
Abstract
Background:
Early postoperative pain is a significant problem in bariatric and metabolic surgery. Our study aimed to investigate the potential role of intraperitoneal bupivacaine hydrochloride in pain management in the early postoperative period after bariatric and metabolic surgery.
Methods:
This double-blind, prospective, randomized, controlled study included 68 individuals who underwent bariatric and metabolic surgery at the Department of Surgery, Istanbul Aydin University Hospital. The study group received 20 mL of 0.5% bupivacaine hydrochloride intraperitoneally at the operative site, and the control group received 20 mL of normal saline. Visual analog scale (VAS) scores of each patient were recorded at 2nd, 4th, and 6th hours postoperatively.
Results:
Our study found significant differences in VAS scores of patients between study group and control group at 2nd, 4th, and 6th hours postoperatively. Significant differences were found between male and female patients in the control group at 2nd, 4th, and 6th hours postoperatively. Interestingly, no significant difference was found between female patients in the study group and control group at 2nd, 4th, and 6th hours postoperatively.
Conclusions:
Our study suggests that intraperitoneal administration of bupivacaine hydrochloride is effective in reducing early postoperative pain in male patients. However, no significant difference was found between the study group and the control group in female patients. Our results indicate that there may be a gender-related difference in the response to bupivacaine administration. Further research is needed to confirm these findings and determine the optimal dosing and administration of local anesthetics for postoperative pain management.
Introduction
Morbid obesity is a health concern that affects millions of people around the world. The prevalence of morbid obesity has gradually increased over the last 25 years due to dietary and lifestyle changes. 1 Consequently, significant advances have been made in the treatment of morbid obesity. 2
Bariatric surgery is a highly effective treatment that promotes sustainable weight loss and health and alleviates the symptoms of morbid obesity. 3 Bariatric surgery has gained widespread acceptance and helped reduce the burden of morbid obesity on health care systems worldwide. Various studies have been conducted aiming to minimize the risk of morbidity and mortality associated with this procedure. 4
Currently, ongoing research in this field revolves around one of the main issues after bariatric surgery: the management of postoperative pain. Effectively managing and reducing the severity of postoperative pain allows patients to mobilize earlier and perform the required breathing exercises regularly, reducing the length of hospital stay and associated costs. 5 Consequently, the perioperative and postoperative administration of opioid analgesics, nonsteroidal anti-inflammatory drugs (NSAIDs), and steroids have become routine despite their associated side effects. 6 Several studies investigating the effect of intraperitoneal local anesthetic administration after laparoscopic surgery on pain have been conducted. 6 This anesthetic strategy provides adequate pain management and avoids the side effects of opioids and NSAIDs.
Bupivacaine hydrochloride is a local anesthetic that is broken down by microsomal enzymes, more stable and less allergic than ester group local anesthetics. Bupivacaine hydrochloride inhibits the permeability of sodium ions along the nerve wall and inhibits the nerve impulses. 7
Extensive research studies and comprehensive reviews have highlighted the role of gender as an important variable in the modulation, interpretation, and perception of pain sensations. Hormonal variances, neurological elements, sociocultural aspects, and psychosocial factors contribute to the differences in pain sensations. A thorough understanding of the gender role in differential pain perception is critical for developing optimal pain management strategies. 8
In this study, we aimed to investigate the potential role of intraperitoneal bupivacaine hydrochloride administration for pain management in patients in the early postoperative period after bariatric and metabolic surgery.
Materials and Methods
Patients
This double-blind, prospective, randomized, controlled study included 68 individuals who underwent laparoscopic sleeve gastrectomy to treat a body mass index (BMI) >32 kg/m2 or obesity-related comorbidities between November 2019 and January 2020 at the Istanbul Aydin University General Surgery Clinic, Istanbul, Turkey. The individuals were randomly assigned to the study (n = 34) and control (n = 34) groups by the anesthesia technicians who was involved in the procedure. The responsibility of this technician was to prepare and hand over the drugs to the surgical nurse for administration. The teams of anesthesiologists and surgeons involved in the surgery were blinded to the selection process. The exclusion criteria included the patients who had a history of reacting to local anesthetics, were undergoing revision surgery, or had a history of previous major abdominal surgery.
