
Abstract
Purpose:
The aim of this study was to find out the potential risk factors for the formation of a permanent stoma (PS) for rectal cancer patients with a temporary stoma (TS) after surgery.
Methods:
PubMed, Embase, and the Cochrane Library were searched for eligible studies until November 14, 2022. The patients were divided into the PS group and the TS group. Odds ratio (ORs) and 95% confidence intervals (CIs) were pooled up for describing dichotomous variables. Stata SE 16 was performed for data analysis.
Results:
After pooling up the data, a total of 14 studies involving 14,265 patients were included in this study. The outcomes showed that age (OR = 1.03, 95% CI = 0.96 to 1.10, I2 = 1.42%, P = .00 < .1), surgery type (P = .00 < .1), tumor stage (P = .00 < .1), preoperative chemoradiotherapy (P = .00 < .1), preoperative radiotherapy (P = .01 < .1), neoadjuvant therapy (P = .00 < .1), American Society of Anesthesiologists (ASA) score of ≥3 (P = .00 < .1), anastomotic leakage (P = .01 < .1), local recurrence (P = .00 < .1), and distant recurrence (P = .00 < .1) were associated with the patient with PS. However, sex (P = .15 > .1), previous abdominal surgery (P = .84 > .1), adjuvant chemotherapy (P = .87 > .1), and defunctioning stoma (P = .1) had little association with PS.
Conclusion:
Patients who were elderly, had advanced tumor stages, had a high ASA score, and underwent neoadjuvant therapy should be informed of the high risk of PS before surgery. Meanwhile, those who underwent rectal cancer surgery with a TS should beware of anastomotic leakage, local recurrences, and distant recurrences, which could increase the risk of PS.
Introduction
With the development of surgical methods and instruments, more rectal cancer patients could be treated with surgery.1–7 The current mainstream approach to rectal cancer surgery is anterior resection (AR).8,9 To protect patients from anastomotic leakage, surgery is usually accompanied by a temporary stoma (TS).10,11 However, about a quarter of the patients who underwent AR with a TS developed a permanent stoma (PS).12,13
A TS was usually reversed 3 months after primary surgery to restore bowel continuity.14,15 However, a previous study demonstrated a high incidence of complications after stoma closure, with the highest incidence of surgical site infections, even approaching 40%. 16 There was shown that the most common risk factor for PS is anastomosis-related complications. 17 Some serious complications might even lead to death.18,19 Therefore, PS may then replace TS to avoid the consequences of complications.
Most patients can accept a TS, but have difficulty understanding a PS. The TS could become a PS because of some factors that may be present pre- or postoperatively. Previous studies show a high incidence of PS (14.5%) or even higher (18%) after radical rectal cancer surgery with TS.20,21 There are many studies dedicated to identifying risk factors for PS,20,22–28 but each one is incomplete. Therefore, we conduct this pooling up analysis, and the aim of this study is to identify potential risk factors for PS in patients undergoing rectal cancer surgery with a TS.
Methods
This study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement. 29
Search strategy
A total of 296 studies were searched from three databases (109 in PubMed, 172 in Embase, and 15 in the Cochrane Library) until November 14, 2022. The core terms were AR, PS, and rectal cancer. Then, these words were connected with “AND.” The search was limited to titles and abstracts. The only language available was English.
Inclusion and exclusion criteria
To filter out suitable articles, the inclusion criteria were as follows: (1) patients diagnosed with rectal cancer and underwent rectal cancer surgery with a stoma; and (2) data for both the PS and TS groups were available in the article. As for exclusion criteria: (1) case reports, case series, comments, letters to the editor, and conference abstracts; and (2) duplicate data.
Study selection
According to the inclusion and exclusion criteria, independent screening was conducted by 2 researchers. The screening steps were as follows: first, we excluded duplicate studies; then, we scanned the titles and abstracts; after that, the full text was read carefully to find eligible studies. All disagreements were well resolved through teamwork.
