
Abstract
Purpose:
This study aimed to evaluate the effect of laparoscopic gastrectomy (LG) and open gastrectomy (OG) on clinical outcomes in patients with remnant gastric cancer (RGC).
Materials and Methods:
The databases of PubMed, EMBASE, and Cochrane Library were used to search for eligible studies from inception to April 1st, 2023. Hazard ratios (HRs), mean difference (MD), odds ratios (OR), and 95% confidence intervals (CIs) were pooled up to analyze. The Newcastle-Ottawa Scale (NOS) scores were used to evaluate the quality of the included studies. This study was performed with RevMan 5.3 (The Cochrane Collaboration, London, United Kingdom) software.
Results:
A total of 11 studies involving 535 RGC patients were included in this study. In terms of basic information, we found that the OG group had a higher American Society of Anesthesiologists (ASA) grade (≥2) (OR = 0.24, I2 = 54%, 95% CI = 0.08–0.71, P = .01) than the LG group. In terms of postoperative outcomes, we found that the LG group had longer operative time (MD = 33.95, I2 = 58%, 95% CI = 15.05–52.85, P < .01), shorter postoperative hospital stay (MD = 5.08, I2 = 84%, 95% CI = −9.74 to −0.42, P = .03), shorter length of incision (MD = −7.15, I2 = 94%, 95% CI = −10.99 to −3.31, P < .01), earlier food intake (MD = −3.09, I2 = 76%, 95% CI = −4.84 to −1.35, P < .01), and earlier time to first flatus (MD = −0.84, I2 = 0%, 95% CI = −1.09 to −0.59, P < .01). We found that there was no statistically significant difference in overall survival (HR = 0.96, I2 = 0%, 95% CI = 0.48–1.93, P = .92) between the LG group and the OG group.
Conclusion:
LG for RGC patients had longer surgical time, shorter postoperative hospital stay, shorter length of incision, earlier food intake, and earlier time to first flatus.
Introduction
Gastric cancer is the third most common cause of cancer-related deaths in males worldwide and the fifth most common cause in females. 1 Remnant gastric cancer (RGC) is defined as cancer that occurs in the remnant stomach after subtotal gastrectomy due to benign diseases or cancer.2–4 Compared with gastric cancer, the incidence of RGC is relatively low. According to reports, RGC accounts for 1%–8% of all gastric cancers.5–7
Due to the improved survival rate after radical gastrectomy for the treatment of peptic ulcers and cancer, 8 there is an increasing number of RGC being discovered at a resectable stage.9,10 Although chemotherapy and radiation therapy have rapidly developed in the field of cancer treatment, for resectable RGC, gastrectomy combined with sufficient lymph node (LN) resection is still the preferred treatment option.8,11,12
With the advancement of endoscopic surgical instruments and the understanding of microsurgery, laparoscopic gastrectomy (LG) has become widespread.13,14 LG is gradually accepted in clinical practice due to its less invasiveness and shorter recovery time compared to open gastrectomy (OG).15,16 However, there was no clear conclusion on the clinical outcomes of the surgical approach for RGC. Thus, this study aimed to investigate the effect of the surgical approach on RGC. For this purpose, we compared the clinical outcomes of LG and OG patients with RGC.
Materials and Methods
This study was conducted by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 17
Search strategy
PubMed, EMBASE, and Cochrane Library were searched from inception to April 1st, 2023. The following keywords related to RGC were used for the search: “remnant gastric cancer” OR “gastric remnant cancer” OR “gastric stump cancer.” As for laparoscopic, the search strategy was “laparoscopic” OR “laparoscopy.” As for open, the searching strategy was “open” OR “laparotomy.” Then, we combined these items with “AND.” The search was limited to title and abstract. The language available was English. And two authors performed the search independently.
Inclusion and exclusion criteria
The studies were included in this study if they met the following criteria: (1) RGC patients who underwent gastrectomy were included; (2) the comparison between the LG group and the OG group was reported; and (3) clinical outcomes were reported. The exclusion criteria of this study were as follows: (1) Conferences, reviews, letters, comments, or case reports, duplicated publication data; and (2) insufficient data for analysis. All disagreements about inclusion and exclusion were solved by group discussion.
Study selection
Two authors searched the database independently. First, after removing the duplicate records, the titles and abstracts were screened. Second, the full texts were evaluated for eligibility based on the inclusion and exclusion criteria. The final judgment was made after the group discussion.
