
Abstract
Background:
Gastric cancer has the third highest cancer-related mortality worldwide. There is no consensus regarding the optimal surgical technique to perform curative resection surgery.
Objective:
Compare laparoscopic gastrectomy (LG) and robotic gastrectomy (RG) regarding short-term outcomes in patients with gastric cancer.
Materials and Methods:
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. We searched the following topics: “Gastrectomy,” “Laparoscopic,” and “Robotic Surgical Procedures.” The included studies compared short-term outcomes between LG and RG. Individual risk of bias was assessed with the Methodological Index for Non-Randomized Studies (MINORS) scale.
Results:
There was no significant difference between RG and LG regarding conversion rate, reoperation rate, mortality, overall complications, anastomotic leakage, distal and proximal resection margin distances, and recurrence rate. However, mean blood loss (mean difference [MD] −19.43 mL, P < .00001), length of hospital stay (MD −0.50 days, P = .0007), time to first flatus (MD −0.52 days, P < .00001), time to oral intake (MD −0.17 days, P = .0001), surgical complications with a Clavien-Dindo grade ≥III (risk ratio [RR] 0.68, P < .0001), and pancreatic complications (RR 0.51, P = .007) were significantly lower in the RG group. Furthermore, the number of retrieved lymph nodes was significantly higher in the RG group. Nevertheless, the RG group showed a significantly higher operation time (MD 41.19 minutes, P < .00001) and cost (MD 3684.27 U.S. Dollars, P < .00001).
Conclusion:
This meta-analysis supports the choice of robotic surgery over laparoscopy concerning relevant surgical complications. However, longer operation time and higher cost remain crucial limitations. Randomized clinical trials are required to clarify the advantages and disadvantages of RG.
Introduction
Nowadays, gastric cancer is the fifth most common cancer worldwide, with its highest prevalence being in Mongolia, Japan, and South Korea. Moreover, WCRF International, in 2020, demonstrated that gastric cancer has the third highest cancer-related mortality rate (7.7/100,000) and it is the fifth most incident tumor in the entire world (11.1/100,000).1,2
Despite the development of new surgical techniques and medical devices, prognosis remains poor. 3 Therefore, it is necessary to improve screening methods to achieve earlier diagnosis and improve the odds of finding a resectable tumor, so as to reduce its burden.4,5
There are two approaches to treat localized gastric cancer: endoscopic resection or radical gastrectomy. The first one is used for gastric cancer classified as stage IA (T1 N0 M0), according to the TNM classification. On the other hand, radical gastrectomy is used for stage IB-III gastric cancers (>T1 and/or ≥N0 M0), and is associated with a simultaneous D2 lymphadenectomy. To increase the probability of a curative resection, this treatment requires neoadjuvant and adjuvant chemotherapy, to reduce preoperative tumor size and probability of recurrence, respectively. 6
Currently, the main surgical approaches are minimally invasive, including laparoscopic surgery and robotic surgery. 5
The largely used conventional laparoscopic gastrectomy (LG) has shown several advantages, when compared with open gastrectomy, such as better surgical safety, less trauma, lower operative morbidity, and faster recovery, with similar overall survival, oncologic outcomes, and relapse-free survival.6,7
On the other hand, robotic gastrectomy (RG) yields high-resolution three-dimensional (3D) images, wrist instruments that offer freedom, tremor filtering technology, and less fatigue. These features are expected to overcome some drawbacks of laparoscopic surgery. 5
There are several studies that reported the advantages of RG, when compared with LG, on the following short-term outcomes in patients with gastric cancer: less blood loss, higher number of harvested lymph nodes, less time to first flatus, shorter length of hospital stay, and less postoperative complications. 8 However, the cost and the operative time related to the expensive instruments and the low experience in performing robotic surgery are still relevant limitations to its current utilization.5,9
Therefore, our systematic review includes the most recent observational studies and the current literature about the comparison of the short-term outcomes between LG and RG for gastric cancer patients to clarify the feasibility and efficiency of robotic surgery, as it is predicted to be more prevalent in the coming years. 10
Materials and Methods
Search strategy/information sources
We conducted our meta-analysis according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Literature search was performed independently by 2 reviewers, on the following databases: PubMed, Web of Science, and Cochrane Library. The query used in PubMed was as follows: “Search (((laparoscopic gastrectomy) OR ((“” Gastrectomy”” [Majr:NoExp]) AND “” Laparoscopy “”[Mesh]))) OR ((((“” Gastrectomy “” [Majr:NoExp]) AND “” Robotic Surgical Procedures “” [Mesh])) OR robotic gastrectomy).” In the Web of Science and Cochrane Library, we used the following query: “((“Gastrectomy” AND “Laparoscopy”) OR (“Laparoscopic Gastrectomy”)) AND (“Robotic Surgery” OR “Robotic Surgical Procedures” OR “Robotic Gastrectomy”).” Existing systematic reviews were also consulted for additional articles.
Study selection and eligibility criteria
The researchers screened the literature and selected articles based on their titles and abstracts. In accordance with previous reviews, we included observational clinical studies that compared short-term outcomes between the two surgical approaches (RG and LG), in patients with gastric cancer, who underwent curative-intent surgery.8,11,12
Then, the authors reviewed the full texts and excluded articles that met the following exclusion criteria: (1) articles that also reported comparison of two robotic systems, (2) proximal gastrectomy comparison only, and (3) D1 lymphadenectomy only. One article was excluded due to the impossibility of obtaining an English version.
Data extraction
Two reviewers independently read and interpreted every original study. Data extraction comprised study information (author, region, published year, study period, study design, sample size, surgical extension, level of lymphadenectomy, and reconstruction options), patients' characteristics (age and gender), and short-term outcomes, which included 3 groups: surgical outcomes (operating time, blood loss, conversion rate, reoperation rate, and mortality rate), postoperative outcomes (length of hospital stay, time to first flatus, time to oral intake, overall complications, surgical complications according to Clavien-Dindo [CD] Grade, anastomotic leakage, pancreatic complication, and cost of operation), and oncological outcomes (distal resection margin distance, proximal resection margin distance, recurrence rate, and number of retrieved lymph nodes). These variables were chosen in accordance with previous systematic reviews8,9,11,12 (Tables 1 and 2).
