
Abstract
Objective:
The purpose of this study was to compare the clinical outcomes of bladder cancer patients treated with extended pelvic lymph node dissection (ePLND) before or after cystectomy under robotic-assisted radical cystectomy (RARC).
Methods:
A retrospective study to identify 348 patients with bladder cancer who underwent RARC was performed. Of the patients, 152 (42.8%) underwent ePLND before radical cystectomy (RC) (group A) and 196 (56.3%) underwent ePLND after RC (group B). The clinical, pathological, and overall survival were compared.
Results:
The total and RC operation time in Group A (total: 130.68 ± 29.25 minutes, RC: 59.45 ± 28.63 minutes) were both shorter than Group B (total: 154.17 ± 38.18 minutes, RC: 94.81 ± 41.21 minutes) (P < .05). However, no significant difference in time of ePLND. The estimate blood loss (EBL) of RC part and total operation (RC+ePLND) in group A was less than group B (both P < .05), while the ePLND part did not show significance. The result of vascular and nerve injury and surgical drain withdrawal time were similar in two groups. The total number of lymph nodes in group A was fewer than group B (16 versus 26; P < .05). Moreover, the number of bilateral internal iliac and presacral lymph nodes of group A was fewer than group B significantly, whereas the number of bilateral external iliac, common iliac, and obturator lymph nodes was similar in two groups. The lymph node density of group A was significantly lower than group B. The median follow-up of all patients was 33.0 months. Importantly, the survival of group B was better than group A (hazard ratio: 1.412; 95% confidence interval: 1.004–1.987; P = .048).
Conclusions:
Performing ePLND before RC reveals better result on operation time and EBL, while, when ePLND after RC, the total number of lymph nodes dissected is more and the survival is better. It recommended ePLND be performed before RC, and it is necessary to recheck the internal iliac and presacral area after cystectomy.
Introduction
Bladder cancer is the most common urinary system malignant tumor in China. 1 According to the 2018 Global Cancer Statistics Report, bladder cancer has already become 8th in the rank of tumors. 2 Approximately, 20%–40% of patients have muscular invasive bladder cancer (MIBC) or high-risk non-MIBC. 1 Radical cystectomy (RC) and extended pelvic lymph node dissection (ePLND) are the golden standard of treatment for those patients. 3 At present, open RC is the most important treatment method for bladder cancer. But because invasive bladder cancer was sensitive with lymph node metastasis, the pelvic lymph node dissection (PLND) reveals very importantly the point on treatment effect. A lot of surgeons believe that the PLND is one of the most important oncologic components of the procedure and the most technical and time-intensive portions of the operation.
Over the past decade, surgical robotic technology has become increasingly accessible, and our overall robotic surgical experience has become more robust with refinements in technique and operative times. The treatment of bladder cancer has been improved a lot with the application of robotic-assisted radical cystectomy (RARC) in urology filed due to its advantages such as less bleeding, earlier bowel motility, and lower postoperative complication rate. 4 RARC and robot-assisted ePLND (RAePLND) have become established as a standardized and reproducible procedure that provides outcomes comparable with open surgery. 4 Nevertheless, the suboptimal reach of the original robotic surgery system impaired cephalad lymphnodal dissection. Improvements in later iterations, as well as adjustments in port placement, have been used to overcome this barrier.
Gradually, the RAePLND is considered to be capable of completing PLND. 5 However, the sequence of ePLND and cystectomy during RARC is still a topic of debate. Moreover, to the best of our knowledge, there were only few evidences on the comparison of the long-term clinical outcomes between patients treated with ePLND before or after cystectomy in RARC series. Therefore, this study aimed to investigate the operative, pathological, and long-term survival outcomes of bladder cancer patients treated with ePLND before and after total cystectomy on the duration of RARC.