Data collection
The information contained baseline characteristics of included studies and information of included patients. The studies' characteristics included author, published year, country, study date, study type, the total number of patients, number of patients in the PS group and the TS group, respectively, and Risk Of Bias In Non-randomised Studies-of Interventions (ROBINS-I) grade. As for patients' information, age, sex, tumor stage, surgery type, American Society of Anesthesiologists (ASA), previous abdominal surgery, preoperative chemoradiotherapy, adjuvant chemotherapy, anastomotic leakage, defunctioning stoma, distant recurrence, local recurrence, preoperative radiotherapy, and neoadjuvant therapy were collected.
Quality assessment
The ROBINS-I grade was used to evaluate the quality of the included studies. 30 The ROBINS-I scale contained 7 domains (bias due to confounding, bias in selection of participants into the study, bias in classification of interventions, bias due to deviations from intended interventions, bias due to missing data, bias in measurement of outcomes, and bias in selection of the reported result). The levels of risk bias included low risk, moderate risk, serious risk, and critical risk.
Statistical analysis
Dichotomous variables were described by odds ratios (ORs) and 95% confidence intervals (CIs). To evaluate the statistical heterogeneity, the I2 value and the chi-squared test were used.31,32 We used the random effects model, and P < .1 was considered statistically significant. Stata SE 16 was used for data analysis.
