
Abstract
Background:
Accurate preoperative workup is crucial to identify patients with intrahepatic cholangiocarcinoma (IHC) who would have truly benefit from liver resection, avoiding it in patients with advanced disease or distant metastases. Staging laparoscopy (SL) may prevent unnecessary laparotomies in those patients with otherwise resectable disease, but evidence of its efficacy is scarce and inconclusive. We aimed to aggregate the available evidence dealing with this specific field of research to produce a snapshot of the current knowledge systematically reviewing the inherent literature.
Methods:
PubMed/Medline, EMBASE, and Web of Sciences electronic databases were queried through December 2022. Inclusion criteria considered all articles reporting data about the role of SL for patients with a diagnosis of IHC. The main outcomes were as follows: overall yield and sensitivity of SL.
Results:
A total of 5 studies including 119 patients met the inclusion criteria and were included in the analysis. Overall, the yield of SL was 19.6% (11.4%–36%), and the sensitivity was 65.2% (55%–71%).
Conclusions:
The role of SL for patients with a preoperative diagnosis of IHC remains unclear. The lack of criteria and indications to perform SL for IHC raises the need for international consensus on this specific field of research.
Introduction
Intrahepatic Cholangiocarcinoma (IHC) is a primary liver cancer that arises in the intrahepatic bile ducts and represents the second most common hepatic tumor after the hepatocellular carcinoma making up 10% to 15% of all primary liver malignancies.1–3 Unfortunately, diagnoses are often incidental events that cause the lack of specific symptoms resulting in the clinical presentation of the disease in a locally advanced or metastatic stage. Surgical resection is the only chance for a radical cure and is currently the standard of care for treatment. 4 An accurate preoperative workup is crucial to identify patients who would have truly benefit from liver resection, avoiding it in patients with advanced disease or distant metastases. Despite technological advances in preoperative imaging modalities used to assess patients before surgery, up to 70% of patients undergo an avoidable nontherapeutic laparotomy.5–8
Reasons for unresectability in these patients are liver, nodal, or peritoneal metastases or locally advanced disease.9,10 Staging laparoscopy (SL) may prevent unnecessary laparotomies in patients with otherwise resectable IHC, but the evidence is scarce and inconclusive. After about 20 years since the earliest reports on this topic, there are no criteria or any consensus about the indications to perform SL in patients with a preoperative imaging-guided diagnosis of IHC yet. The aim of the present study was to aggregate the available evidence dealing with the role of SL in patients with IHC to produce a snapshot of the current literature and to develop the first systematic review on this topic.
Materials and Methods
The PRISMA Statement checklist for reporting systematic reviews and meta-analysis 11 was used as a guide to aggregate scientific articles dealing with the role of SL in patients affected by IHC. Data for analysis were retrieved from the included studies following a pre-established pattern. Two authors (D.C. and A.S.) performed an independent and comprehensive literature search up to December 2022 through the PubMed/Medline, EMBASE, and Web of Sciences (WOS) electronic databases 12 with a combination of the following keywords and free text: “staging laparoscopy” OR “diagnostic laparoscopy” AND “cholangiocarcinoma” OR “cholangiocellular carcinoma” OR “biliary cancer” OR “primary liver cancer.” Titles and abstracts were selected, and the articles were considered eligible if the following criteria were met: (1) English language; (2) articles considering SL for cholangiocarcinoma; and (3) adult patients with preoperative imaging diagnosis of IHC.
Articles dealing with patients affected by distal or hilar cholangiocarcinoma or gallbladder cancer were excluded from the analysis as for case reports or congress proceedings. The references of the retrieved articles were hand screened to find further includible articles. The Population, Intervention, Comparator, Outcome, and Study design (PICOS) criteria are shown in Table 1.
Population, Intervention, Comparison, Outcomes, and Study Design
SL, staging laparoscopy.
From each included study, the following data were retrieved when available: population number, age, preoperative investigations such as computed tomography (CT), magnetic resonance imaging (MRI), positron emission tomography (PET) scans, and eventual biopsy, indications to SL were appraised too. With regard to the main outcomes data, the yield and sensitivity of SL were thus analyzed. As in previous reports, the yield of SL was defined as the proportion of laparotomies avoided in patients with high-quality preoperative imaging diagnosis, calculated by dividing the number of avoided laparotomies or the number of advanced diseases identified by laparoscopy to the total number of laparoscopic procedures.
