
Abstract
Introduction and Objective:
Laparoscopy is the most widely followed approach in ablative or reconstructive kidney surgeries. The aim of this study is to assess the utility and safety of laparoscopic approach in pelvic ectopic kidney surgeries.
Methods:
Between July 1, 2021 and June 30, 2022, 8 patients with pelvic kidneys; 4 with pelviureteric junction obstruction, 3 with pelvic stones, and 1 nonfunctioning kidney underwent laparoscopic pyeloplasty, pyelolithotomy, and nephrectomy, respectively. The records of all 8 patients were evaluated retrospectively for analyzing the operating time, blood loss, postoperative hospital stay, intra- and postoperative complications, surgical difficulty, and the success in completing the case laparoscopically. The patients were followed for at least 6 months to know the outcome. After pyeloplasty the improvement in function and drainage as well were recorded.
Results:
Of 8 cases, 6 (75%) were completed laparoscopically. One pyelolithotomy and 1 pyeloplasty patient were converted to open surgery. The median operative time was 180 (140–240) minutes, median blood loss was 100 (50–300) mL, and median hospital stay was 4 (3–6) days. One patient, who had open conversion, had Clavien grade I complication in the form of prolonged fever. Pyeloplasty patients at 6 months follow-up showed improvement in symptoms as well as function.
Conclusion:
The laparoscopic approach has obvious benefits in pelvic surgeries. Laparoscopy for ectopic pelvic kidneys are challenging due to abnormal anatomy of vessels and kidneys. Proper exposure of kidneys and exact identification of vessels can accomplish laparoscopic procedure in ectopic kidneys successfully with patients having nil complications and early convalescence.
Introduction
Ectopic kidney as a congenital anomaly has an incidence in between 1 in 2200 and 1 in 3000. 1 Ectopic kidney may have different positions in retroperitoneum such as abdominal, lumbar or pelvic, the latter being the most common (55%). 2 Ectopic pelvic kidneys are usually incidentally detected and are asymptomatic, but they can have pathological conditions such as pelvi-uretero junction obstruction (PUJO) and nephrolithiasis.1,3 The anatomy and the vascular supply is usually abnormal in such kidneys and becomes challenging if any surgical intervention is needed in such cases. 4 Laparoscopic approach in such kidneys becomes a challenge as intraoperative problems and dilemmas may arise due to unpredictable anatomy, abnormal renal vessels, uncertainty of ureter course, narrow confines, and restricted access of the true pelvis. 5 The aim of this study is to describe our experience of laparoscopic intervention in treating various pathologies in ectopic pelvic kidneys.
Materials and Methods
It is a retrospective study, which was performed at the Smt GR Doshi and KM Mehta Institute of Kidney Disease and Research Centre (IKDRC) Ahmedabad. The study proposal was approved by the Institution Ethics committee, IKDRC, Ahmedabad. Total 8 cases with ectopic pelvic kidney, 4 with PUJO and 3 with renal pelvic calculi, and 1 with nonfunctioning kidney, who underwent laparoscopic surgical intervention between July 1, 2021 and June 30, 2022, were included in the study. These patients underwent laparoscopic pyeloplasty, pyelolithotomy, and nephrectomy.
The parameters that were analyzed were outcome, morbidity, hospital stay, operative time, blood loss, and any intraoperative complications. The radiological investigations carried out were X ray kidney ureter and bladder, ultrasonography (USG) abdomen, and contrast-enhanced computed tomography (CECT). X-rays are helpful in quantifying stones and in follow-up and USG as an initial screening test. CECT abdomen along with angiography was done in all cases to get information about the abnormal anatomy, including the aberrant vascular supply and orientation and position of the pelvis and ureter.
All patients underwent laparoscopy under general anesthesia in Trendelenburg position. Patient for reconstructive procedure underwent preoperative retrograde pyelography (RGP) for a better understanding of ureteral course and surgical planning. The pneumoperitoneum was created by Veress needle at the left palmar point. Three ports were used in all cases: a 10 mm camera port in the midline 2–4 cm above umbilicus and two working ports at the level of umbilicus, 10 mm at the right mid-clavicular line and a 5 mm at the left mid-clavicular line (Fig. 1).