Results
Study selection
After searching PubMed, Embase, and the Cochrane Library, a total of 296 studies were found (109 in PubMed, 172 in Embase, and 15 in the Cochrane Library). Then, 81 duplicate records were removed. The 215 left articles were browsed for titles and abstracts after excluding unqualified study types. After that, 25 articles were left and full texts were accessed for eligibility. Finally, 14 eligible studies were included in this analysis17,20–28,33–36 (Fig. 1).
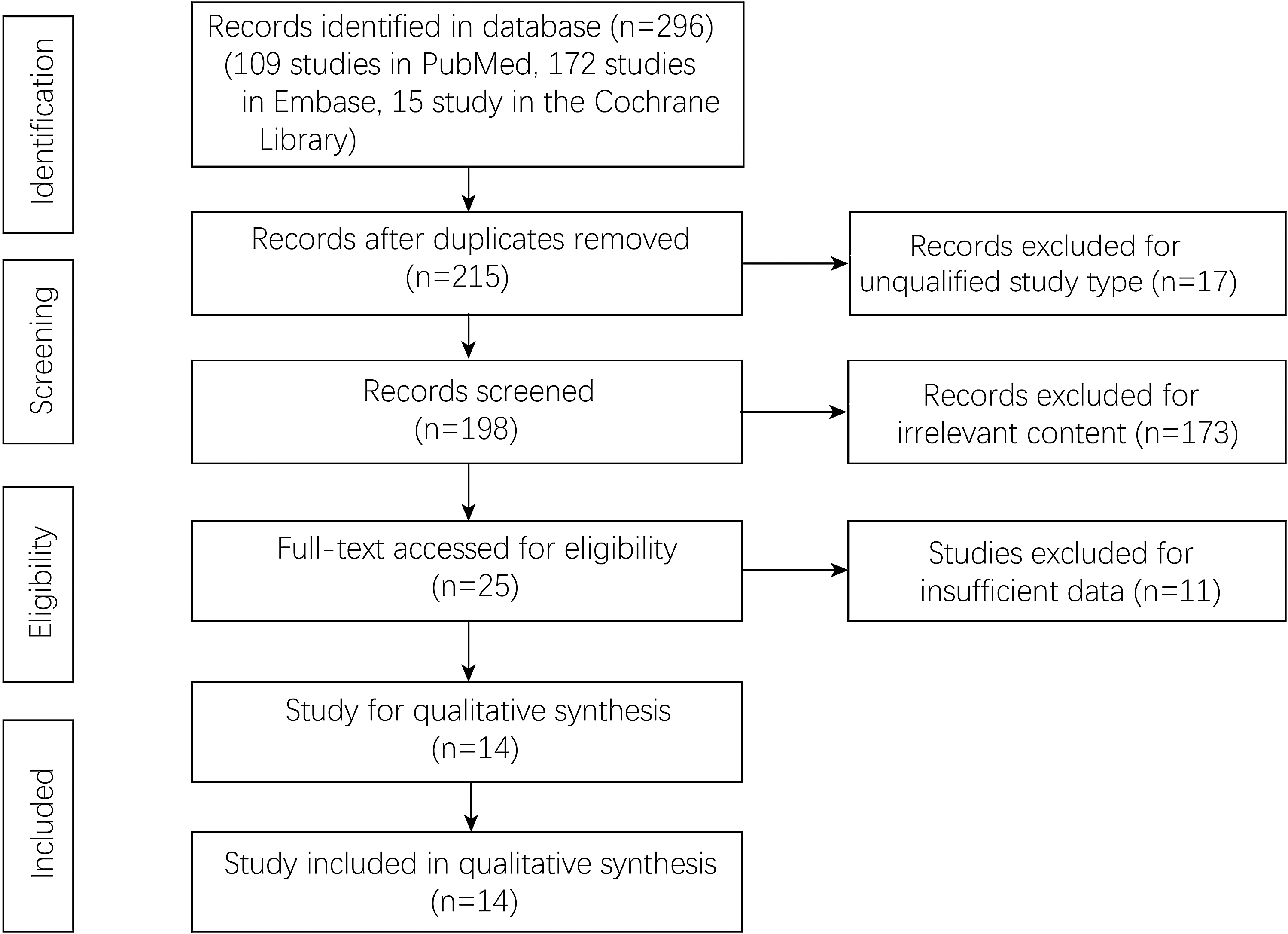
Flowchart of study selection.
Baseline characteristics of included studies
The included articles contained 14,265 patients. The published year was from 2010 to 2021, and they were published in Sweden, Canada, Austria, Germany, Korea, Poland, and China. The study scope was from 1985 to 2018. Some other characteristics, including study type, the number of patients in the PS group and the TS group, and the ROBINS-I grade of studies, are shown in Table 1.
Baseline Characteristics of Included Studies
PS, permanent stoma; ROBINS-I, Risk Of Bias In Non-randomised Studies-of Interventions; TS, temporary stoma.
Preoperative/postoperative risk factors of PS
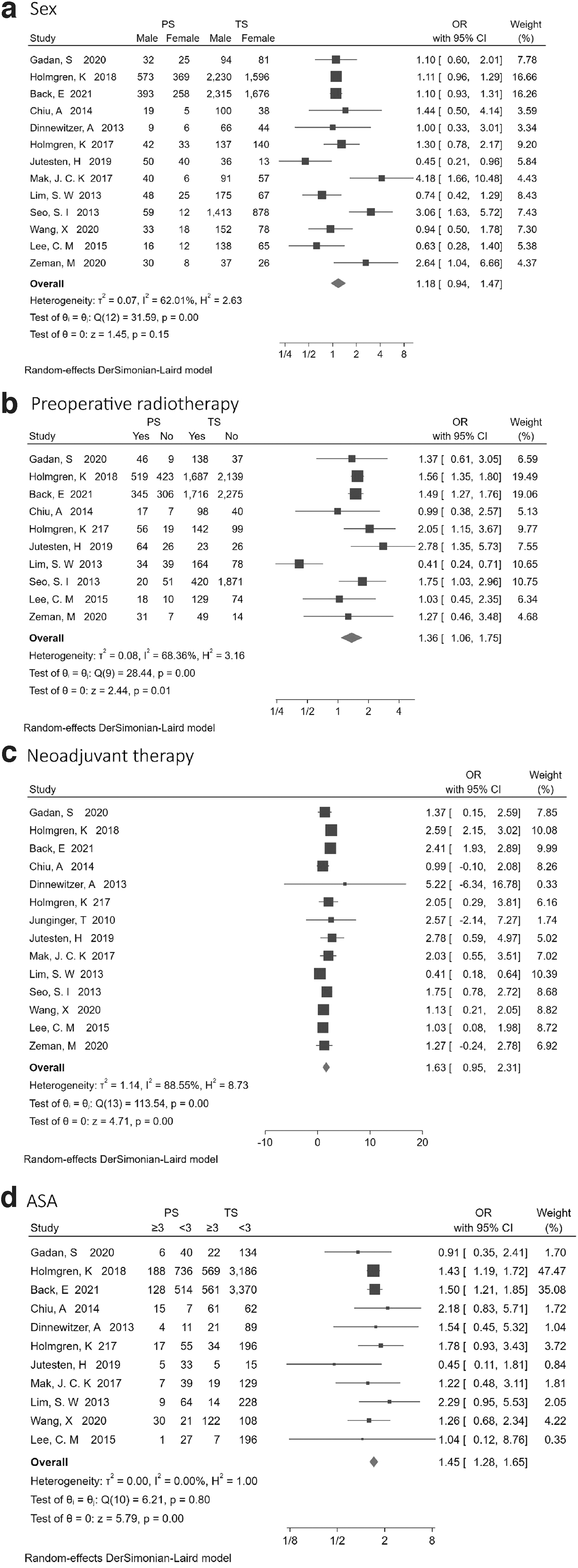
According to analysis, as Figure 2 shows, the PS group had more patients who received preoperative radiotherapy (OR = 1.36, 95% CI = 1.06 to 1.75, I2 = 68.36%, P = .01 < .1) (Fig. 2b) or neoadjuvant therapy (OR = 1.63, 95% CI = 0.95 to 2.31, I2 = 