
Abstract
Background:
To determine the perioperative quality assessment results and learning curves for robot-assisted anatomical lung resection.
Methods:
We analyzed the data of the initial 400 patients who underwent lobectomies or segmentectomies by 1 surgeon from January 2020 to November 2021. The learning curve was analyzed using cumulative sum analysis.
Results:
The surgical experience was divided into an initial phase (1st–40th procedures), a transition phase (41st–131st procedures), and a proficient phase (132nd procedure onward). The operative time showed a conspicuously continuous improvement over the 400 consecutive patients. After the 120th procedure, there were significant improvements in the rate of persistent air leakage (11.7% versus 3.9%; P = .003), chest tube duration (3.92 ± 1.91 versus 2.99 ± 1.31, P = .00), and postoperative hospital stay (6.22 ± 2.02 versus 4.93 ± 1.44, P = .00).
Conclusions:
In conclusion, 40 patients were necessary to pass the learning curve, and technical proficiency with favorable perioperative outcomes was achieved after 120–130 patients.
Introduction
Thoracic minimally invasive surgery has been the common treatment for lung resection owing to improved perioperative results, such as postoperative pain and morbidities.1–3 Compared with other minimally invasive surgeries, robot-assisted thoracic surgery (RATS) has favorable postoperative results and potential survival benefits. 4 Although the first robot-assisted lobectomies were reported in 2003 and the first robot-assisted segmentectomies were described in 2007, the application of robot-assisted thoracic technology remains limited.5,6
When implementing a new surgical technique, new adopters need to perform enough to achieve consistent safety and efficacy, which is referred to as the learning curve. A case series showed that the learning curve of robot-assisted lobectomies ranged from 14 to 40 patients.7–12 Nevertheless, these reports were hindered by a lack of consistent methodology, small sample sizes, and the shortcomings associated with retrospective data collection. These studies were mainly focused on the decrease in operating time; however, the operating time does not adequately reflect the true learning curve. Perioperative complications related to the technique itself should also be considered when assessing technical skills for acquiring surgical proficiency.
In this study, we analyzed our experience during the first 400 consecutive robot-assisted anatomical lung resections for non–small cell lung cancer (NSCLC). The aim of this study was to analyze the number of patients required to achieve surgical proficiency while maintaining patient safety and operative quality.
Patients and methods
This study was approved by the Institutional Review Board of the Second Affiliated Hospital of Harbin Medical University (No. IRB-2019-188), and informed consent was waived. We reviewed prospectively collected data on patients 18 years and older with early-stage primary NSCLC who underwent lung resection with lymph node dissection performed by a single surgical team from January 2020 to November 2021. This phase included the initial 400 robotic lung resections accomplished by a single surgeon with extensive expertise and proficiency in video-assisted thoracoscopic surgery (VATS).
Patients
The selection criteria for lung resection candidates were based on the patient physiological assessment recommended by clinical practice guidelines. 13
Clinical characteristics were collected. The intra- and postoperative results were collected from patient records. The staging was confirmed according to the TNM Classification of Malignant Tumours, Eighth Edition. 14
Surgical technique
RPL/S-3 procedures were used in this study. 15 The surgeon was certified by the surgeon council in Seoul (2019). Patients received intravenous inhalation compound anesthesia, and a double-lumen tube was placed. The 3-arm robotic approach with a Xi Da Vinci robot (Intuitive, Sunnyvale, CA) was used for all patients. The first 8-mm port, which was used for the camera, was located at the 8th intercostal space (ICS) at the level of the anterior superior spine. CO2 insufflation was started with a pressure of 8–10 mmHg. The second 8-mm port was located along the angulus inferior scapulae line at the same horizontal level and 8–10 cm away from the camera port. The third 8-mm port was located at the 6th or 7th ICS at the same horizontal level and 8–10 cm from the camera port. The assistant port was created in the 5th ICS along the midclavicular line using a 12-mm disposable trocar.
