determine the optimal timing to resume peritoneal dialysis after surgery.
Methods
The study was approved by our Ethics Committee and was conducted in accordance with the Declaration of Helsinki. Owing to the retrospective nature of the study, written informed consent from the enrolled patients was not required. We retrospectively analyzed the clinical data of 15 patients on peritoneal dialysis with inguinal hernia who underwent laparoscopic surgery in the First Affiliated Hospital of Shandong First Medical University from July 15, 2020 to December 15, 2022. All patients were diagnosed with inguinal hernia by physical examination and ultrasound during a period of peritoneal dialysis. The patients' age, sex, type of inguinal hernia, catheter insertion time, operation time, blood loss, and perioperative complications were recorded in detail. The patients were followed up every month after the operation to record whether there was chronic pain or recurrence of inguinal hernia.
Preoperative management
Routine preoperative assessment included evaluations of the patient's cardiopulmonary function, a complete auxiliary examination to further eliminate surgical contraindications, cessation of peritoneal dialysis 24 hours before surgery, change to hemodialysis, drainage of any abdominal fluid to the greatest extent practical, nutrition support, renal function medications, and other symptomatic treatment as needed.
Surgical procedures
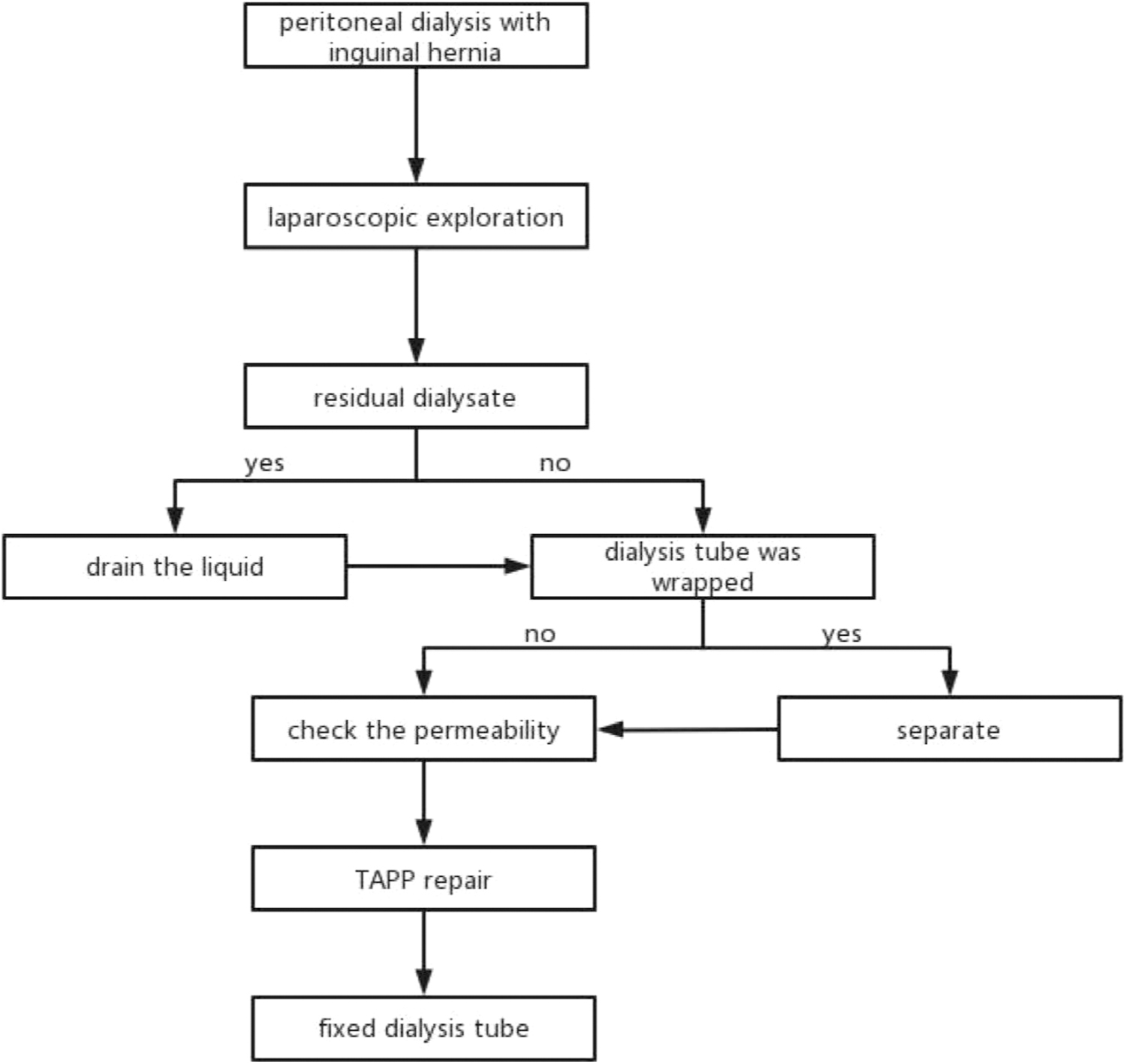
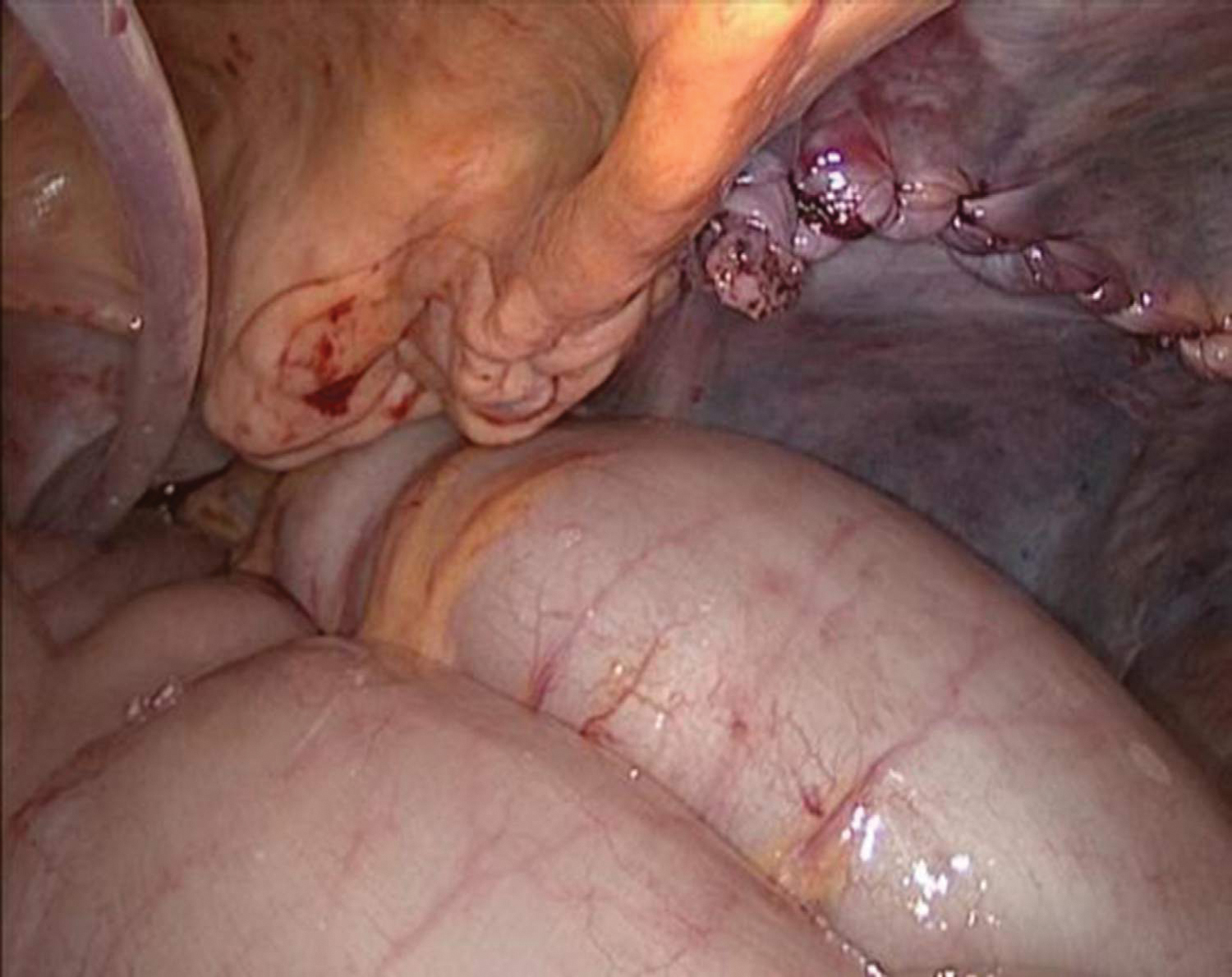