Summary of Studies Included in the Meta-Analysis
BI, Billroth I; BII, Billroth II; D, distal; EGJ, esophagogastric junction; EJJ, esophagojejunostomy; GG, gastro-gastro anastomosis; LG, laparoscopic gastrectomy; LND, lymphadenectomy; MINORS, Methodological Index for Non-Randomized Studies; NA, not available; OCS, observational clinical study; P, prospectively collected data; P, proximal; PCD, prospectively collected data; PPG, pylorus-preserving gastrectomy; R, retrospectively collected data; RG, robotic gastrectomy; RY, Roux-en-Y; ST, subtotal; T, total.
Patients' Characteristics
F, female; LG, laparoscopic gastrectomy; M, male; NA, not available; Pt, patients; RG, robotic gastrectomy; SD, standard deviation.
Quality assessment
In our meta-analysis, we used the MINORS (Methodological Index for Non-Randomized Studies) scale to assess the quality and individual risk of bias of our nonrandomized studies. The final version of the MINORS scale comprises 12 items, which identify whether the included studies contained a clearly stated aim, included all potentially fit patients, involved prospective collection data, had appropriate endpoints according to the aim of the study, had blind evaluation of objectives and subjective endpoints, had an appropriate follow-up period, loss of follow-up under 5%, and prospective calculation of the study size. Furthermore, the MINORS scale also evaluates additional criteria for comparative studies such as the control group, the time period of both groups, their baseline equivalence, and an adequate statistical analysis. Each item is scored as 0 (not reported), 1 (reported, but inadequate), or 2 (report and adequate). The total score, in comparative studies, is 24 points. 13
Statistical analysis
We performed our meta-analysis using Review Manager (Version 5.4.1).
For dichotomous outcomes, we presented the results as risk ratio (RR) with 95% confidence intervals (CIs), by using the Mantel-Haenszel method. For continuous outcomes, we presented the results as mean differences (MD) with 95% CI, by using the generic inverse variance method. Some studies presented their outcomes as median and range. Therefore, we applied a method described by Hozo et al. 14 to estimate the mean and standard deviation. We used an alpha (α) level of 0.05 for statistical significance. The Chi-squared (χ 2 ) test and the I-squared (I 2 ) measure were used to assess heterogeneity. We applied a random effects model because of the clinical heterogeneity of included studies. We assessed the existence of publication bias among included studies using funnel plots, provided as Supplementary File S1.
Subgroup analysis
In our systematic review, 22 studies used propensity score matching (PSM) to minimize baseline differences that usually contribute to bias in the interpretation of results. The remaining 31 studies did not perform PSM. Hence, we conducted a subgroup analysis to understand whether PSM had any effect in the association between the surgical approach and the studied outcomes.
Results
Studies selected and characteristics
We selected 2848 articles from our research on PubMed, Web of Science and Cochrane Library. After reading their titles and abstracts, we selected 82 full-text articles to assess for eligibility. No additional study from other sources was deemed relevant. From these articles, we excluded 29 because they did not fulfill the inclusion criteria. Then, for our systematic review, we included 53 studies in the quality assessment and quantitative analysis (Fig. 1). These studies include a total of 25,521 participants, of which 8154 underwent RG and 17,367 underwent LG. All studies were retrospective observational studies.15–67
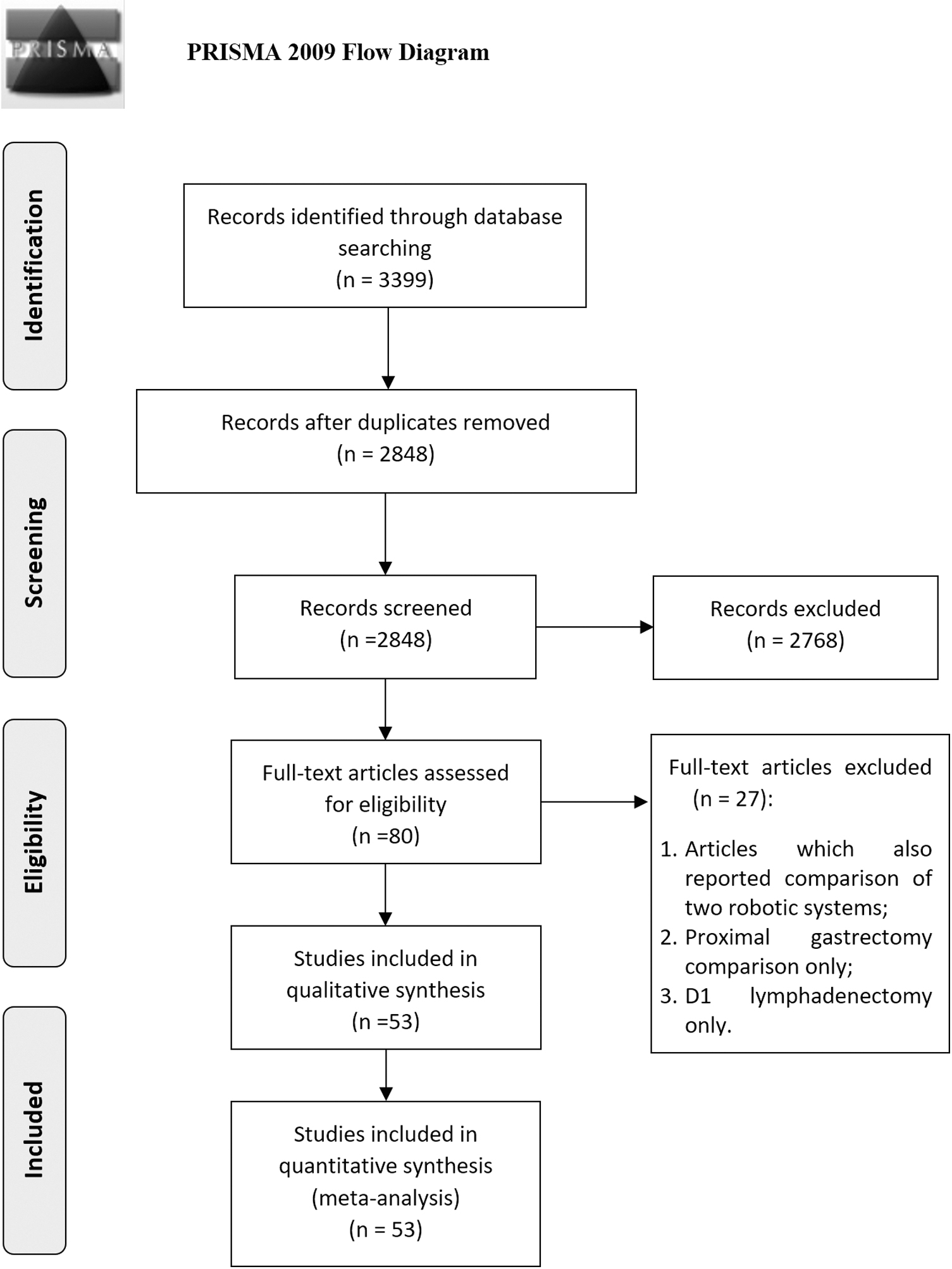
Flow diagram according to the PRISMA guidelines. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Quality assessment