The robotic approach used in this study for robotic surgery differs somewhat from conventional approaches. The conventional incision for robot-assisted surgery, as reported in the literature, is generally located at the 9th or 10th ICS 5–8. In the early stages of performing robot-assisted surgery, we also used this incision layout. However, there were instances where the assistant's use of this incision could lead to interference with the robotic arms. Moreover, different resections of lung lobes or segments necessitated varying incision layouts. We have since relocated the auxiliary incision to just after the 5th ICS along the midline, making it closer to the thoracoscopic auxiliary incision site, which has made the surgical procedure more convenient. Furthermore, our current layout can essentially meet the surgical requirements for lobes and segments in all positions.
For lobectomies, the pulmonary arteries, veins, and bronchi were individually dissected using stapling devices. Systematic lymph node resection was performed. The tunnel technique was used for incomplete fissures. After the surgery, the specimen was extracted with sterile gloves from the enlarged assistant port.
The target bronchus, artery, and vein were identified and divided for segmentectomies. The collapsed lung was re-expanded completely with airway pressure under 20 cm of H2O via pure O2. Single-lung ventilation was continued. Several minutes later, a clear intersegmental plane line was identified. Segmentectomy was performed along the intersegmental plane line with staplers. Mediastinal and hilar lymph node sampling was performed.
Assessment of quality outcomes
The patients were divided into deciles according to the chronological order of surgery, with 40 patients in each group. The results were plotted on control charts to visualize outliers in each group.
The operation time was recorded from skin incision until closure. Postoperative morbidities were evaluated according to the Clavien–Dindo classification. 16 Intraoperative morbidities included injury of the bronchus, vessel injury, and conversion. Postoperative morbidities included fistula of the bronchus, persistent air leakage (>5 days), postoperative pneumonia, empyema, and postoperative pneumothorax.
Statistical analysis
Statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) version 24.0 software (SPSS, Inc., Chicago, IL). Non-normally distributed data are summarized as the median and interquartile range, normally distributed continuous data are summarized as the mean and standard deviation, and categorical data are summarized as frequencies and percentages. Analysis of variance and the unpaired Student's t-test were used for normally distributed continuous data, and the Wilcoxon rank sum test was used for non-normally distributed data. Frequency-dependent data were analyzed using Fisher's exact test.
The operating time was analyzed using the cumulative sum (CUSUM) method. This approach has been shown to be effective in learning curve analysis, especially in the field of surgery.12,17 In this study, the average total operation time was collected, and the CUSUM statistic of the first case was equal to the total operation time of the first case minus the average total operation time. The CUSUM statistic for the second and subsequent patients is equal to the difference between the total operative time and the mean summed CUSUM statistic for the previous case. This recursive process continues until the last patient has a CUSUM evaluation of zero. 18 In GraphPad Prism 9.0 for Mac (GraphPad software), the scatterplots of CUSUM and consecutive patients were plotted, and the curves were fitted according to nonlinear regression (least squares fitting method).
Then, we generated polynomials according to nonlinear regression. We computed the first derivative for each case on the two curves to determine the cutoff point, defined as the point at which the first derivative equals zero. Finally, different learning stages were identified according to these cutoff points.
Results
Baseline characteristics and general perioperative outcomes
The baseline characteristics are given in Table 1. No significant differences were observed in sex, height, weight, body mass index, pulmonary function, or comorbidities between the subgroups. The intraoperative outcomes are evaluated in Table 2. There were 245 lobectomies and 155 segmentectomies in this cohort. The mean operative time was 126.32 ± 46.62 minutes. Conversion was required for 3 patients (0.75%). Robot-assisted anatomical lung resections were performed for 365 patients with adenocarcinoma (91.25%), 33 patients with squamous cell carcinoma (8.25%), and 2 patients with other histologic types (0.5%), as given in Table 3. The mean tumor size was 15.64 ± 12.38 mm. The pathologic stages of lung cancer were IA1 in 164 cases (41%), IA2 in 143 patients (35.75%), IA3 in 22 patients (5.5%), IB in 21 patients (5.25%), IIA in 5 patients (1.25%), IIB in 17 patients (4.25%), IIIA in 25 patients (6.25%), and IIIB in 3 patients (0.75%).