Ethics statement
Ethics Committee approval (no. 2019/183) was obtained from the Istanbul Aydin University Ethics Committee on November 11, 2019. All procedures complied with the Institutional and National Research Committee's ethical standards and the 1964 Helsinki declaration and its later amendments. Written informed consent was obtained from each patient before surgery.
Surgical procedure
All the patients underwent preoperative anesthetic, pulmonological, and psychiatric consultations.
All 68 patients underwent laparoscopic sleeve gastrectomy, and 3 underwent additional cholecystectomy due to coexisting cholelithiasis. Preoperatively, 3 mg intravenous midazolam, and during induction, 200 mg of 1% propofol, 0.5 mg/kg of rocuronium, 1 mg/kg of fentanyl, 10 mg of metoclopramide, 20 mg of hyoscine-n-butyl bromide, 1 mg/kg of methylprednisolone, 2 g of paracetamol, 100 mg of tramadol, and 50 mg of ranitidine were administered. Following induction, the patients were positioned in the reverse Trendelenburg position with their legs abducted. The surgeon was positioned between the patient's legs, the assistant surgeon on the patient's right, and the scrub nurse on the left. An 11 mm camera trocar was inserted to the left of the midline, ∼10–12 cm inferior to the lower end of the sternum, without creating a pneumoperitoneum, and CO2 insufflation was performed to an intraabdominal pressure of 15–16 mmHg. Using Petit's triangle as a landmark, a camera-guided transversus abdominis plane (TAP) block was performed on both sides of the patient's abdomen. 9
The TAP block was performed by injecting 20 mL of 0.5% bupivacaine hydrochloride (100 mg) diluted in 20 mL of normal saline into each side of the patient's abdomen. One 5 mm and one 15 mm trocar were inserted into the right side of the abdomen and one 5 mm trocar into the left side.
The greater curve of the stomach was dissected using the LigaSure™ (Medtronic, Minneapolis, MN). The stomach was freed from the pylorus to the hiatus, and a 36 F orogastric bougie was placed. Next, the sleeve gastrectomy procedure was initiated 3 cm above the pylorus using Tri-Staple™ (Medtronic). The patients were given 20 mg of tenoxicam and 8 mg of ondansetron during resection. At the end of the surgery, 20 mL of 0.5% bupivacaine hydrochloride (100 mg) was administered, intraperitoneally, to the operative site (hiatal region) in the study group. The control group received 20 mL of normal saline at the same site. A 10 mm soft silicone drain was placed next to the remnant stomach.
The drain was clamped for 30 minutes to prevent leakage of the local anesthetic. The patients were postoperatively administered 0.5 mg/kg of pethidine hydrochloride and transferred from the recovery room to their rooms after being assessed for adequate analgesia. Pain was assessed at 2, 4, and 6 hours postoperatively using the visual analog scale (VAS), ranging from 0 (no pain at all) to 10 (the worst pain). 10 In accordance with routine practice, the patients were administered 20 mg of tenoxicam twice a day, 50 mg of tramadol four times a day, and 1 g of paracetamol three times a day within the first 12 hours after surgery, and on postoperative day 1. Additional tramadol was administered when necessary. All patients had their drains removed on postoperative day 1. At discharge, the patients were prescribed only oral paracetamol syrup for analgesia, which was discontinued after the follow-up appointment on postoperative day 7.
Statistical analyses
The normal distribution of the continuous variables was determined using the Shapiro–Wilk test. Comparison of variances was analyzed using F-test. For normally distributed variables, the unpaired t-test was used to compare the values of two independent groups. For non-normally-distributed variables, the Mann–Whitney U test was used to compare the values of two independent groups. A P value <.05 was considered statistically significant. All statistical analyses were performed using GraphPad Prism version 9.5.1 (GraphPad Software).
Results
A total of 37 women and 31 men were enrolled in the study. The mean age was 35.39 years, and the mean BMI was 42.27 kg/m2. VAS score of all patients were recorded at the 2nd, 4th, and 6th hours (Table 1).
Characteristics of the Patients with Details
BMI, body mass index; SD, standard deviation.