88.55%, P = .00 < .1) (Fig. 2c). Meanwhile, the PS group had a higher proportion of an ASA score of ≥3 (OR = 1.45, 95% CI = 1.28 to 1.65, I2 = 0.00%, P = .00 < .1) (Fig. 2d). Sex had no influence on the incidence of PS (OR = 1.18, 95% CI = 0.94 to 1.47, I2 = 62.01%, P = .15 > .1) (Fig. 2a).
Furthermore, the outcomes showed that age (OR = 1.03, 95% CI = 0.96 to 1.10, I2 = 1.42%, P = .00 < .1), surgery type (OR = 1.75, 95% CI = 1.74 to 2.08, I2 = 0.00%, P = .00 < .1), tumor stage (OR = 2.56, 95% CI = 1.93 to 3.99, I2 = 11.00%, P = .00 < .1), preoperative chemoradiotherapy (OR = 1.75, 95% CI = 1.53 to 1.97, I2 = 0.00%, P = .00 < .1), anastomotic leakage (OR = 3.85, 95% CI = 1.48 to 10.04, I2 = 93.58%, P = .01 < .1), local recurrence (OR = 6.77, 95% CI = 3.00 to 10.53, I2 = 52.62%, P = .00 < .1), and distant recurrence (OR = 2.20, 95% CI = 1.37 to 3.51, I2 = 66.28%, P = .00 < .1) were the risk factors of PS. However, previous abdominal surgery (OR = 0.96, 95% CI = 0.66 to 1.40, I2 = 0.00%, P = .84 > .1), adjuvant chemotherapy (OR = 1.01, 95% CI = 0.91 to 1.12, I2 = 0.00%, P = .87 > .1), and defunctioning stoma (OR = 2.00, 95% CI = 0.88 to 4.55, I2 = 93.96%, P = .1) had little association with PS (Table 2).
Risk Factors for Permanent Stoma
P < .1.
CI, confidence interval; IV, tumor stage IV; NA, not applicable; OR, odds ratio; PS, permanent stoma; TS, temporary stoma.
Sensitivity analysis
Each study was excluded at a time for sensitivity analysis, and there was no significant difference between every outcome.