Materials and Methods
We retrospectively analyzed patients with bladder cancer who underwent RARC plus ePLND in our hospital from April 2014 to April 2022. This study was approved by the Ethics Committee of Zhejiang Provincial People's Hospital. All patients in this study gave informed consent to participate in this study. All methods in this study were carried out in accordance with relevant guidelines and regulations. The World Health Organization 2004 classification 6 was used for histopathological typing and grading. Pathologic staging was assigned according to the 2016 WHO tumor-node-metastasis classification. 7
Patients' inclusion criteria for the study are the following: (1) clinical stage from T2 to T4 bladder cancer patients or T1 patients who were suspected with high-risk muscular invasive and presented with multiple tumors, and (2) patients younger than 85 years of age. Exclusion criteria for the study are the following: (1) medical history of previous bladder or prostate surgery or radiotherapy; (2) patients with distant metastasis; (4) coagulation dysfunction; (5) important organ dysfunctions; and (6) combined with other systemic malignant tumors. A total of 348 patients were enrolled in our study group. Group A (n = 152) underwent ePLND before RC, and group B (n = 196) underwent ePLND after RC.
Surgical process
All operations were performed by three experienced surgeons in our department. All patients underwent general anesthesia. Both groups underwent RARC and systematic bilateral ePLND, and the urinary diversion (Ileal conduit, orthotopic, ureterostomy) was performed intracorporeally. The operator to choose the PLND before or after total cystectomy usually depends on the habit of operator. No patient was transferred to open surgery during the operation. The ePLND template included the obturator, external iliac, internal iliac, common iliac, and presacral regions bilaterally. For the ePLND margin, the caudal border was the deep circumflex vein and the femoral canal, the cranial border was the ureter crossing over the common iliac artery, the lateral border was the genitofemoral nerve, and the medial border was the vesical fat. Surgical specimens of the bladder and nine distinct pelvic lymph nodes separated by region were submitted for pathological evaluation separately.
Data collection
Demographic information, intraoperative data, and pathological results were recorded for each patient. The two groups were compared for ePLND time, RC time, and total operation (RC+ePLND without urinary diversion) times, estimate blood loss (EBL) in RC, EBL in ePLND, EBL in total operation, vascular injury, obturator nerve injury, time of removing the pelvic drainage, the number of total lymph nodes removed, the number of lymph nodes removed from each region separately (described in surgical process part), and LND (lymph node density, number of positive nodes/total nodes). After statistical analysis, there were no significant differences in demographic, clinical, and pathological characteristics between the two groups (all P values >.05) (Table 1).
Patient's Data Between the Two Groups
Group A: underwent ePLND before RC.
Group B: underwent ePLND after RC.
Bmi, body mass index; ePLND, extended pelvic lymph node dissection; RC, radical cystectomy.
Statistical analysis
SPSS 22.0 software was used. Measurement data were expressed as mean ± standard deviation (x ± s). Categorical variables are described by frequencies and percentages. The number of lymph node was expressed as Median (range). Two independent samples' t-test was used for comparison between groups, count data were expressed as percentage (%), and χ 2 was used for comparison between groups test, P < .05 was considered statistically significant difference. A Kaplan–Meier curve with a two-sided log-rank test and a Cox proportional hazard model with a calculated hazard ratio (HR) and 95% confidence interval (CI) were used to determine survival differences.
Results
The total operation time in the Group A (130.68 ± 29.25 minutes) was shorter than Group B (154.17 ± 38.18 minutes) (P < .05). Moreover, the operation time for RC reveals that Group A (59.45 ± 28.63 minutes) was shorter than Group B (94.81 ± 41.21 minutes) (P < .05). However, there was no significant difference in the time of ePLND between the two groups (P > .05). The EBL of RC part and total operation (RC+ePLND) in group A was less than that in group B, and the difference was statistically significant (both P < .05) while the ePLND part did not show significance in EBL. Likewise, the results of vascular injury, obturator nerve injury, and surgical drain withdrawal time were similar in the two groups (all P > .05) (Table 2).
Surgical and Perioperative Outcomes
Total means RC+PLND.
EBL, estimate blood loss; PLND, pelvic lymph node dissection; RC, radical cystectomy.