Demographics of 400 Consecutive Patients Who Underwent Robot-Assisted Anatomic Lung Resection
BMI, body mass index; CHD, coronary heart diseases; DLCO, diffuse diffusing capacity for carbon monoxide; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; MVV, maximum ventilatory volume.
Intraoperative Outcomes of 400 Consecutive Patients Who Underwent Robot-Assisted Anatomic Lung Resection
Oncological Outcomes of 400 Consecutive Patients Who Underwent Robot-Assisted Anatomic Lung Resection
The postoperative results of the 400 consecutive patients are given in Table 4. The chest tube duration was 3.27 ± 1.57 days, and the postoperative hospital stay was 5.32 ± 1.73 days. There was no perioperative death or bronchopleural fistula. Postoperative morbidities occurred in 39 patients (9.75%), of whom 25 patients (6.25%) had prolonged air leakage (>5 days) (PAL), 2 (0.5%) had atelectasis, 1 (0.25%) had pneumonia, 1 (0.25%) had empyema, 1 (0.25%) had atrial tachycardia, 6 (1.5%) had atrial fibrillation, 2 (0.5%) had stroke, and 1 (0.25%) had wound infection.
Postoperative Outcomes of 400 Consecutive Patients Who Underwent Robot-Assisted Anatomic Lung Resection
Assessment of safety outcomes
Estimated blood loss, intraoperative hemorrhage (>500 mL), and perioperative morbidities were considered patient-safety outcomes. No significant differences were observed in the mean blood loss among the subgroups (P = .71). Intraoperative hemorrhage (>500 mL) occurred in 14 patients (3.5%), and there were no significant differences among the subgroups. The most frequent morbidity was PAL. The incidence of PAL significantly decreased after 120 patients (11.7% versus 3.9%; P = .003; Fig. 1). The highest incidence of PAL occurred in subgroups 2 (patients 41–80) and 3 (patients 81–120). The incidence of postoperative complications was significantly improved after 120 patients (15.83% versus 7.14%, P = .007).
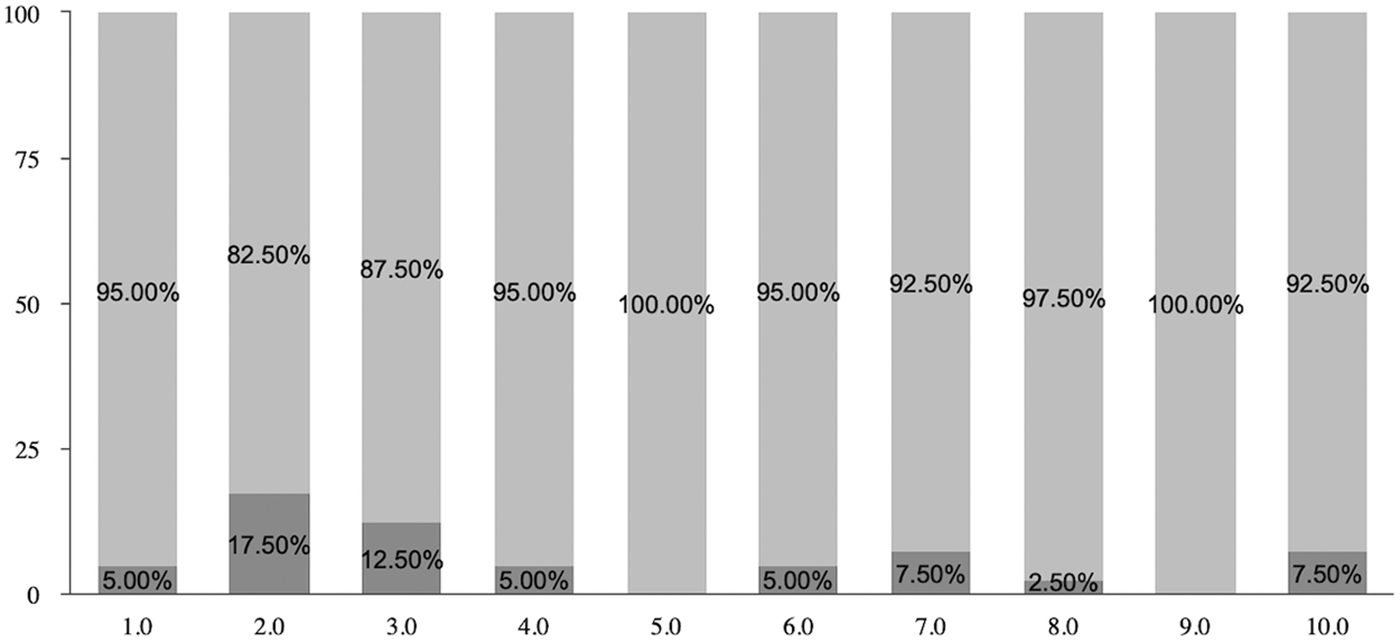
Safety outcomes for 400 consecutive robot-assisted lung resections. Incidence of prolonged air leakage.