The median score in the MINORS scale was 22, with a range of 19–23. Therefore, all included studies were considered adequate to be included in the quantitative analysis.
Meta-analysis
A synthesis of every meta-analytical measure is presented in Table 3. We provide the results of each individual meta-analysis as forest plots in Supplementary File S2.
Results of the Meta-Analysis
CI, confidence interval; LG, laparoscopic gastrectomy; MD1, mean difference; MD2, margin distance; RG, robotic gastrectomy; RR, risk ratio.
Surgical outcomes
Operative time
Our meta-analysis included 50 studies, which reported the operation time. It was significantly shorter in the LG group, when compared with the robotic surgery group (MD 41.19, P < .00001 [95% CI: 33.47 to 48.92], I2 = 98%, P < .00001). Mean operation time was 269.22 minutes in the robotic surgery group and 225.65 in the laparoscopic surgery group (Fig. 2).

Operative time.
Blood loss
Blood loss was reported in 46 studies. The mean blood loss was 90.72 mL in the RG group and 108.2 mL in the LG group. This difference was statistically significant (MD −19.43, P < .00001 [95% CI: −25.23 to −13.62], I2 = 92% P < .00001).
Conversion
This outcome was included in 33 studies and demonstrated no statistically significant difference between the 2 groups (RR 0.68, P = .09 [95% CI: 0.43 to 1.07], I2 = 0%, P = .50). Conversion rate to open surgery was 0.59% (26/4390) in the RG group and 0.89% (69/7730) in the LG group.
Reoperation
Eighteen studies reported reoperation rate. There was no statistically significant difference between both surgical approaches, regarding reoperation (RR 0.89, P = .57 [95% CI: 0.59 to 1.34], I2 = 0%, P = .72). Reoperation rate was 1.38% (37/2677) in the RG group and 1.56% (68/4366) in the LG group.
Mortality
Thirty-nine studies were included, and mortality was comparable between both groups (RR 1.20, P = .37 [95% CI: 0.81 to 1.77], I2 = 0%, P = .98). Mortality rate was 0.6% (40/6708) in the RG group and 0.59% (64/10,776) in the LG group (Fig. 3).

Mortality.
Postoperative outcomes
Length of hospital stay
This outcome was reported in 52 studies. The mean length of hospital stay was 8.74 days in the robotic surgery group and 9.38 days in the laparoscopic surgery group. The robotic surgery group displayed a significantly shorter hospital stay (MD −0.50, P = .0007 [95% CI −0.79 to −0.21], I2 = 85% P < .00001).
Time to first flatus
There were 25 studies that reported time to first flatus. The robotic surgery group showed a significantly shorter time to first flatus (MD −0.52, P < .00001 [95% CI −0.55 to −0.50], I2 = 98% P < .00001).
Time to oral intake
Twenty-seven studies included this outcome. Time to oral intake was significantly shorter in the robotic surgery group (MD −0.17, P = .0001 [95% CI −0.25 to −0.08], I2 = 53% P = .0008).
Overall complications
The overall complication rate was 12.97% (873/6732) in the RG group and 13.11% (1504/11,469) in the LG group. There were 51 studies reporting this outcome, and the meta-analysis did not demonstrate a statistically significant difference (RR 0.93, P = .15 [95% CI 0.85 to 1.03], I2 = 18%, P = .14).
Surgical complications (grade ≥III in the CD classification)
Thirty-one studies reported this outcome. Our study showed that the robotic surgery group had a significantly lower number of surgical complications (RR 0.68, P < .0001 [95% CI 0.57 to 0.82], I2 = 7%, P = .35), with a rate of 3.88% (212/5464) in the RG group and 6.4% (467/7303) in the LG group (Fig. 4).

Surgical complications (Grade ≥III in the Clavien-Dindo classification).
Anastomotic leakage
Thirty-three studies included this outcome. The rate of anastomotic leakage was 1.72% (91/5289) in the RG group and 1.93% (168/8721) in the LG group. This difference was not significant (RR 1.06, P = .71 [95% CI 0.78 to 1.45], I2 = 16%, P = .21).