The sensitivity was defined as the probability of detecting unresectable disease by laparoscopy calculated by dividing the number of unresectable patients at SL to the total number of patients with unresectable cancers. The reasons for unresectability and eventual intraoperative or postoperative complications were also recorded. Differences in opinion were discussed with the input of a third author (G.L.G.). Discrepancies between the authors' retrievements were solved by consensus among all authors.
Quality assessment of the included studies was assessed by using the guide of the Risk Of Bias In Non-randomised Studies–of Interventions (ROBINS-I) tool (Table 2). 13
Methodological Quality Assessment of the Included Studies with the Risk Of Bias In Non-randomised Studies–of Interventions (ROBINS-I) Tool
NA, not available.
Results
Studies selection
Through the initial electronic search, a total of 16,860 records were retrieved. The titles and abstracts were examined, duplicates were excluded, and full texts of potentially eligible articles were appraised. Finally, 5 studies including 119 patients met the inclusion criteria and were considered for analysis.4,14–17 The search strategy is depicted in Figure 1.
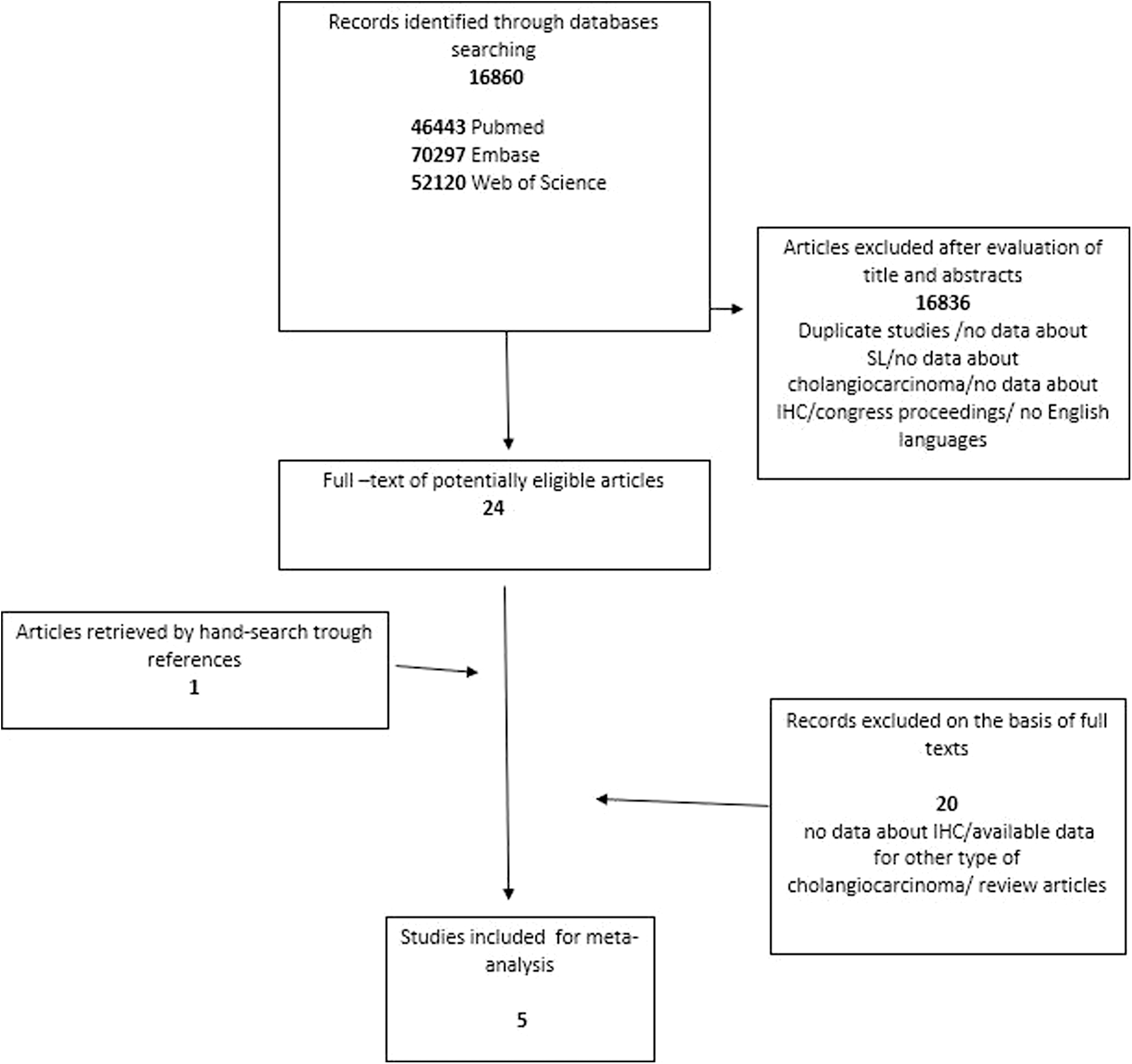
Search strategy. IHC, intrahepatic cholangiocarcinoma; SL, staging laparoscopy.