Assessment of efficiency outcomes
The outcomes, including mean operative time, rate of conversion, chest tube duration, and postoperative hospital stay, reflected efficiency. Sustained improvement in mean operative time was shown across 400 consecutive patients (P = 0; Fig. 2a). CUSUM graphs were constructed to confirm the improvement in operative time (Fig. 2b). According to the CUSUM analysis of operative time, the learning curves of lobectomy, segmentectomy, and total lung resection were fit to a sixth-order polynomial (R 2 = 0.9276, 0.9789, and 0.9649, respectively). In patients involving lobectomies, the learning curve was divided into three phases: an initial phase (patients 1–14, phase 1), a transition phase (patients 15–93, phase 2), and a proficient phase (patients 94 and those after, phase 3). In segmentectomy patients, the learning curve was as follows: an initial phase (patients 1–9, phase 1), a transition phase (patients 10–99, phase 2), and a proficient phase (patient 100 and those after, phase 3).
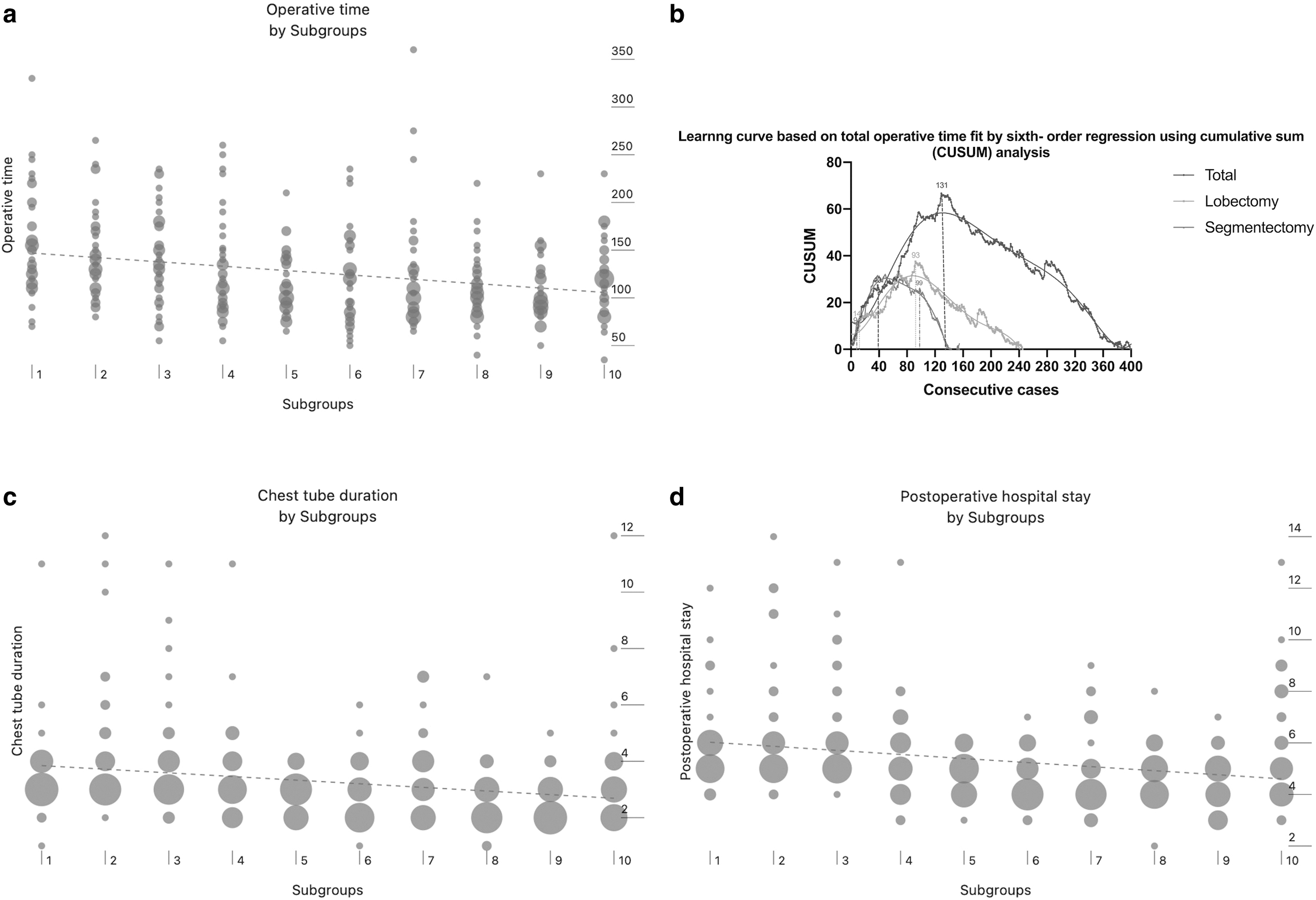
Efficiency outcomes for 400 consecutive robot-assisted lung resections.
For total lung resections, the initial phase comprised patients 1–40, the transition phase comprised patients 41–131, and the proficient phase comprised patient 132 and those after. There were 3 patients with conversion among these 400 patients, 1 each in subgroup 2 (41–80), subgroup 5 (161–200), and subgroup 10 (361–400). The reasons for conversion were intraoperative hemorrhage (n = 2) and calcified lymph nodes in the hilum (n = 1). The length of postoperative hospital stay and chest tube duration also showed significant decreases after 120 patients (3.92 ± 1.91 versus 2.99 ± 1.31, P = .000; 6.22 ± 2.02 versus 4.93 ± 1.44, P = .00, respectively). Figure 2c, d shows continuous improvement trends throughout the 400 consecutive patients.
Assessment of oncologic outcomes
In this cohort, R0 resections were achieved in all 400 consecutive patients. The mean number of lymph nodes was 6.54 ± 1.27, and the mean number of lymph node stations was 6.54 ± 1.27. Subgroups 2 (patients 41–80) and 3 (patients 81–120) showed significant improvements in dissected stations of lymph nodes among the subgroups (P = .01) (Table 3).
Discussion