Pancreatic complications
This outcome was included in 21 studies. The rate of pancreatic complications was 0.64% (22/3445) in the RG group and 1.42% (78/5497) in the LG group. This difference was statistically significant (RR 0.51, P = .007 [95% CI 0.31 to 0.83], I2 = 0%, P = .60) (Fig. 5).
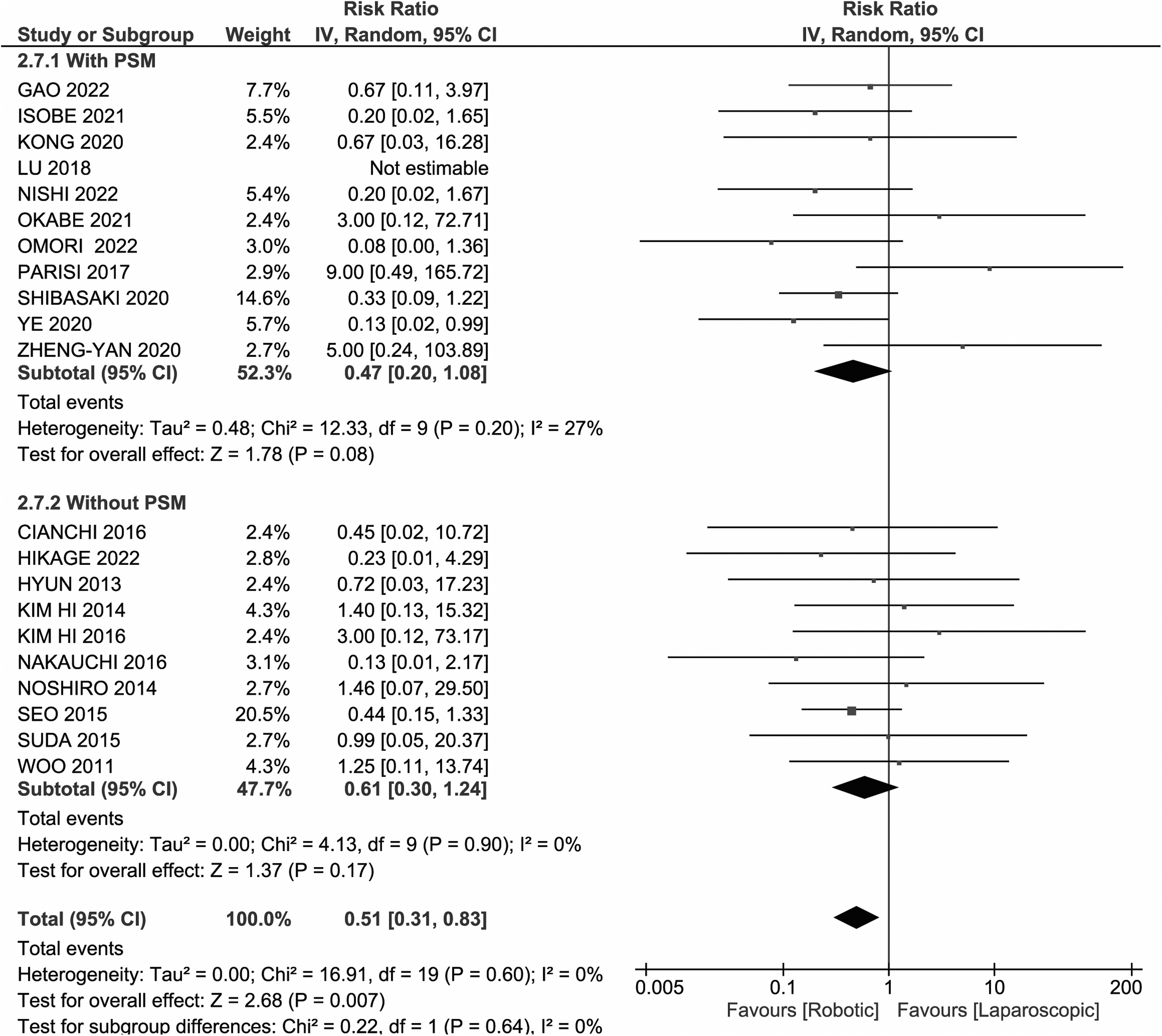
Pancreatic complications.
Cost
Cost was reported in eight studies. On average, the total cost of robotic surgery was 3684.27 U.S. dollars (3442.99 Euros), significantly higher compared with laparoscopic surgery (MD 3684.27, P < .00001 [95% CI 2986.11 to 4382.44], I2 = 90% P < .00001) (Fig. 6).