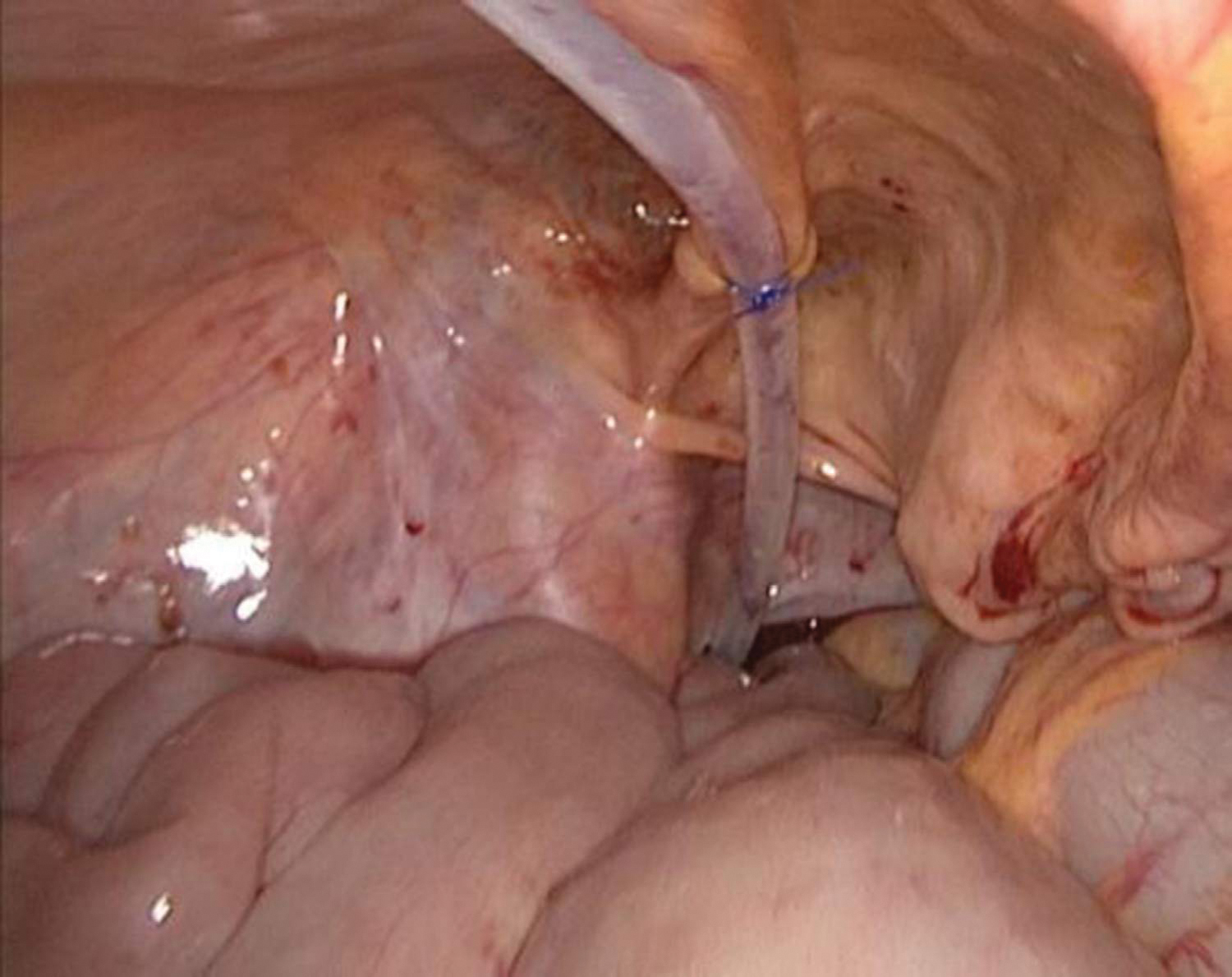
Urinary catheters were placed in all patients preoperatively to avoid bladder filling (Fig. 1). After the patient was successfully anesthetized, the laparoscope and operating instruments were readied. First, an investigation was carried out to determine whether any contralateral occult hernias or residual dialysate in the abdominal cavity were present (Fig. 2). If residual dialysate was present, an aspirator was used to drain the liquid. If the peritoneal dialysis tube was wrapped in the omentum majus, the dialysis tube was separated from the omentum majus (Fig. 3), and its permeability was checked (Fig. 4). Subsequently, TAPP repair was routinely performed. The hernia sac was fully returned during the