The total number of lymph nodes dissected in group A was fewer than that in group B, and the difference was statistically significant (16 [12–27] versus 26 [13–30]; P < .05). Moreover, the number of bilateral internal iliac (right2 [0–6] versus 4 [0–9]; left2 [0–7] versus 4 [0–8]) and presacral (1 [0–5] versus 3 [0–8]) lymph nodes of group A were fewer than group B significantly, while the number of dissected bilateral external iliac, common iliac, and obturator lymph nodes in group A was similar with group B (all P > .05). The LND of group A was significantly lower than group B (Table 3). The median follow-up of all patients was 33.0 months (interquartile range: 6–77 month). Importantly, the survival of group B was better than group A marginal significantly (HR: 1.412; 95% CI: 1.004–1.987; P = .048) (Fig. 1).
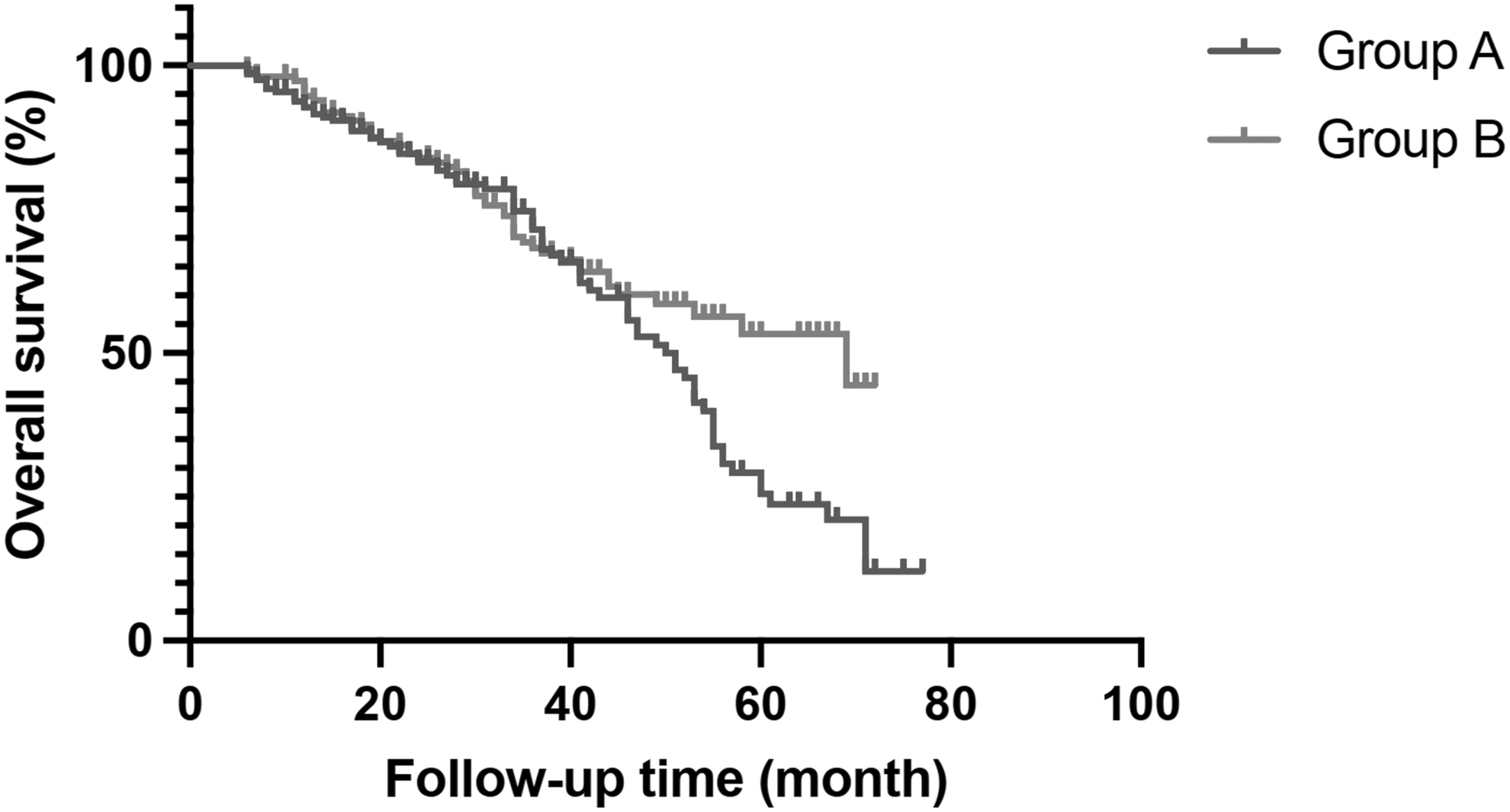
Kaplan–Meier curves of survival comparison in two groups.