Port position: patient in Trendelenburg position with three ports. Ten millimeter camera port in the midline. Two working ports, 10 mm at the right mid-clavicular line and a 5 mm at the left mid-clavicular line.
Laparoscopic pyeloplasty
All patients planned for pyeloplasty underwent RGP beforehand. Then the patient was placed in the Trendelenburg position. There were no prior Double-J stents or any catheter inserted. As all pelvic kidneys were left sided, after the ports insertion, sigmoid colon was mobilized and pelvic kidney was exposed. Renal pelvis was identified first and ureter was dissected distally (Fig. 2). In 3 out 4 pyeloplasties the pelvis was facing anteriorly. In the remaining one it was left posterolateral in the direction (Fig. 3). The pelviureteral junction was dismembered and ureter was spatulated posteriorly as pelvis was facing anterior and pyelotomy was anterior. Any vessel encountered was meticulously dissected and preserved. Pyeloplasty was done using 4-0 braided polyglactin suture. Double-J stent was placed antegradely.

Laparoscopic pyeloplasty in ectopic pelvic kidney.
CT image of patient with pelviureteral obstruction in which pelvis was facing posterolateral.
Laparoscopic pyelolithotomy
After performing RGP and confirming the stone position under fluoroscopy, patient was placed in Trendelenburg position. Initial steps were similar to pyeloplasty up till exposure of pelvis. As marked hydronephrosis was not present as in PUJO cases, ureter was first identified and dissected proximally till the renal pelvis. Pyelotomy was done and calculi were extracted and placed in a plastic bag and retrieved. A Double-J stent was placed and pyelotomy was repaired by 4-0 polyglactin.
Laparoscopic nephrectomy
In the single patient who underwent laparoscopic nephrectomy, the kidney was grossly hydronephrotic and sigmoid colon was pushed toward right (Fig. 4). The kidney was lying over the major vessels and was dissected. There was a single renal artery arising from the common iliac artery and single renal vein draining in the internal iliac vein (Fig. 5). The vessels were clipped and divided. After dissecting the kidney away from the body, the ureter was dissected and clipped near the bladder and divided. The specimen was bagged in a locally made plastic bag and was retrieved from a 5 cm lower midline incision.
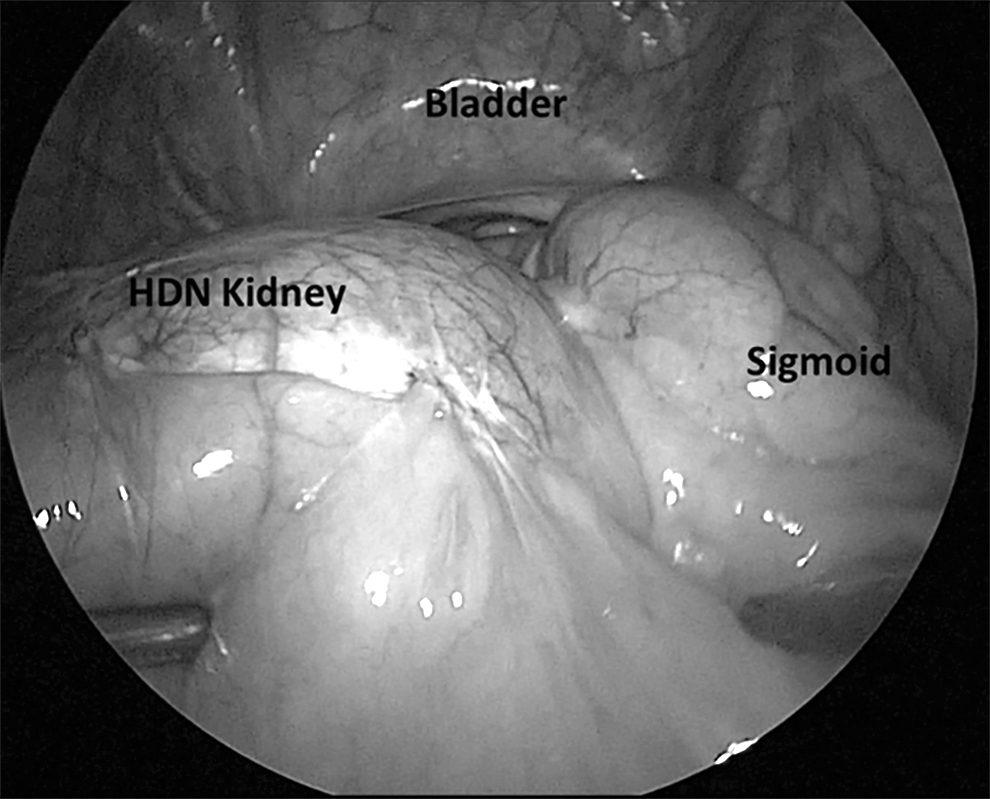
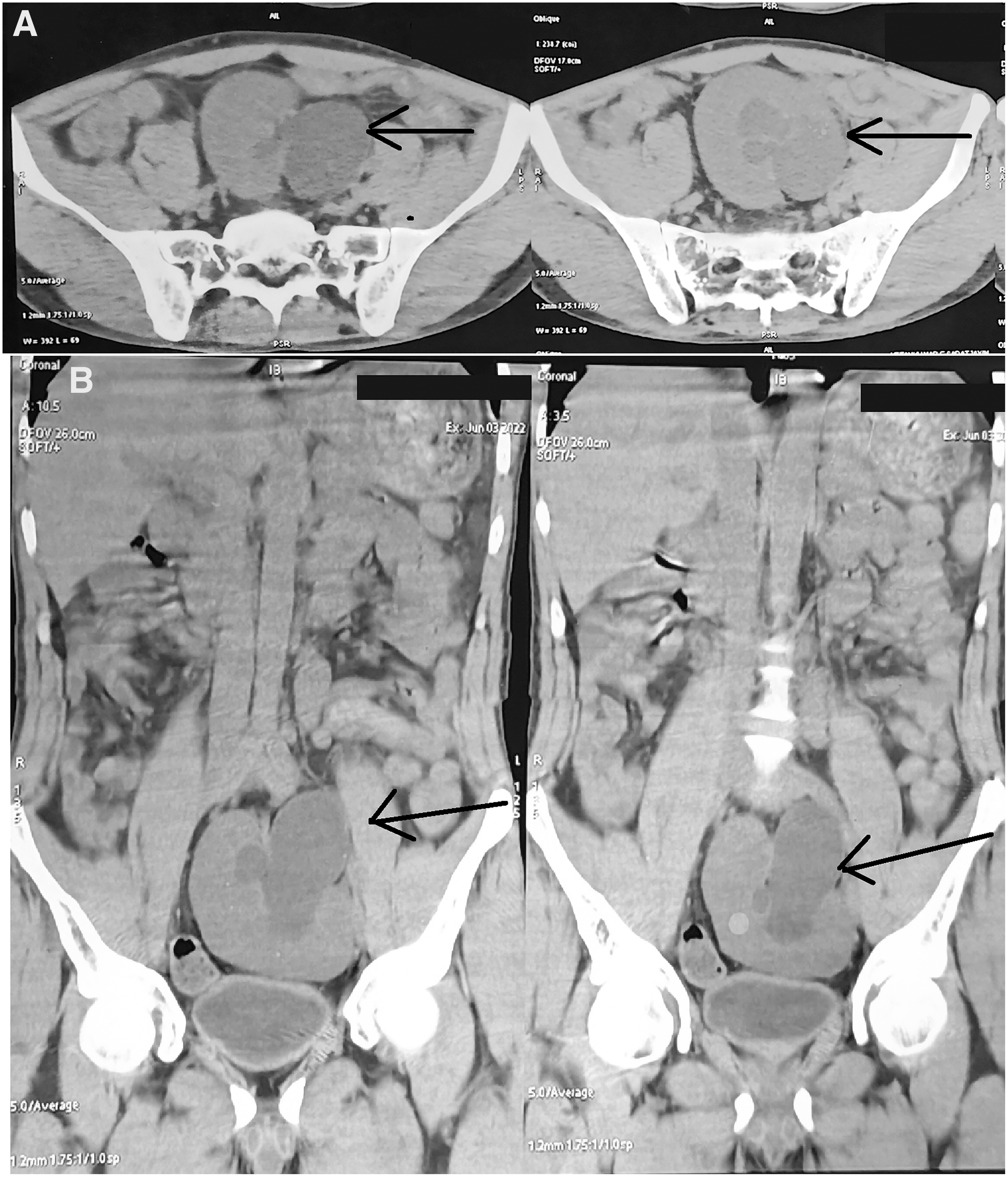
Grossly hydronephrotic nonfunctioning kidney pushing sigmoid colon toward right.