Definition
Postoperative complications of this study were classified according to the Clavien-Dindo classification and severe postoperative complications were defined as grades ≥III. 18
Data extraction
The data of this study were extracted as follows: (1) Studies' information, including the publication year, the first author's name, country, sample size, and study design; (2) patients' baseline information, including age, sex, body mass index (BMI), American Society of Anesthesiologists (ASA) grade, comorbidity, original disease, previous surgical approach, primary reconstruction, time interval, histologic type, location, Tumor Node Metastasis (TNM) stage, tumor size, and number of retrieved LN and number of metastatic LN; and (3) postoperative clinical outcomes, including operative time, postoperative hospital stay, blood loss, length of incision, food intake, time to first flatus, anastomotic leakage, pancreatic fistula, intra-abdominal infection, surgical site infection, anastomotic stenosis, pneumonia, postoperative bleeding, major complications, overall complications, and overall survival (OS).
Quality assessment
The Newcastle-Ottawa Scale (NOS), which had a score ranging from zero to nine points, was used to assess the quality of enrolled studies. 19 A study with a score of nine points was considered high quality, a study with a score of seven to eight points was considered medium quality, and a study with six or fewer was considered low quality.
Statistical analysis
Mean differences (MDs) and 95% confidence intervals (CIs) were calculated for continuous variables. Odds ratios (ORs) and 95% CIs were calculated for the postoperative complications. Hazard ratios (HRs) and 95% CIs were calculated for the OS of RGC patients. Statistical heterogeneity was assessed by using the value of I2 and the result of the chi-squared test. If I2 > 50%, it was considered high heterogeneity, the random effect model was used, and P < .1 was considered statistically significant. 20 Funnel plots and Egger tests were also used to observe the heterogeneity of studies and publication bias. This study was performed with RevMan 5.3 (The Cochrane Collaboration, London, United Kingdom).
Results
Study selection
A total of 50 studies were identified in the database, including 30 studies in PubMed, 17 studies in Embase, and 3 studies in the Cochrane Library. After removing duplicate studies and unqualified study type, 28 were left for record screening. After browsing the titles and abstracts, 13 studies were left for full-text scanning. Finally, 11 studies21–31 were included in this study (Fig. 1).

Flowchart of study selection.
Characteristics of the included studies
A total of 11 studies involving 535 patients were included in this study. These studies were published from 2014 to 2022 and the study period was from 1996 to 2021, including 11 retrospective studies. More specific information and the NOS scores are shown in Table 1.
Baseline Characteristics of Included Studies
NOS, Newcastle-Ottawa Scales.
Baseline information between the LG group and the OG group
By comparing the baseline information, we found that there was no significant difference in age (MD = −0.12, I2 = 0%, 95% CI = −2.51 to 2.27, P = .92), sex (OR = 0.94, I2 = 0%, 95% CI = 0.57–1.56, P = .82), BMI (MD = −0.24, I2 = 0%, 95% CI = −1.00 to 0.52, P = .54), comorbidity (OR = 0.53, I2 = 8%, 95% CI = 0.23–1.24, P = .15), original disease (OR = 0.91, I2 = 4%, 95% CI = 0.59–1.40, P = .66), primary reconstruction (P > .05), time interval (MD = 8.53, I2 = 0%, 95% CI = −0.64 to 17.69, P = .07), histologic type (OR = 0.75, I2 = 0%, 95% CI = 0.40–1.40, P = .36), location (OR = 0.75, I2 = 0%, 95% CI = 0.41–1.35, P = .33), TNM stage (P > .05), tumor size (MD = −7.80, I2 = 0%, 95% CI = −16.46 to 0.87, P = .08), number of retrieved LN (MD = 1.35, I2 = 72%, 95% CI = −1.99 to 4.68, P = .43), or number of metastatic LN (MD = −0.47, I2 = 0%, 95% CI = −1.01 to 0.07, P = .09).
We found that the OG group had higher ASA grade (≥2) (OR = 0.24, I2 = 54%, 95% CI = 0.08–0.71, P = .01) than the LG group (Table 2).
Summary of Characteristics Between the Laparoscopic Gastrectomy Group and the Open Gastrectomy Group
ASA, American Society of Anesthesiologists; BMI, body mass index; CI, confidence intervals; FE, fix effect; LG, laparoscopic gastrectomy; LN, lymph node; MD, mean difference; OG, open gastrectomy; OR, odds ratio; RE, random effect; TNM, Tumor Node Metastasis.
Operative and postoperative complications between the LG group and the OG group
We found that the LG group had shorter length of incision (MD = −7.15, I2 = 94%, 95% CI = −10.99 to −3.31, P < .01) than OG group.