The use of robotics in thoracic surgery has been shown to be safe and to achieve equivalent oncological outcomes.19–21 Compared with other minimally invasive surgeries, the robot-assisted system provides three-dimensional optics, flexible maneuverability, and improved dexterity. Melfi et al. first reported robot-assisted lobectomy in 2002, and Anderson reported the first robot-assisted segmentectomy in 2007.5,6 Since then, the application of robotic surgery has been gradually accepted across the world.
Several series have demonstrated the safety and feasibility of robotic thoracic surgery; however, adoption of this procedure by experienced surgeons remains a challenge because many of them are accustomed to performing VATS or open surgery. 7 This study reports that the learning curve required to effectively perform lung resections ranges from 20 to 40 patients, within the previously reported range of 14–60 patients. 7 In this study, the learning curve was similar to that in previous studies. The operative time was improved after 40 patients and showed significant improvement after 120 patients. The operative time gradually declined during the consecutive 400 patients. This finding may suggest that robotic platforms could allow surgeons to constantly improve their technique and continually reduce operating time, consistent with previous studies. 22
However, the operating time itself is not enough to reflect the learning process of robot-assisted lung resections. Competence is the basis on which surgeons are allowed to perform operations independently. Growing competence in complicated surgery entails performing enough procedures to demonstrate consistent safety and efficacy. 23 The safety of surgery was evaluated by intraoperative blood loss, intraoperative hemorrhage (>500 mL), and perioperative morbidities. The mean blood loss was not significantly different between the subgroups. This result may indicate that robot-assisted anatomical lung resection is safe for surgeons with VATS experience. Intraoperative hemorrhage (>500 mL) occurred in 14 (3.5%) patients, which were distributed among the subgroups 2, 3, 4, 5, 7, 8, 9, and 10. Conversion was observed in 3 patients, which were distributed among the subgroups 2, 5, and 10. In intraoperative hemorrhage patients, the mean tumor size was 37.92 ± 31.23 mm.