Aberrant renal artery (grey arrow) originating from common iliac artery and renal vein (black arrow) draining in the internal iliac vein.
Result
Among 8 patients with pelvic kidneys, 6 (75%) were male and 2 (25%) were female. The median age was 29 (17–54) years. All kidneys were left sided. In 1 patient the kidney was in the midline in supravesical region (Fig. 3). The median operating time was 180 (140–240) minutes; median blood loss was 100 (50–300) mL. The median hospital stay was 4 (3–6) days (Table 1). The median creatinine was 1.2 (0.7–1.4) mg/dL. There were no severe complications with none in Clavien–Dindo class 2–5. Six (75%) out of 8 patients were completed successfully by laparoscopic approach. Two (25%) patient were converted to open, 1 was pyelolithotomy, and other was pyeloplasty.
Demographics and Outcomes of Individual Cases with Pelvic Kidneys Who Underwent Laparoscopic Management
Median value (range).
NFK, non functioning kidney; PUJO, pelvi-uretero junction obstruction.
Among 4 patients with pelvic kidneys who underwent laparoscopic pyeloplasty, there was no crossing vessel reported in any case. All patient postoperatively were relieved of symptoms. In nuclear scans, median improvement in the glomerular filtration rate (GFR) was 3.5 mL/min/1.73 m2 at 6 months of follow-up. Three patients who underwent pyeloplasty had improved GFR after 6 months of surgery. One patient who had converted to open had unchanged GFR at follow-up. There was improvement in the drainage in all patients in the postoperative scans. One patient who had midline supravesical pelvic kidney had to be converted to open approach as the pelvis was facing left posterolateral and not easily accessible laparoscopically (Fig. 3). It was the single functioning kidney for the patient.
In 3 patients with renal pelvic calculi, 2 patients had solitary stones with sizes 2 and 3 cm, respectively. One patient had multiple (five) calculi, largest stone being 4 cm in size. Laparoscopic pyelolithotomy was successfully performed in 2 patients. The patient with multiple calculi had to be converted to open surgery because of deep renal pelvis, which was not easily reachable and doubts about stone clearance.
In a single patient who had nonfunctioning pelvic kidney, the etiology was PUJO. The kidney was hydronephrotic measuring ∼8 cm (Fig. 6). It had aberrant vascular supply, but the nephrectomy was comparatively easier as compared with the reconstructive procedures.

CT image of hydronephrotic nonfunctioning kidney. CT, computed tomography.
Discussion
Kidneys originate from metanephros in the sacral region. 6 During embryological development at 6–9 weeks, the metanephros ascends to lumbar region and simultaneously rotates medially from anteriorly along its long axis. Incomplete renal ascent leads to ectopic kidneys and when the kidney does not ascent at all, it results in pelvic kidney. Thus, the pelvic kidney has usually anterior facing pelvis, which makes the pelvic reconstruction and suturing easy. The blood supply of the primitive kidney arises from transient aortic off-shoots, which degenerates subsequently. 7 When these fail to degenerate in ectopic kidney, aberrant blood supply results, which may arise from middle sacral artery, iliac arteries, aortic bifurcation, or aorta. 8 The knowledge of such aberrant vessels beforehand helps in proper surgical planning.
On reviewing the literature, we found two retrospective studies about the laparoscopy in pelvic kidneys. Gupta et al. performed a study of 6 patients with ectopic pelvic kidneys who underwent laparoscopic intervention. 8 In their study, 2 patients each had PUJO, renal pelvic calculi and nonfunctioning kidneys who underwent laparoscopic pyeloplasty, pyelolithotomy and nephrectomy, respectively. All patients underwent laparoscopy in 45° lateral position.