operation to avoid peritoneal damage. A mesh was placed and fixed with hernia fixing glue. Absorbable sutures were used to continuously suture the peritoneum and close it tightly (Fig. 5).
Surgical procedures.
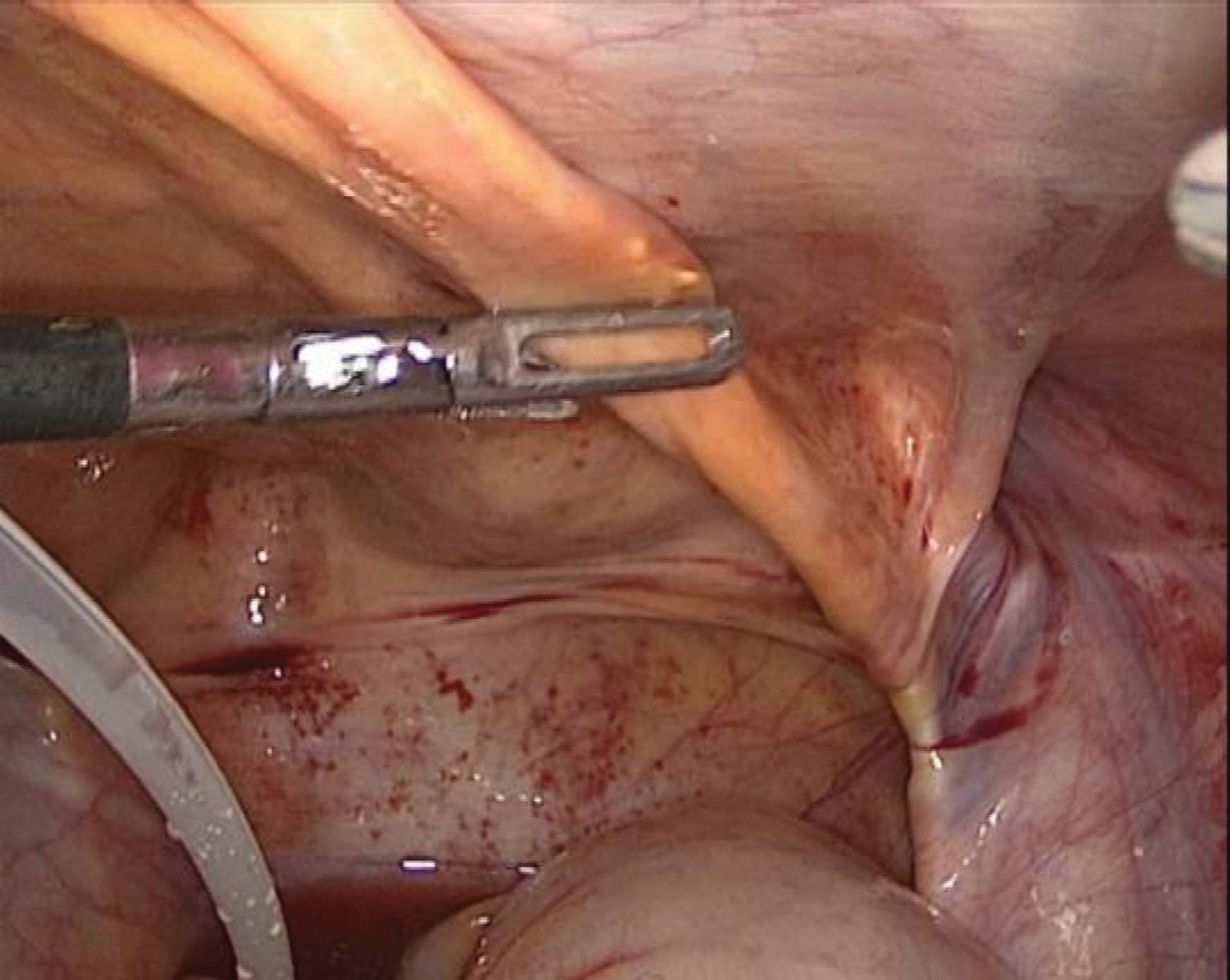
Explore dialysis tube and inguinal hernia.
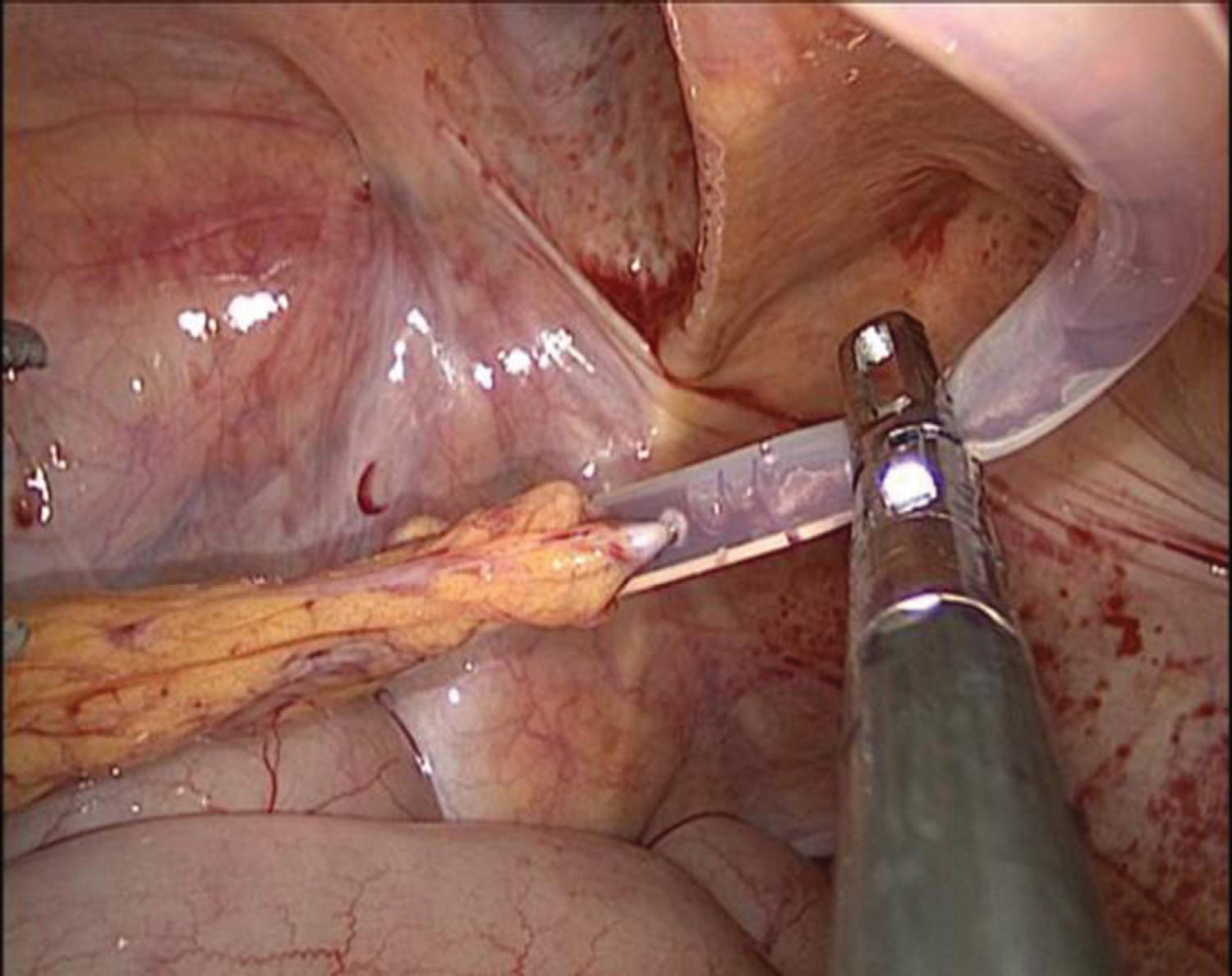
Separation of dialysis tube from omentum majus.
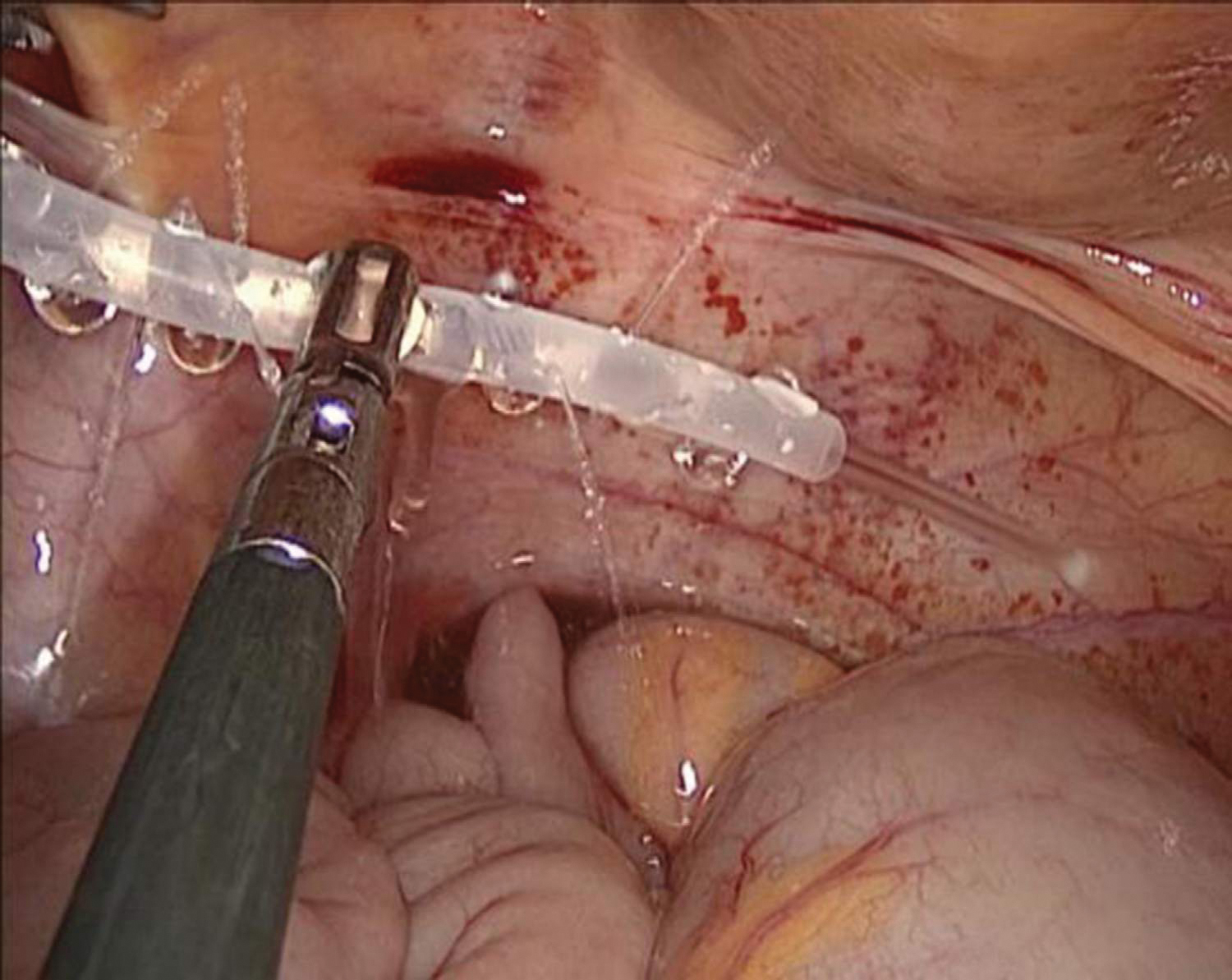
Check the permeability of dialysis tube.
Inguinal hernia has been repaired.
Any peritoneal damage, if present, was closed. Any contralateral occult hernias were treated simultaneously. After repairing the inguinal hernia, the end of the peritoneal dialysis tube was placed into the excavatio rectovesicalis and fixed in the median umbilical