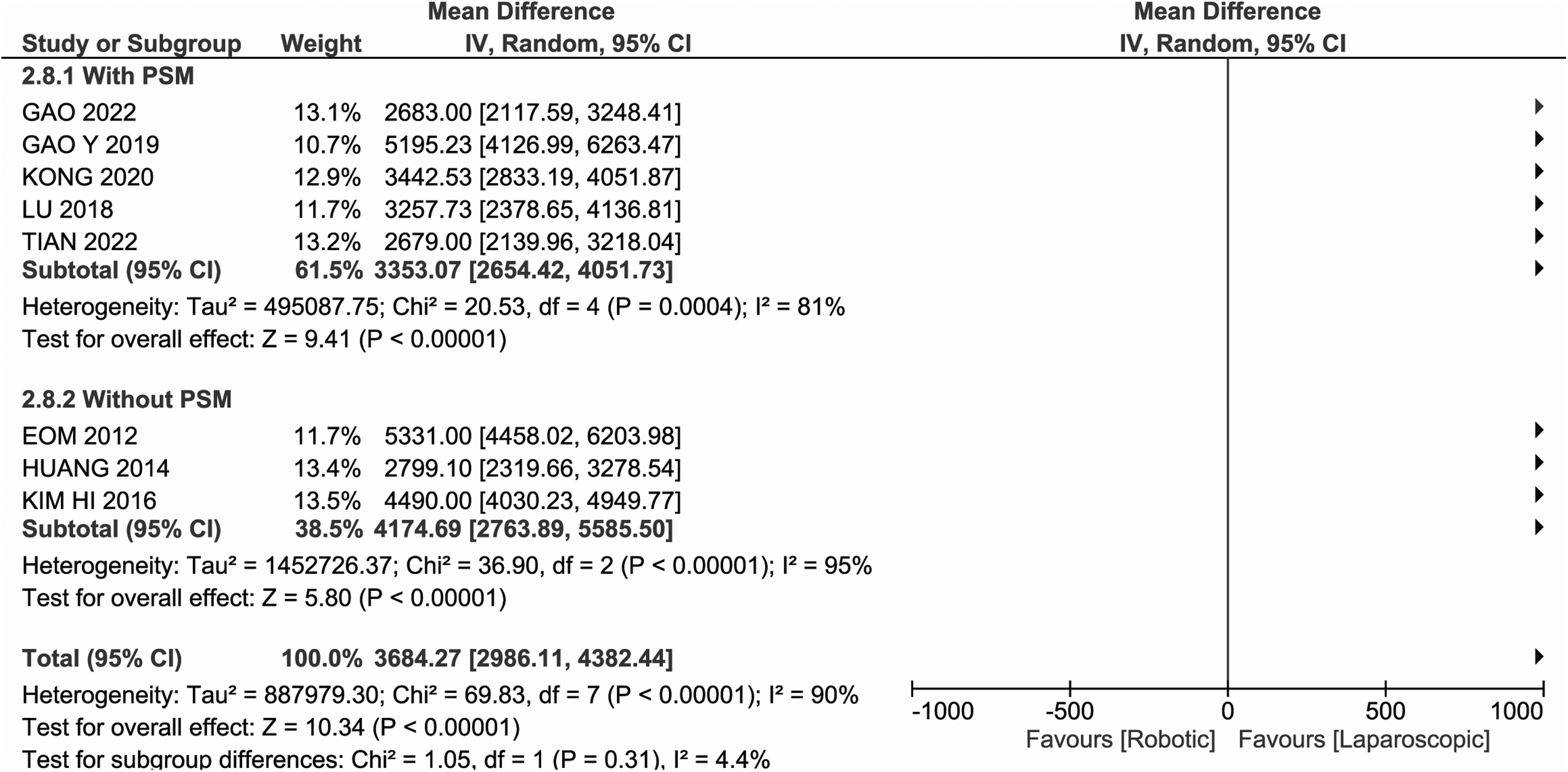
Cost.
Oncological outcomes
Distal resection margin distance
Fourteen studies reported this outcome. The mean distal resection margin distance was 6.9 cm in the robotic surgery group and 6.82 cm in the laparoscopic surgery group. The difference was not statistically significant (MD 0.16, P = .37 [95% CI −0.19 to 0.51], I2 = 76% P < .00001).
Proximal resection margin distance
Fifteen studies reported this outcome. The mean proximal resection margin distance was 4.35 cm in RG and 4.24 cm in LG. The difference was not statistically significant (MD 0.06, P = .29 [95% CI −0.05 to 0.18], I2 = 0% P = .52).
Recurrence
Eleven studies reported this outcome. The recurrence rate was 9.9% (134/1358) in the RG group and 10.6% (215/2024) in the LG group. There was no statistically significant difference (RR 0.95, P = .61 [95% CI 0.77 to 1.17], I2 = 0%, P = .91).
Number of retrieved lymph nodes
The number of retrieved lymph nodes was reported in 49 studies. The mean number of retrieved lymph nodes was 36.7 in the RG group and 35.61 in the LG group. The robotic surgery group had a significantly higher number of retrieved lymph nodes (MD 1.69, P = .001 [95% CI 0.68 to 2.70], I2 = 93% P < .00001) (Fig. 7).

Number of retrieved lymph nodes.
Subgroup analysis
Surgical outcomes
Operative time
Both subgroups demonstrated a significantly longer operative time in the robotic surgery group. Heterogeneity was high and statistically significant. In addition, regarding subgroup differences, I2 = 73.5% and P = .05 (Fig. 2).
Blood loss
There was significantly lower blood loss in the robotic surgery group in studies with and without PSM. This difference was more evident in the PSM subgroup. There was no significant difference between groups (I 2 = 0%, P = .76) and heterogeneity was similar.
Conversion
The PSM subgroup presented a stronger association between surgical approach and conversion rate, with the robotic surgery group being lower in both subgroups. However, neither subgroup had a statistically significant result (P = .06 for studies with PSM and P = .61 for studies without PSM). There was no significant difference between subgroups (I 2 = 0%, P = .63) and no significant heterogeneity in either.
Reoperation
The subgroups showed opposite results, both without statistical significance. Inside each subgroup, heterogeneity was not significant. There was no significant difference between subgroups either (I 2 = 68.4%, P = .08).
Mortality
There was no significant difference between subgroups (I 2 = 0%, P = .98) and neither displayed significant heterogeneity. Both favor the laparoscopic surgery group, although these results are not statistically significant (Fig. 3).
Postoperative complications
Length of hospital stay
The PSM subgroup displayed significantly lower length of hospital stay in the robotic surgery group, whereas there was no significant difference in studies without PSM, despite both favoring the robotic surgery group. Heterogeneity in both subgroups was significantly high. Between subgroups, there was no significant difference, with I2 = 0%, P = .84.
Time to first flatus
Both subgroups showed a significantly shorter time to first flatus in the robotic surgery group, although there was significant heterogeneity. There was a significant difference between subgroups (I 2 = 99.8%, P < .00001). The PSM subgroup displayed lower heterogeneity.
Time to oral intake
The robotic surgery group had significantly lower time to oral intake in both subgroups. Heterogeneity was significant in the non-PSM subgroup (I 2 = 71%, P = .0008) There was no significant difference between subgroups (I 2 = 0%, P = .32).