Lymph Node Dissection Between Two Groups
LND, lymph node density.
Discussion
RC is the preferred treatment for invasive bladder cancer. In recent years, with the clinical development of robot-assisted minimally invasive techniques, RARC has gradually become as relative “gold standard.” However, since invasive bladder cancer tends to develop lymphatic metastasis, 8 which leads to increased rate of tumor recurrence postoperation, the prevention of lymphatic metastasis is particularly critical for improving patient outcomes. The ePLND has been established as a basic part of RC in open radical cystectomy (ORC) literature that affects oncologic results while acting as a evaluation criteria for the quality of the surgical resection. There was a view that ePLND in RARC cannot be as complete as in ORC due to limitations accessing the proximal nodes.
Nonetheless, contemporary RARC series have revealed lymph node yields comparable with ORC series. 9 But, when to perform the ePLND, that is, before or after the cystectomy, still is a hotly debated topic. Lymphatic dissection before cystectomy can better expose the anatomical level, but the operation space in the pelvis is limited, which is particularly difficult for patients with larger bladder volume; lymphatic dissection postcystectomy produces a larger operating performing space, but the operation time is too long. Our department completed the first case of RARC and ePLND since 2014. Then, we gradually improved the details of the surgical procedure in the following 8 years. Among our three experienced robotic surgeons, some prefer to finish ePLND before RC, while others prefer the opposite process.
According to our result, there are some advantages from our points: (1) The operative time for RC is shorter when it is performed after ePLND. It is because that the blood supply to the bladder was cut off during lymphatic dissection. Also, isolation and control of pedicles during RC is easier and the resection of the bladder is quicker.
Moreover, with the urachus still suspended in its anatomic position, the obliterated umbilical artery provides a useful guide toward the internal iliac regions; (2) The RC performed after ePLND reveals less bleeding than pre-ePLND. The possible explanation might be that ePLND before RC fully exposes the pelvic vascular structures, which minimizes the chance of accidentally injuring the supply vessels of the bladder during cystectomy; (3) the number of left and right internal iliac and presacral lymph node dissection in the group B was more. Similarly, the total number of lymph nodes dissected in group B was more than that in group A. The reason may be that removing the bladder first provides a more capacious surgical field for operator to work in, which makes the node dissection been much easier, especially for the region of presacral and internal iliac.
(4) Group B presented with higher LND due to higher numbers of lymph nodes removed. LND improves upon pathologic nodal staging as it not only accounts for positive LN metastasis but also reflects the quality of the PLND. 10 From the perspective of point 1 and 2, it can be recommended that ePLND be performed before RC for better operative results, whereas from point 3 and 4, the ePLND performed after RC is more beneficial to the pathological results of the patients. Therefore, it is necessary to find a compromise to coordinate the surgical and pathological results. With our suggestion, the patients who had ePLND before RC are advisable to recheck the presacral area and adjacent area of internal iliac for additional lymph nodes after cystectomy.
The past reports revealed that ePLND ends at the level of the common iliac vessels used to take about 60 minutes in open RC.11,12 However, for some patients with more comorbidities, the operation time was associated with postoperative recovery time. Therefore, some operators do not perform ePLND to save operation time. Our results on time of ePLND, which reveals no statistical significance in two groups, showed that the ePLND part occupied 63.67 ± 21.06 minutes in whole surgery. It is similar with other reports. The result indicates that the sequence of ePLND and RARC does not cause any significant differences in the duration of ePLND.
In all operations, no matter which surgeons, it usually needs to be very careful in dealing with the lymph nodes near the blood vessels by robotic arm, so the time spent on the ePLND will not vary greatly. In contrast, the time of RC in group A was significantly reduced. The reason may be that the ePLND part had set up the cystectomy by skeletonizing the pedicles clearly and allowing for smooth resection of the bladder. It also results in decrease of time of the whole RARC part. So, it indicates that the time of surgery was more associated with the time of RC.