Discussion
A total of 14 studies involving 14,265 patients were enrolled in this pooling up analysis.17,20–28,33–36 After data analysis, the outcomes revealed that pre- or postoperative factors could lead to PS. More open surgery rate, later tumor stage, a higher proportion of preoperative chemoradiotherapy, more anastomotic leakage rate, more local recurrence rate, and a higher proportion of distant recurrence were revealed in the PS group. Moreover, age, preoperative radiotherapy, neoadjuvant therapy, and an ASA score of ≥3 were the risk factors of PS as well. However, sex, previous abdominal surgery, adjuvant chemotherapy and defunctioning stoma had little association with PS.
Previous studies reported a variety of risk factors of PS. The most frequently reported risk factor for PS was anastomosis-related complications.17,20–22,24–26,35,36 One of the most significant complications was anastomotic leakage. This was well in line with the findings of us. Anastomotic leakage was a major contributor to PS formation,21,35 and failure of the stoma might reduce the risk of PS formation due to anastomotic leakage. 17 Similarly, in our study, we found that defunctioning stoma had little association with PS. Some patients could not accept a PS that reduced the patient's quality of life. 37 Therefore, this current analysis was to find out what were the potential risk factors for the formation of a PS after surgery for rectal cancer with a TS. So that the operator could give the patient a preoperative explanation of the possibility of PS.
The effect of preoperative radiotherapy on PS remained controversial. We demonstrated that neoadjuvant therapy might increase the risk of PS. Hassan demonstrated that preoperative radiotherapy increased the risk of PS as well. 38 However, some authors demonstrated that long-term neoadjuvant radiotherapy was effective in diverting patients from planned abdominoperineal resection to a sphincter-preserving procedure to avoid a PS.3,39 This may be a late tumor stage in patients on neoadjuvant therapy. Holmgren et al., 35 Mak et al., 24 and Lim et al. 25 revealed that stage IV tumor could lead to PS. However, in this study, we were unable to distinguish between which was the main factor contributing to PS, tumor stage and neoadjuvant treatment were both independent risk factors.
Ostomy was a common procedure used to protect against complications associated with anastomotic leakage after colorectal cancer surgery or to resolve bowel obstruction.40–42 To prevent anastomotic leakage, experts proposed prophylactic stomas.43–45 These stomas were usually considered temporary. There were reports that both early (<30 days) and late (>6 months) stoma closure might be associated with an increased rate of postoperative complications.46,47 Therefore, the best time to close the stoma is 4–5.6 months after the stoma.13,21,25 Because of some factors, a TS could not be returned, resulting in a PS. Local recurrence was also strongly associated with PS.21,24–26,34,36 Some studies showed that the nonreversal rate for ileostomy was 13.8%–24.9%.10,13,21,48,49
In our pooled analysis, we found age, surgery type, tumor stage, ASA ≥3, neoadjuvant therapy, and preoperative chemoradiotherapy were the risk factors of PS. The reason might be patients, who were older, with later tumor stage, with poorer physical condition and with ASA ≥3, had poor recovery after surgical trauma. It was reported that high incidence of postoperative anastomotic leakage in older people.23,24 Anastomosis-related complications were a major cause of PS.21,25,36,50 Therefore, the operator should be more careful when performing the procedure. More effort was put into postoperative management.
To our knowledge, this pooled analysis was the first to report the pre- and postoperative risk factors comprehensively. However, there were some limitations as well. First, almost all of the included studies were retrospective studies, which might lead to a reporting bias. Second, some of the indicators included in the article used different classification criteria. More relevant research was needed in the future.
In conclusion, patients who were elderly, had a high ASA score, had advanced tumor stages, or underwent neoadjuvant therapy should be informed of the high risk of PS before surgery. Meanwhile, those who underwent rectal cancer surgery with a TS should beware of anastomotic fistulas, local recurrences, or distant recurrences, which can increase the risk of PS.
Footnotes
Acknowledgments
We thanked all the authors in this article.
Authors' Contributions
All authors contributed to data collection and analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the study.
Data Availability Statement
The data were accessed in the database.
Disclosure Statement
The authors declare that there are no conflicts of interest.
Funding Information
Not apply.