Overall complications
There was no significant difference in either subgroup. The PSM subgroup favored the robotic surgery group, but P = .06. Differences between subgroups were not statistically significant (I 2 = 56%, P = .13).
Surgical complications (grade ≥III in the CD classification)
The PSM subgroup demonstrated a significantly lower rate of surgical complications in the robotic surgery group when compared to the laparoscopic surgery group (3.9% and 5.76%, respectively; RR = 0.66, P < .0001). In addition, both subgroups revealed low heterogeneity and there was no significant difference between them (I 2 = 0%, P = .97) (Fig. 4).
Anastomotic leakage
In the PSM subgroup, anastomotic leakage was lower in the robotic surgery group. However, the results were not statistically significant (RR = 0.73; P = .11). In both subgroups, heterogeneity was not significant. The differences between them were statistically significant (I 2 = 80.8%, P = .02), as they showed opposite results.
Pancreatic complications
Both subgroups favored the robotic surgery group, but the results were not statistically significant. There was no significant heterogeneity. Moreover, the 2 subgroups were similar (I 2 = 0%, P = .64) (Fig. 5).
Cost
Both subgroups significantly favored laparoscopic surgery. Heterogeneity was high and significant in both subgroups. There was no significant difference between subgroups (I 2 = 4.4%, P = .31) (Fig. 6).
Oncological outcomes
Distal and proximal resection margin distances
Regarding distal resection margin, both subgroups were similar (I 2 = 0%, P = .73). In studies without PSM, there was significant heterogeneity (I 2 = 85%, P < .00001). For the proximal resection margin, there was no significant difference between subgroups (I 2 = 23.6%, P = .25) and neither subgroup displayed significant heterogeneity.
Recurrence
None of the subgroups showed a significant difference in recurrence rate between the two approaches, and heterogeneity was not significant. There was no significant difference between subgroups (I 2 = 0%, P = .36).
Number of harvested lymph nodes
The 2 subgroups showed a significantly higher number of retrieved lymph nodes in the robotic surgery group. They appeared to be similar concerning subgroup differences (I 2 = 0%, P = 1.00), and they both showed high values of heterogeneity, individually (Fig. 7).
Discussion
This meta-analysis, which, as far as we know, is the largest one on the subject so far, provides insights into the comparison of short-term outcomes between robotic and laparoscopic gastrectomies in patients with gastric cancer. Marano et al. 9 aggregated 14 meta-analyses published until December 2019 and showed better results in favor of robotic surgery, regarding blood loss, length of hospital stay, recovery of bowel function, distal resection margin distance, and number of retrieved lymph nodes. However, not all represented an acceptable level of evidence, concerning the high percentage of heterogeneity of some outcomes. Hence, it is still unclear if RG is more feasible and safer than LG.
Our results demonstrated that both surgical techniques are similarly effective in term of conversion rate, reoperation rate, mortality, overall complications, anastomotic leakage, distal and proximal resection margin distances, and recurrence rate.
Operative time and cost favor the laparoscopic approach, while blood loss, length of hospital stay, time to first flatus, time to oral intake, surgical complications (CD grade ≥III), pancreatic complications, and the number of retrieved lymph nodes favor the robotic approach.
Surgical outcomes
Operative time
This meta-analysis shows a similar result to previous studies, which demonstrated that operative time is significantly longer in RG when compared with LG.9,11,12
Some studies have suggested that the learning curve associated with the use of robotic technology and the need for instrument exchange during the procedure may contribute to the longer operative time seen in the robotic surgery group. 68
As Gong et al. 8 refer, the majority of studies did not discriminate the several steps of the surgery, regarding the operative time. Nishi et al. 40 and Ye et al. 65 divided the operative time into different steps of the surgery, which demonstrated that robotic surgery is not inferior regarding the effective operative time. However, the total operative time, which includes the effective time and “junk time” (setup, docking, and adjustment of surgical instruments), remains longer in robotic surgery due to the latter.65,69
There were two studies demonstrating a shorter operative time in the robotic surgery group, one of them (Omori) with a statistically significant difference.40,45 Omori et al. 45 applied relevant techniques to shorten the “junk” time, such as the standardization of the setup and the use of MBS and SPIDER techniques, which reduce pancreatic manipulation during lymphadenectomy.
So the early standardization of the setup as well as the surgical team's experience could contribute to similar results between both technical approaches.26,40 On the other hand, there appear to be more possible factors that influence the operative time, rather than the docking time, 46 such as the more accurate and delicate lymphadenectomy provided by the robotic platform.15,45
Blood loss
The mean blood loss was significantly lower in the robotic surgery group, compared to the laparoscopic surgery group. This result was also observed in previous systematic reviews. 9 The majority of studies included in our meta-analysis demonstrates a tendency to lower blood loss in robotic surgery. However, there were some studies that showed the opposite and stated that robotic surgery still has some instrumental limitations.22,55
The reasons for the significant difference in intraoperative blood loss could be due to reduction of the physiologic tremor, increased surgical field with 3D view, which provides greater instrument dexterity, and more precise and less damaging dissection. These allow for a more accurate lymphadenectomy, less blood loss, less pancreatic damage, and less muscle trauma.65,70
Conversion/reoperation/mortality
Conversion, reoperation, and mortality were found to be comparable between the 2 groups. There was a tendency to favor the robotic surgery group, regarding conversion and reoperation, and previous studies also presented similar results with no statistically significant difference.8,11,12 There were four studies that demonstrated more cases of conversion to open gastrectomy in the robotic surgery group, with the following causes: intra-abdominal bleeding, serosa involvement, massive abdominal adhesion, damage to adjacent organs with the insertion of trocars, inadequate surgical margins, and anatomical and dissection difficulties.20,33,47,48 Some studies reported the causes of reoperation, such as anastomotic or intra-abdominal bleeding, pancreatic complications (postoperative pancreatic fistula), and intestinal obstruction.34,65
The mortality rate was also found to be similar between the 2 groups. This holds true in this study, with the laparoscopic surgery group displaying a mortality of 0.59%, and the robotic surgery group displaying a value of 0.60%. These findings are consistent with previous studies. 9
Perioperative outcomes
Length of hospital stay/time to first flatus/time to oral intake
The length of hospital stay, time to first flatus, and time to oral intake are outcomes associated with a faster recovery, as well as lower probability of intrahospital complications and better patient well-being.