The past studies revealed that the number of nodes retrieved in ePLND was directly related to patients' postsurgical survival. 13 Because the dissection of lymph node not only provides valuable prognostic information but has also been shown to confer clinically significant therapeutic benefit for the effect of eradicating micrometastatic disease. One study found significant correlation between the number of nodes retrieved and 5-year recurrence-free survival in pT1–3 patients, as well as those with one to five metastatic lymph nodes. 14 Similarly, another study found improvement in survival in both lymph node pathologically positive and negative patients with increased nodal resected. 15 The Bladder Cancer Collaborative Group proposed using LN yield of 10 to 14 as a metric for quality RC, which was considered as the minimum requirement for the evaluation of lymph node status as well as beneficial for overall survival. 16
In the SWOG 8710 trial, removal of ≥10 nodes was independently associated with better survival. 17 In our study, the total lymph nodes of Group A were less than Group B (16 versus 26; P < .05). Hence, we analyzed the results of the number of lymph nodes, which reveals that the decrease in the number of lymph nodes dissected mainly came from the right internal iliac region, left internal iliac and the presacral region. We believe that the main reason was the interference and view cover from the sigmoid colon, ureter, and bladder during the operation. Moreover, in our study, it is important to note that, the survival time was slightly been influenced by the sequence of ePLND and RARC. The phenomenon might benefit from the higher total LN number in group B than group A.
The average number of lymph nodes dissected in both groups is more than 15 (16 versus 26), which are the values accepted as cutoffs for improving staging, prognosis, and survival. It demonstrated that both groups had completed very meticulous ePLND. This may be the reason why there is only marginal significant difference in the survival curve between the two groups.
It was worth noting that there were many other factors that also could cause changes in perioperative outcomes, although these factors did not show a significant impact in our study. Higher body mass index often means more abdominal fat in Chinese Han population and it brings relative narrow pelvic area. Dissection in this kind of pelvis, especially in large bladder masses, could be considered as a disadvantage of performing PLND and cystectomy. It took more operative time and bleeding. While neoadjuvant platinum-based chemotherapy confers a survival benefit of 5% at 5 years after RC, 18 the majority of suitable patients in clinical practice do not actually receive the treatment. 19 Commonly cited concerns against the utilization of neoadjuvant chemotherapy (NAC) include drug toxicity, a delay to curative surgery, and a potential for increased perioperative outcomes.
However, the IRCC reported that NAC utilization was not associated with a significant increase in perioperative surgical morbidity in those undergoing RARC. 20 In our opinion, the NAC could reduce the volume of tumor and decrease the density of blood vessels around the bladder which supplied tumors. These factors are beneficial to shorten the time of operation and reduce the amount of intraoperative bleeding. The NAC also could reduce the number of positive lymph nodes, which may be beneficial to the patient's survival. 15
There are several limitations to this study. First, it was a single center retrospective study and the number of cases was relatively low, so it cannot be to a high level of evidence. Second, this was not a randomized clinical study, thus it bears all the biases inherent with such a study. The third, there were no metric to evaluate the surgical quality of this complicated surgery. Also, all the operations in our study was performed by three surgeons, the differences yielded in this study might be due to the differences in the experience of the surgeons.
Conclusions
Regardless of when the lymphadenectomy is performed, it is critical to follow all oncologic principles and establish a consistent approach that facilitates a systematic and complete RARC and ePLND. In our study, PLND before total cystectomy reveals better result in RARC on operative time and blood loss, but to achieve better surgical quality, it is necessary to recheck the internal iliac and presacral lymph nodes after cystectomy to avoid omission. Larger series of prospective randomized studies and longer follow-up are warranted to elucidate the effect of timing lymphadenectomy on operative and survival outcomes.
Footnotes
Authors' Contributions
S.W. and Y.B. contributed to writing/editing and data collection or management; D.Z., X.Q., and F.L. contributed to suggestions and data proof reading; L.X. gave approval of the final version of this work. All authors read and approved the final article.
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article available from the corresponding author.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.