Similar to our study, there was left preponderance with all 6 patients having left-sided pelvic kidneys. The follow-up period was 12 months. In this study, 5 out of 6 (83.3%) patients were completed laparoscopically successfully. One pyelolithotomy was converted to open approach due to thick and adherent mesocolon to renal pelvis, difficult to reach stone and bleeding from the edematous renal pelvis. The hospital stay, mean operative time, blood loss, perioperative complications, and other parameters were comparable as in our study. This study suggested that, as opposed to pyeloplasty and nephrectomy, reaching renal pelvis was difficult in pyelolithotomy.
In another retrospective study done by Muller et al., 5 pediatric patients with ectopic pelvic kidneys underwent laparoscopic pyeloplasty. 9 Among these 2 had left, 2 had right, and 1 had retrovesical pelvic kidney. Just like our study, the patients were operated in supine position with 30° upward tilt to left and camera port at umbilicus and working ports at mid-clavicular line, one above and another below umbilicus. Fourth port was used in 2 cases to improve the exposure. Four (80%) patients had successful laparoscopy. Postoperative morphological and functional evaluation was done by USG, magnetic resonance urography, and dimercapto succinic acid nuclear renography. The mean follow-up was 3.3 (2–5.6) years. All patients had improved morphology with equivalent function during follow-up.
In our study, 8 patients with ectopic pelvic kidney underwent laparoscopic intervention. All the kidneys were left-sided ectopic kidneys with ureter opening on left side of the trigone. All patients were operated in Trendelenburg position as opposed to in study by Gupta et al. where patients were operated in lateral position. 8 In lateral position, bowel is mobilized unilaterally and it falls to midline. In contrast, Trendelenburg position can provide wide accessibility to pelvis. This can make accessibility to the aberrant vessels in pelvic kidneys easier as compared with operating patients in lateral position. Six patients were managed successfully, whereas 2 patients had to be converted to open due to difficult anatomy with pelvis facing lateral and being inaccessible.
Both of these patients had relatively longer operating times, more blood loss and prolonged hospital stay as compared with other cases in the study. The subjective requirement for analgesia was also more in these 2 cases as analgesic dose was prolonged as compared with others. It may be due to prolonged pain at the open surgical site. All pyeloplasty patients showed improved drainage and symptoms at 6 months follow-up. Optimal imaging in the form of CT angiography and RGP helped in the proper planning of the surgery. In patient with midline supravesical kidney, RGP suggested that the ureter was opening on the left side of the trigone. Thus, RGP can diagnose the laterality of the kidney as well. The comparison of three studies is shown in Table 2.
Comparison of Different Studies Related to Laparoscopy in Ectopic Pelvic Kidneys
DMSA, dimercapto succinic acid; GFR, glomerular filtration rate; MRuro, magnetic resonance urography.
In a metanalysis studying the side distribution of different renal malformation, it was found that in 232 cases of unilateral renal ectopia included in six studies, 56.9% were on the left side. 10 The ectopic pelvic kidneys have a slight predominance on the left side. 11 It is interesting to note that in Indian studies there was a strong preponderance of ectopic pelvic kidney being left sided as found in our study and also by Gupta et al. 8 In both studies, total 14 patients with pelvic kidneys got operated and all of them were left sided as opposed to the literature. The exact cause of such lateralization is unknown, but it could be due to varied gene expression or environmental factors such as hypoxia. 10 Well-planned studies can delineate the cause for strong left-sided predominance of ectopic pelvic kidney in this geographical region.
Conclusion
Ectopic pelvic kidney has a strong predominance on left side. Laparoscopic approach is suitable in the management of ectopic pelvic kidney pathology and can be performed in supine position successfully. Preoperative imaging, including RGP, can provide important information about the aberrant anatomy in pelvic ectopic kidneys. Frequent laparoscopy in pelvic kidneys can help in making it standard of care.
Footnotes
Authors' Contributions
Conceptualization by S.J.R. Data curation by K.M. and M.K.B. Formal analysis by K.M., S.J.R., and M.K.B. Methodology and project administration by S.J.R. and P.R.M. Writing—original draft by K.M. and S.J.R. Writing—review and editing by all authors.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.