This study showed significant results favoring robotic surgery, which appears to cause less damage to adjacent organs, less blood loss, and fewer postoperative complications. This finding supports the intrinsic advantages of the robotic platform, resulting in less trauma and, therefore, shorter time to recovery.
The mean of length of hospital stay was 8.74 days in the robotic surgery group and 9.38 days in the laparoscopic surgery group. Similar results can be seen in Hu et al., without significant heterogeneity. 71
In fact, Liu et al. correlate the shorter hospital stay in the robotic surgery group with a better bowel function recovery and a faster shift from liquid to soft diet. In addition, the surgical operation area and the inflammatory response can influence gastrointestinal recovery, due to surgical manipulation of internal organs.37,65 Moreover, Guerrini et al. referred the importance of early oral feeding in accelerating the recuperation process. 12
Overall complications
Regarding overall complications, they did not differ considerably between both surgical approaches, despite a tendency for lower overall complications in the robotic surgery group. These results were also observed in other meta-analyses.8,12 However, Jin et al. claimed to be the first meta-analysis to demonstrate fewer overall complications in the robotic surgery group with statistical significance. 11 Nevertheless, the possible cause of this observation remains unclear. They still add that this could be related with the statistically significant result in pancreatic complications. 11
Omori et al. demonstrated, by multivariate analysis, that laparoscopic surgery is an independent risk factor for postoperative complications. 45
Surgical complications (grade ≥III in the CD classification)
Several studies applied the CD classification to highlight the most severe complications, which have the most impact in postoperative morbidity and mortality. In fact, Guerrini et al. emphasized the importance of separate medical and surgical complications, because of a direct relation between surgical complications and postoperative recovery and prognosis. 12 Tian et al. showed that surgical complications, CD grade III–IV, are independent prognostic factors for both overall survival and relapse-free survival. 59
Furthermore, Hikage et al. established, according to their multivariate analysis, that laparoscopic surgery is an independent risk factor for postoperative complications with a CD grade of III or higher. 22 In this article, these surgical complications were significantly lower in the robotic surgery group, with only 7% heterogeneity (P = .35). The rates of the surgical complications were 3.88% in the robotic surgery group and 6.39% in the laparoscopic surgery group. These observations are consistent with those of Guerrini's meta-analysis. However, our results presented slightly lower rates of surgical complications. 12 Hence, RG results in less relevant morbidity.
Anastomotic leakage
This study did not show a statistically significant difference in anastomotic leakage, which is congruent with previous studies. 12
Pancreatic complications
Pancreatic morbidity is relatively rare. Nevertheless, it represents a real threat to the patient. 72 One of the main concerns of gastrectomy is pancreatic manipulation during lymphadenectomy. 58
Jin et al. and Gong et al. showed that pancreatic complications were significantly lower in the robotic surgery group.8,11 These results are consistent with our meta-analysis. In addition, Jin et al. discuss the influence of the extension of lymphadenectomy on pancreatic complications as an unexpected inverse relationship between the number of harvested lymph nodes and pancreatic morbidity. 11 In fact, these results support the efficacy and efficiency of the abovementioned characteristics of robotic surgery, which lead to minimization of pressure on the pancreas, as well as reduction on parenchymal injury.16,58,72
Omori et al. used the SPIDER and MBS techniques to optimize the removal of suprapancreatic lymph nodes with an internal organ retractor, which held the pancreas, and a bipolar soft-coagulation forceps, which minimizes thermal damage. 45
Cost
The cost of robotic surgery remains an important drawback to this technique. On average, the total cost of robotic surgery was 3684.27 U.S. dollars (3442.99 Euros), significantly higher compared with laparoscopic surgery. Our meta-analysis includes 8 studies that reach the same conclusion: that the cost of the laparoscopic surgery is significantly lower, compared to that of robotic surgery.9,12
Some studies suggest that the fewer postoperative complications and the faster recovery and hospital stay can compensate for the higher costs associated with robotic surgery.9,59 Moreover, other studies predict a reduction in the cost of robotic surgery over time with an increase in competition and technological improvement.12,19,34
Oncological outcomes
Distal and proximal resection margin distances
Our systematic review mainly includes studies on short-term outcomes. Therefore, it becomes difficult to analyze oncological variables, which demand a longer follow-up. To overcome this problem, we used distal and proximal resection margin distances as predictors for oncologic prognosis. 12
This article did not show a significant difference in either resection margin distance, but there was a small tendency to favor the robotic approach. The mean distal resection margin distance was 6.9 cm in the robotic surgery group and 6.82 cm in the laparoscopic surgery group. Regarding the proximal resection margin distance, RG had a mean of 4.35 cm and LG had a mean of 4.24 cm.
Recurrence
Overall, the recurrence rate was comparable between the robotic and laparoscopic techniques (9.9% and 10.6%, respectively), although it appears to be lower in the robotic surgery group. Only one of the recent included studies analyses recurrence, particularly within 5 years after surgery, and it reported 7 cases of recurrence in 58 patients who underwent LG and 3 cases in 36 patients who underwent RG, with no locoregional recurrence in the robotic surgery group. 22 Han et al. 21 did not report any case of recurrence and the mean follow-up for both surgical groups was <2 years, when recurrence is more common. 73 In fact, recurrence rate can happen in more than half of gastric cancer patients after surgical treatment.74,75 Furthermore, lymphovascular invasion, lymph node metastases, and tumor stage are independent risk factors of early recurrence (≤12 months) after curative resection. 76
Number of harvested lymph nodes
Lymphadenectomy is part of the standard treatment, and it is one of the main steps of the surgery, regarding the difficulty on managing and dissecting around critical organs, such as the pancreas, and an important predictor of the oncological prognosis, as they determine the extent of the tumor, according the TNM classification.