However, was were no significant difference in blood loss (MD = −77.23, I2 = 75%, 95% CI = −167.15 to 12.69, P = .09), anastomotic leakage (OR = 1.39, I2 = 0%, 95% CI = 0.40–4.88, P = .61), pancreatic fistula (OR = 0.76, I2 = 69%, 95% CI = 0.03–22.86, P = .88), intra-abdominal infection (OR = 3.38, I2 = 0%, 95% CI = 0.71–16.03, P = .13), surgical site infection (OR = 0.60, I2 = 0%, 95% CI = 0.06–5.66, P = .66), anastomotic stenosis (OR = 1.01, I2 = 0%, 95% CI = 0.16–6.44, P = .99), pneumonia (OR = 1.07, I2 = 16%, 95% CI = 0.28–4.13, P = .93), postoperative bleeding (OR = 0.71, I2 = 0%, 95% CI = 0.18–2.73, P = .62), major complications (OR = 0.45, I2 = 0%, 95% CI = 0.19–1.06, P = .07), or overall complications (OR = 0.72, I2 = 0%, 95% CI = 0.43–1.23, P = .24) (Table 3).
Operative and Postoperative Complications Between the Laparoscopic Gastrectomy Group and the Open Gastrectomy Group
CI, confidence intervals; LG, laparoscopic gastrectomy; OG, open gastrectomy.
Comparing OS between the LG group and the OG group
There were four studies22,23,26,31 reporting the OS. No statistically significant difference was found in OS between the LG and OG groups (HR = 0.96, I2 = 0%, 95% CI = 0.48–1.93, P = .92) (Fig. 2).