fold with a nonabsorbable suture to prevent displacement (Fig. 6). The operation was deemed complete if no active bleeding was found.
Dialysis tube has been fixed.
Postoperative management
All patients continued to receive symptomatic treatment such as nutritional support, drug protection of renal function, and local compression to prevent mesh displacement, pain reduction, and seroma prevention. All patients were changed to hemodialysis after the operation. On the 7th day postop, low-dose peritoneal dialysis (0.5–1 L each time, 4–6 times a day) was started. If no discomfort was observed, the original peritoneal dialysis program was gradually resumed 7 days later. All patients were discharged within 10–12 days of the operation. Telephone follow-up was carried out every month, and ultrasound examination was performed to check for hernia recurrence at 1, 6, 12, and 24 months postoperatively.
Results
From July 15, 2020 to December 15, 2022, a total of 15 patients on peritoneal dialysis with inguinal hernia underwent TAPP repair without conversion to open surgery. Among the 15 patients, 13 were men and 2 were women, with a mean age of 57.47 ± 11.41 years. The mean duration of peritoneal dialysis before the operation was 8.06 ± 6.18 months. Contralateral occult hernias were found in 3 patients intraoperatively and were treated simultaneously. During exploration, it was found that the dialysis tube was wrapped in the omentum majus in 6 patients. After separation of the adhesion, it was confirmed that the dialysis tube was unobstructed and could continue to be used.
One patient developed seroma postoperatively and recovered after conservative treatment. No patients had hematoma or wound/mesh infection. In the mean follow-up time of 11.33 ± 7.55 months, no patients experienced a recurrence of inguinal hernia. One patient died unexpectedly due to a car accident 3 weeks after the operation. One patient stopped peritoneal dialysis after kidney transplantation due to progressive renal failure 8 months after the operation. All other patients had unobstructed peritoneal dialysis tubes and successful peritoneal dialysis (Table 1).
Basic Characteristics and Therapeutic Effect in 15 Patients
BIH, bilateral inguinal hernia; UIH, unilateral inguinal hernia.