Characteristics of the studies
Three of the included studies were from Europe,14–16 and two were from the United States.4,17 The time frame in which the studies have been published was about 20 years from 2000 and 2020. All the studies were retrospective analyses of single-center series, and no randomized controlled trial (RCT) has been found. All articles report on SL in patients with cholangiocellular cancer, but only two articles4,14 are specific for IHC and one article 16 explored also the role of laparoscopic ultrasound in SL for proximally biliary cancer. The median age of patients was 61 years, but detailed data of subgroups of IHC patients were reported only in one study. 14
Circumstantial data on preoperative imaging are reported in all articles, but almost for the entire series considered, specific data about patients who underwent a CT scan alone are derived from three articles14–16 (data from 90 patients), showing that it was performed for 100% of patients considered; one study 14 reported that MRI alone was not performed, both CT and MRI were performed for 66% of population, and PET for 29% (data from 35 patients).
The indications for performing SL are explained in detail in two studies14,16 (data from 79 patients) showing 27% to exclude metastatic disease, 62% for large-size tumors, 2% to assess the quality of remnant liver after portal vein embolization, and 9% to obtain eventual pathological confirmation of preoperative diagnosis.
Main outcomes
Four studies did report data concerning the yield and sensitivity of SL for specific subgroups of patients with the diagnosis of IHC,4,14–16 and one study reported the yield of the entire series analyzed. 17 Overall, the yield of SL was 19.6% ranging between 11.4% and 36%, and the sensitivity was 65.2% ranging between 55% and 71%, including in the analysis only study containing specific data (data from 112 patients). Data concerning the reasons for the judgment of unresectable disease are reported in four studies,4,14–16 but only in two studies4,14 are detailed and specific for IHC patients. Peritoneal metastases represented 14% of the reasons for unresectability judgments, the same percentage was for liver metastases, 3% was for severe cirrhotic liver, 3% for distant lymph node metastases, and finally, 1% for locally advanced tumors.
Complications
Two studies14,15 reported data about intraoperative or postoperative complications (data from 46 patients): one (2%) serosal tear of the small bowel managed by simple suturing and one aspiration pneumonia (2%). Table 3 summarizes the results.
Summary of the Results
Data of the entire series.
CT, computed tomography; FNH, focal nodular hyperplasia; liver met, liver metastases; loc adv, locally advanced disease; lymph met, distant lymph node metastases; met, exclusion of metastatic disease; MRI, magnetic resonance imaging; NA, not available; path conf, pathological confirmation; PET, positron emission tomography; perit met, peritoneal metastases; rem liv, assessment of remnant liver after portal vein embolization; sev cirr, severe cirrhosis; SL, staging laparoscopy.
Discussion
The role of SL for patients with IHC is a matter of debate that has not yet been concluded and clarified. In addition, there is neither a consensus nor criteria for indications to perform it as a preoperative workup to detect potentially unresectable diseases. This is demonstrated by the fact that, although about 20 years have passed since the publication of the first works on this topic, the relative literature is scarce both in quantity and in quality and completeness of the data of each single study. Probably because the disease is very rare, its presentation is unlikely to be at a potentially curable stage, and therefore, the data obtained from the literature derive from small series of patients and from retrospective studies of single centers. The aim of our study was to aggregate all available literature in the field of SL for patients with IHC. To the best of our knowledge, this represents the first systematic review of this specific topic.