Comparing OS between the LG group and the OG group. LG, laparoscopic gastrectomy; OG, open gastrectomy; OS, overall survival.
Comparing clinical outcomes between the LG group and the OG group
Seven studies21,22,24,25,29–31 reported operative time and four studies21,26,30,31 reported postoperative hospital stay. We found that the LG group had longer operative time (MD = 33.95, I2 = 58%, 95% CI = 15.05–52.85, P < .01) (Fig. 3a) and shorter postoperative hospital stay (MD = 5.08, I2 = 84%, 95% CI = −9.74 to −0.42, P = .03) (Fig. 3b). Three studies21,26,31 reported food intake and three studies22,30,31 reported time to first flatus. We found that LG group had earlier food intake (MD = −3.09, I2 = 76%, 95% CI = −4.84 to −1.35, P < .01) (Fig. 4a) and earlier time to first flatus (MD = −0.84, I2 = 0%, 95% CI = −1.09 to −0.59, P < .01) (Fig. 4a).

Comparing operative time
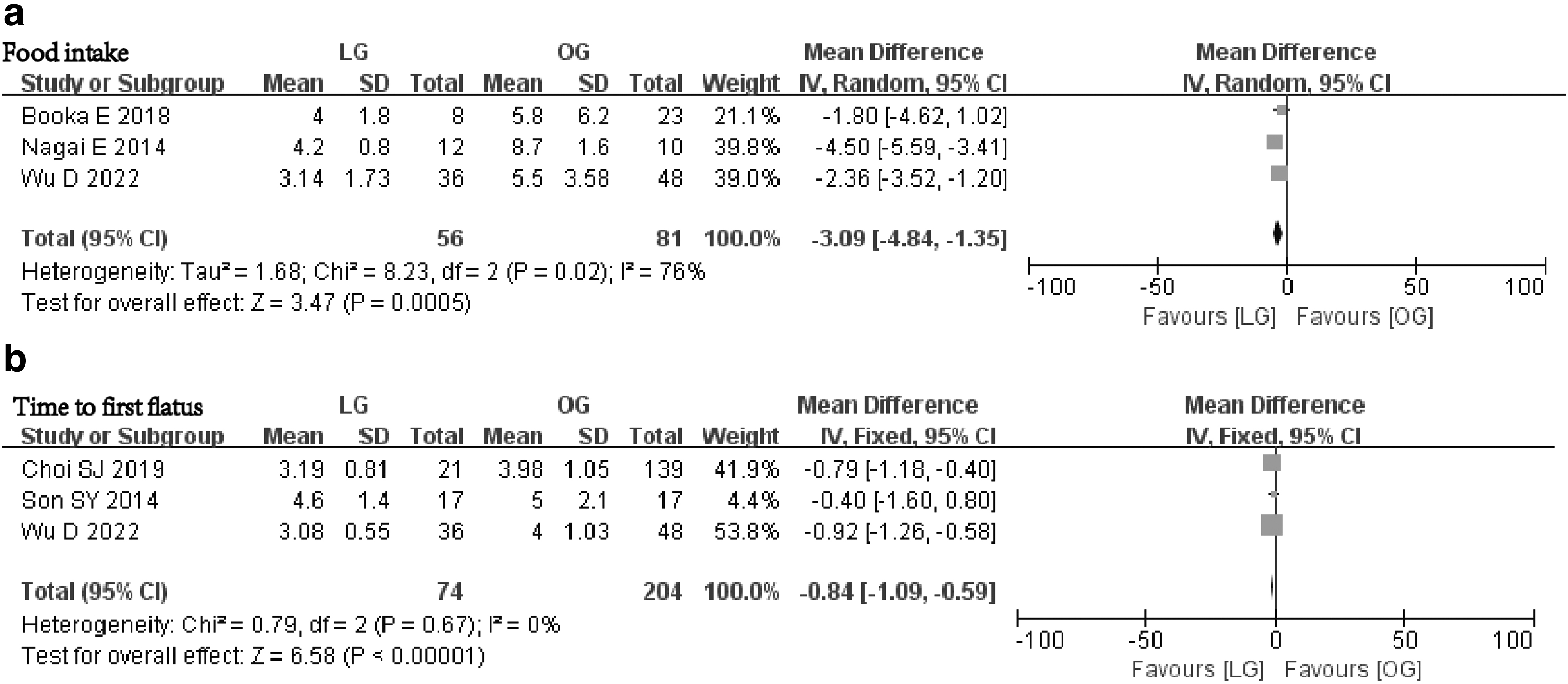
Comparing food intake
Publication bias
Publication bias for the included studies was based on a visual inspection of the symmetrical funnel plot. We developed a funnel plot to reflect the heterogeneity of overall complications for the included studies (Fig. 5).
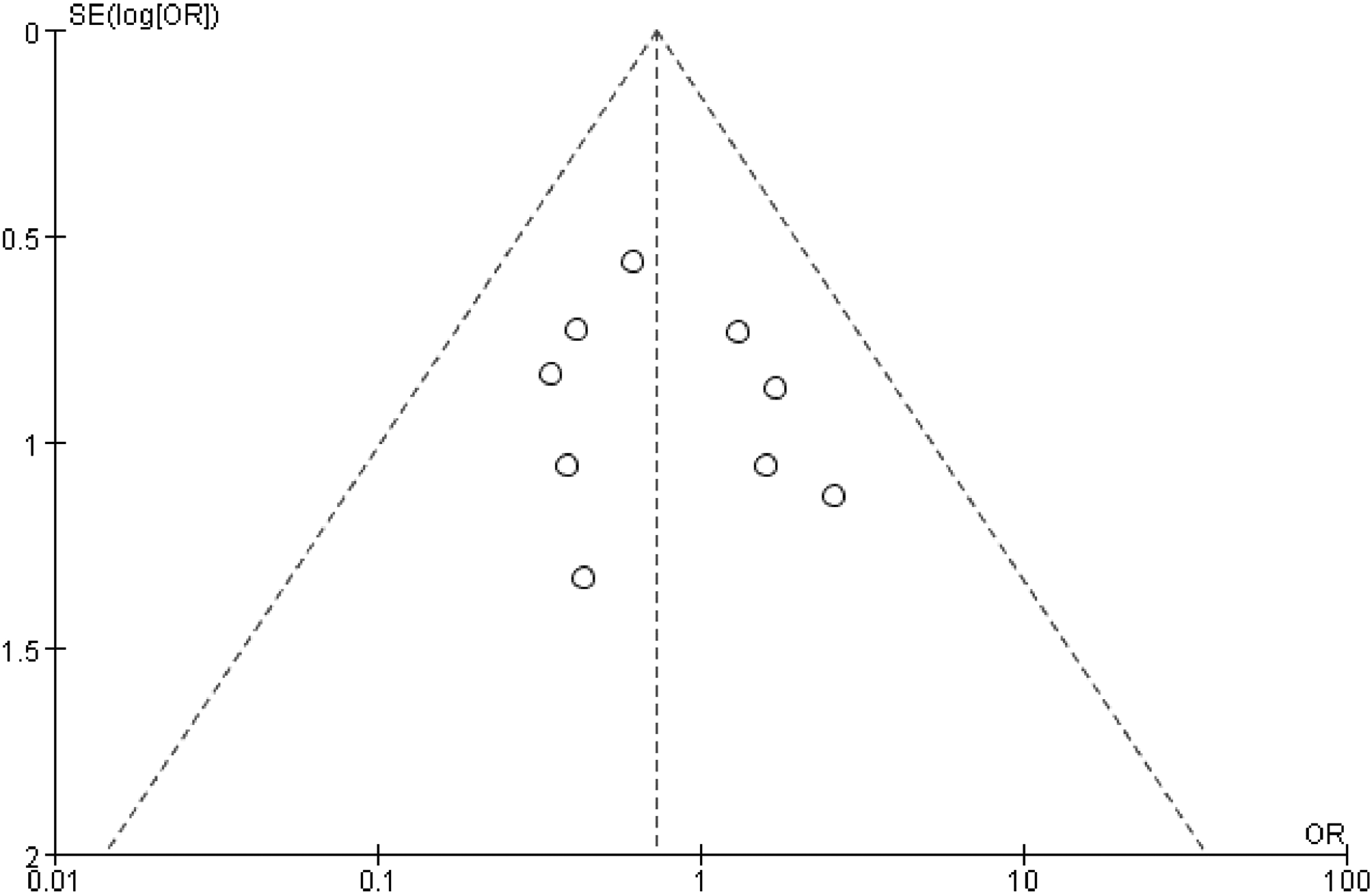
Funnel plot of overall complications.