The pathologic stages of lung cancer were IIIB in 1 patient, 3A in 5 patients, IIB in 3 patients, and IA in 4 patients. Most patients showed lymph node fibrosis and calcification on CT scans. These hemorrhage and conversion numbers probably reflect the increasing experience of the surgeon and the confidence to perform more difficult operations. The total postoperative morbidity was 9.75%. Subgroups 2 and 3 accounted for the highest incidence of complications. The incidence of intraoperative complications gradually decreases as the learning curve progresses.24–26 PAL was the most common morbidity in this cohort. A case series reported the risk factors for PAL, including emphysema, low forced expiratory volume in 1 second (FEV1), obesity, male sex, pleural adhesions, and upper lobectomy or bilobectomy. 27 Surgeon experience was another factor associated with prolonged air leak time after robot-assisted lung resection.
Lowell and colleagues reported the inflection point at which PAL rates were significantly reduced after the 50th patient. 28 Experienced surgeons with meticulous surgical techniques are vital in reducing PAL incidence. 29 Competence is indicated by a physician's ability to perform a surgery safely and effectively.
The primary indicators to evaluate surgical efficiency were chest tube duration and postoperative hospital stay in this study. We found that the chest tube duration and length of postoperative hospital stay improved significantly after 120 patients. Oncological efficiency includes the rate of R0 resection, mean numbers of harvested lymph nodes, and stations of lymph nodes. In this cohort, the rate of R0 resection was 100%, and there were no differences in the numbers of dissected lymph nodes between subgroups. The oncological efficiency is favorable for experienced surgeons. There were more mean dissected stations of lymph nodes in subgroup 4 than in the other subgroups. This outcome may result from the high proportion of lobectomy in this subgroup. Compared with VATS, RATS may harvest more lymph nodes, especially in the mediastinum regions. 30 Robotic technology offers advantages for lymph node dissection, including three-dimensional surgical views, magnification, and dexterity. The number of lymph nodes did not tend to improve in this cohort. The reason for this outcome is that the surgeon was experienced and skilled in the resection of lymph nodes.
Study strengths and limitations
First, this analysis was a retrospective study in which the surgeries were performed by a single surgical team. The retrospective nature may increase the risk of selection bias. However, this also increases the homogeneity of the data while avoiding being confounded by other surgeons' experience. Second, this study included 245 lobectomies and 155 segmentectomies. The learning curves for lobectomies and segmentectomies may be different. In clinical practice, lobectomy and segmentectomy cannot be completely isolated. Therefore, comprehensive analysis of the initial 400 consecutive anatomical resections may reflect the reality of new implementations in robot-assisted lung surgery. Third, middle-term and long-term oncological results are lacking. The assessment of postoperative oncological efficiency requires further data to update the outcomes. Finally, the surgeon in this study was proficient in minimally invasive thoracoscopic surgery. The learning curve for different surgeons may vary depending on their previous experience and inherent skills.
Conclusions
During the performance of robot-assisted anatomical lung resection, we performed a comprehensive assessment of surgery quality and perioperative outcomes. In conclusion, technical proficiency with favorable perioperative outcomes was achieved after 120–130 patients.
Footnotes
Authors' Contributions
X.H.: Methodology, software, data curation, writing—original draft preparation. Z.L.: Writing—reviewing and editing.
Availability of Data and Materials
The datasets used and/or analyzed during this study are available from the corresponding author upon reasonable request.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.