Discussion
Abdominal hernia is a common complication of CAPD, accounting for 60.4% of all associated complications; inguinal hernias specifically account for 24.9%. 12 The primary reason for inguinal hernia in CAPD is the continuous increase of intra-abdominal pressure caused by dialysate injection into the abdominal cavity, in addition to potential negative nitrogen balance associated with renal failure. Following hernia onset, patients often cease CAPD but may also experience potentially life-threatening effects, such as groin area swelling and incarceration or strangulation of hernia contents. Therefore, hernia occurrence merits rapid intervention.
Lichtenstein has the advantage of ensuring the integrity of the peritoneum and avoiding the recurrence of inguinal hernia caused by leakage of dialysate when the patient resumes CAPD after surgery. According to the author's clinical experience, the time of peritoneal healing is ∼7 days. After TAPP repair, it is safe to change to hemodialysis, start small dose peritoneal dialysis (0.5–1 L each time, 4–6 times a day) on day 7 postop, and gradually transition to the original peritoneal dialysis program. This approach can avoid complications such as mesh infection and hernia recurrence caused by peritoneal incision dialysis fluid entering the repaired area. In this study, 15 patients underwent TAPP repair, and no patient experienced a recurrence of inguinal hernia after gradually resuming peritoneal dialysis. Although ascites is a contraindication of TAPP repair, unlike ascites due to cirrhosis, the peritoneal dialysis fluid is controllable and will not affect the operation.
The physical condition of patients on peritoneal dialysis is generally poor. The trauma caused by the Lichtenstein operation in this patient population is greater than that caused in healthy people, and wound complications are relatively higher. 4 In contrast, TAPP repairs are associated with less trauma, faster postoperative recovery, fewer wound complications, and lower recurrence rates.13,14 Moreover, these advantages are more pronounced in patients undergoing peritoneal dialysis. In addition, 3 out of 13 patients diagnosed with unilateral inguinal hernias preoperatively were also found to have contralateral occult hernias. If left untreated, occult hernias can progress rapidly when peritoneal dialysis is resumed, resulting in the patient requiring further operation. TAPP repair can be used to detect the presence of such occult hernias and allow them to be treated simultaneously, thus avoiding subsequent operation.
In this study, one patient had a recurrent hernia after the Lichtenstein operation. The recurrence rate is high, and the damage is great when open repair is performed again, TAPP repairs can completely repair the myopectineal orifice, with less pain, fewer side injuries, and lower recurrence rates. 15 Therefore, TAPP repair is more suitable for patients on peritoneal dialysis with recurrent inguinal hernias.
Compared with totally extraperitoneal repair, TAPP repair can also explore the placement of dialysis tubes. If the dialysis tube is wrapped in the omentum majus, the adhesion can be separated under laparoscope, and it can be determined whether the dialysis tube is unobstructed. The end of the peritoneal dialysis tube can then be placed in the excavatio rectovesicalis and fixed in the median umbilical fold to prevent displacement, which prolongs the usage time of the dialysis tube and is more conducive to subsequent peritoneal dialysis treatment. In this study, the peritoneal dialysis tube was found to be wrapped in the omentum majus in 6 patients and was subsequently separated during the operation. This allowed for the dialysis tubes to be adjusted and fixed in all patients. Follow-up showed that all patients had unobstructed dialysis tubes and successful peritoneal dialysis.
In conclusion, if peritoneal dialysis is resumed incrementally and gradually postoperatively (starting with a low dose of 0.5–1 L each time, 4–6 times a day from day 7 postop), TAPP repair is a safe, effective, and feasible treatment for inguinal hernias in patients on peritoneal dialysis. The biggest disadvantages of TAPP repair are the increased risk of hemodialysis complications and medical expenses; however, we think these are far outweighed by the benefits of TAPP repair. Due to the small number of cases included in this study, the authors plan to increase the sample size and conduct a comparative study to confirm the validity of these conclusions in future work.