The most important finding derived from this research is probably the scarcity of literature concerning the role of SL in the preoperative workup of patients with preoperative imaging diagnosis of IHC.
As specific data for patients with IHC were only partially available in the preoperative imaging investigations, it was not possible to ascertain the true number of patients who underwent CT only, MRI only, or both, or PET. Mejia and Pasko in their work recommended dedicated liver multiphasic CT or MRI 18 as necessary workup investigations in suspected IHC and PET or mass biopsy within the examinations to consider in the second line. To date, both CT and MRI are considered investigations with comparable sensitivity in identifying secondary disease localization. 19 In the recently released European Association for the Study of the Liver and the International Liver Cancer Association (EASL-ILCA) Clinical Practice Guidelines on the management of IHC, MRI and CT are recommended as staging imaging tests. The role of contrast-enhanced ultrasound is still controversial, and the usefulness of CT-PET is of relevance for lymph node metastasis identification. 20 In this scenario, an SL before surgery could be beneficial for patients who have a suspicion of metastatic disease that was not evident during their preoperative imaging workup.
The lack of precise indications and criteria for performing a diagnostic laparoscopy in this type of patient is demonstrated by the fact that the reasons for SL were only clearly illustrated in two studies,14,16 the predominant reason being the tumor size, also re-evaluated in the most recent and just updated guidelines on staging, 21 followed by the identification of metastatic disease, the histological confirmation of the diagnosis, and assessment of the quality of the remnant liver after portal vein embolization.
Regarding the main objective of the study, there was considerable variability between all studies with an average yield and sensitivity value of 19.6% and 65.2%, respectively, values that do not allow to recommend it on a routine basis. Russolillo et al. 16 investigated how to increase the yield and accuracy of SL, adding to it the laparoscopic ultrasound by augmenting the overall yield from 11.4% to 18.2% and overall accuracy from 62.5% to 100%; this concept has been expressed already in previous reports about the laparoscopic staging of biliary and other intra-abdominal cancers.22–24
Unfortunately, there are no comparative studies on this for IHC patients. In regard to the causes of inoperability, the main reason was found to be peritoneal carcinomatosis, followed by liver metastases, lymph node metastases on a par with severe cirrhosis, and finally, locally advanced neoplasms, also for this outcome, a variability of data reporting existed, specific data only from two studies.4,14 Complications of SL represent a negligible percentage as demonstrated by the fact that from this research, only one complication can be strictly linked to the surgical procedure, a small bowel serosal tear. Chang et al. also reported a low risk of complications after SL illustrating potential risks of bleeding, infection, and bile leak, particularly if a liver biopsy is performed and those associated with surgical laparoscopy in general and those associated with anesthesia. 22
Anyway, in this challenging management, a multidisciplinary approach is needed in the decision-making on any type of treatment, especially for those patients potentially resectable.
Some limitations of the study must be acknowledged. First, the scarcity of the limited number of studies and patients does not allow us to generalize the results obtained to the general population; furthermore, the retrospective nature of the studies as well as the lack of RCTs preclude us to define ours as “high” level evidence. Second, only two studies are specific to IHC, some data refer to the entire series of patients considered in individual studies sometimes affected by other types of cholangiocarcinoma, and therefore, not all results can be attributed specifically to IHC patients. Finally, the publication time interval between the studies considered of about 20 years brings with it the weight of the differences and evolutions both in the preoperative imaging investigations and in the surgical techniques strictly linked to SL performance.
Conclusions
The role of SL for patients with a preoperative diagnosis of IHC remains unclear. The scarcity of the inherent literature is evident and precludes the possibility to reach clear conclusions but opens the way to further investigations. Laparoscopic ultrasound could augment the yield and sensitivity of SL in those patients affected by doubtful resectable diseases. The lack of criteria and indications to perform SL as an important point in the preoperative workup for IHC may raise the need for international consensus on this specific field of research.
Footnotes
Authors' Contributions
Conceptualization: D.C. and G.L.G. Methodology: D.C. and A.S. Formal analysis: D.C. and A.S. Data curation: D.C. Writing—original draft preparation: D.C. and G.L.G. Writing—review and editing: D.C., A.S., G.L.G., and A.P. Critical revision of the article: A.P. All authors have read and agreed to the published version of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.