In our meta-analysis, the number of retrieved lymph nodes was significantly higher in the robotic surgery group, when compared with the laparoscopic surgery group, as demonstrated in previous meta-analysis.8,11,12 All of these studies, including ours, showed a significant heterogeneity, which puts the external validity of their results into question.
In fact, some studies40,59 revealed a significantly higher number of harvested lymph nodes in the robotic surgery group, particularly caused by the retrieval of the suprapancreatic lymph nodes. 59 They attribute these results to the better surgical field, with 3D vision and endowrist movements, and the reduction of the surgeon's physiologic tremor that the robotic platform provides.40,59 Moreover, these differences were more evident in advanced gastric cancer 59 and Jin et al. demonstrated a preference for performing robotic surgery in patients whose body mass index was under 25 kg/m2, whose age was under 65, and who had a tumor with a longest diameter above 5 cm. 11
Several studies defined that an adequate number of retrieved lymph nodes was more than 15.34,49–51 Roh et al. 49 showed that there was an inadequate number of retrieved lymph nodes (<16) in the laparoscopic surgery group and the surgical success, which included this outcome, was significantly higher in the robotic surgery group. Nevertheless, it remained unclear what the real cause of these results was. This robotic surgery had a firefly system that was used for achieving a real-time fluorescence image, during lymphadenectomy, to detect lymphatic drainage and optimize the dissection and retrieval of lymph nodes with more accuracy.
On the other hand, despite the good results of the SPIDER and MBS techniques in reducing pancreatic damage, Omori et al. 45 found that laparoscopic and robotic surgeries are comparable, concerning the number of retrieved lymph nodes, as shown in a randomized control trial. 77 In opposition, another randomized clinical trial (RCT) described a significantly higher number of harvested lymph nodes. 78
Subgroup analysis
There were significant subgroup differences in the following outcomes: operative time, time to first flatus, and anastomotic leakage. Regarding operative time, while both subgroups favored robotic surgery, studies without PSM showed more pronounced differences.
The MD of time to first flatus was higher in the non-PSM subgroup, when compared to that of the PSM subgroup. However, the first subgroup showed higher heterogeneity. These findings demonstrated that PSM reduced both heterogeneity and difference between the robotic and laparoscopic surgery groups. The same happened in the following outcomes: conversion, time to oral intake, surgical complications (CD Grade ≥III), cost, and distal resection margin distance. Therefore, this method allows a better understanding of each comparison and a more accurate approximation of reality.
Concerning anastomotic leakage, the significant subgroup differences appear to be due to opposite results. The meta-analysis showed that, in the PSM subgroup, there is a tendency for lower anastomotic leakage when performing robotic surgery. There were other outcomes, which also showed results favoring robotic surgery in the PSM subgroup, in comparison with those in the non-PSM subgroup, such as blood loss, reoperation, overall complications, proximal resection margin distance, and recurrence. However, none of these outcomes demonstrated any significant difference between subgroups.
There were also outcomes where the PSM method did not reduce the heterogeneity of included studies. In fact, there were higher values of heterogeneity in the PSM subgroup regarding operative time, length of hospital stay, overall complications, pancreatic complications, and number of retrieved lymph nodes.
In addition, length of hospital stay and surgical complications with a CD Grade ≥III showed a significant difference only in the PSM subgroup.
On the one hand, PSM subgroups were more consistent and did not emphasize the differences between both surgical approaches. On the other hand, in certain outcomes, these subgroups demonstrated results that were more supportive of robotic surgery, highlighting its advantages when compared with laparoscopic surgery.
The demographic characteristics of people who underwent PSM were not equal in every study. Therefore, it is still possible that there are variables that did not undergo PSM and are affecting the validity of the results, in terms of heterogeneity.
This study also has some limitations: first, we included nonrandomized comparative studies; second, several outcomes demonstrated a high percentage of heterogeneity, which may put the validity of results into question. These differences between studies could be explained by discrepancies in the surgical team's experience in performing robotic surgery; third, about half of the studies included did not perform PSM, contributing to the influence of confounding factors on the results and conclusions about the outcomes in study; fourth, there was one article that we could not access, resulting in a slight reporting bias; fifth, the majority of the included studies is from Southeast Asia (Japan, China, and Korea), which may not be representative of the global reality; and sixth, postoperative inflammatory reaction and drain amylase levels, which could improve the assessment of pancreatic damage, were not included.
Conclusion
In conclusion, we believe that our results demonstrate RG is a safe and feasible procedure, when compared with LG.
Overall, robotic surgery presented better results regarding blood loss, length of hospital stay, time to first flatus, time to oral intake, relevant surgical complications, pancreatic complications, and the number of retrieved lymph nodes. However, operative time and financial cost remain the main drawbacks to its widespread use. Further studies are needed to understand mechanisms to minimize these downsides, aiming for a more efficient use of the robotic platform in gastric cancer curative-intent surgery.
Moreover, randomized clinical trials are also desired in contemplation of a better comprehension of advantages in performing RG.
Footnotes
Authors' Contributions
P.L.: conceptualization (equal); data curation (equal); formal analysis (equal); investigation (equal); validation (equal); visualization (lead); writing—original draft (lead); and writing—review and editing (equal). J.P.B.: data curation (equal); formal analysis (equal); investigation (supporting); resources (lead); supervision (supporting); validation (equal); visualization (supporting); writing—original draft (supporting); and writing—review and editing (equal). J.F.V.: investigation (equal) and validation (equal). J.B.: conceptualization (equal); investigation (supporting); supervision (lead); visualization (supporting); and writing—review and editing (supporting).
Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
No funding was received for this project.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.