Discussion
A total of 11 studies involving 535 RGC patients who underwent surgery were included in this study. By comparing clinical outcomes between the LG group and the OG group, we found that the LG group had longer operative time, shorter postoperative hospital stay, shorter length of incision, earlier food intake, and earlier time to first flatus. We did not find a statistically significant difference in OS between the LG group and the OG group.
The safety and feasibility of LG in treating gastric cancer have been proven to be noninferior compared with OG. 32 Therefore, LG treatment for residual gastric cancer was a technically feasible method, and LG could recover earlier compared to open surgery. 24 However, LG for RGC was more difficult than primary cancer due to the technical challenges posed by abdominal adhesions, anatomic displacements, and concerns for radical resection in patients with previous gastrectomy. 26 Yamada et al. 33 reported the first case of LG for the treatment of RGC in 2005. Since then, there was an increasing researcher reporting the effect of LG and OG on the clinical outcomes of RGC treatment.
However, for some clinical outcomes, researchers did not reach a consensus. Booka et al. 21 reported that no statistically significant difference was found in operative time, hospital stay, and food intake between LG and OG. Choi et al. 22 reported that LG had longer operative time than OG, and LG has an earlier time to first flatus. However, there was no difference in postoperative hospital stay between LG and OG. Kwon et al. 24 found that there was no difference in the time to first flatus between LG and OG, and LG had longer operative time, shorter hospital stay, and earlier feeding than OG. Thus, this study aimed to investigate the specific effect of surgical approach on clinical outcomes in patients with RGC.
In our study, we summarized and compared the clinical outcomes of LG and OG patients with RGC. For clinical outcomes that have not reached consensus, we found that the LG group had longer operative time, shorter postoperative hospital stay, earlier food intake, and earlier time to first flatus. The main reason might be due to the difficult operation of LG, which might take longer time than open surgery. However, LG had minimal trauma and low stress response compared to OG. Thus, LG was more conducive to the recovery of gastrointestinal function, early feeding of patients, and accelerating recovery process. 31
To the best of our knowledge, this study was the first pooling up analysis to assess the effect of LG and OG on clinical outcomes in patients with RGC. However, some limitations existed in this study. First, only 11 articles were included in the study, which was relatively small. Second, some of these articles had relatively few cases, and all articles were retrospective studies. Third, all studies came from Asia; thus, these results applied to restricted regions. Therefore, comprehensive, prospective, large sample size, and high-quality randomized controlled trials should be conducted to further confirm our results in the future.
In conclusion, we found that the LG group had longer operative time, shorter postoperative hospital stay, shorter length of incision, earlier food intake, and earlier time to first flatus. Due to the difficulty in treating RGC with LG, we suggested that the surgery should be performed by an experienced laparoscopic surgeon.
Footnotes
Acknowledgments
We acknowledge all the authors whose publications are referred to in our article.
Authors' Contributions
Data extraction, Y.-Y.Q. and F.L.; quality assessments, X.-R.L. and W.Z.; data analysis, Z.-W.L. and Y.-Y.Q.; writing-origin draft, Z.-W.L.; and writing-review and editing, Z.-W.L., Y.-Y.Q., and D.P. All authors read and approved the final article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.