In Figure 1, significant differences of VAS scores of the patients were found between the study group (n = 34) and the control group (n = 34) at the 2nd, 4th, and 6th hours (P < .05, P < .05, and P < .01, respectively).
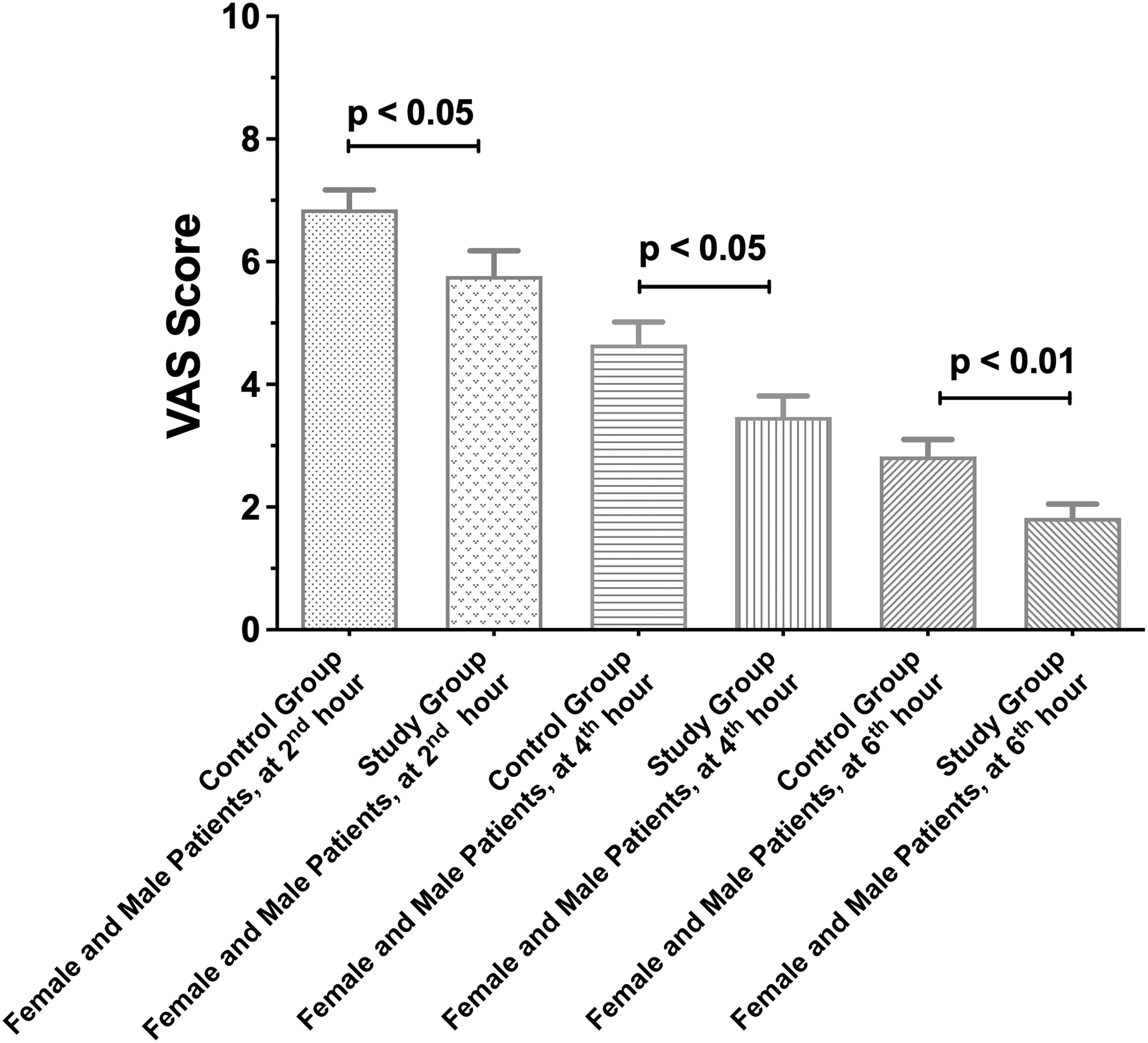
Comparison of VAS scores of study group and control group. VAS, visual analog scale.
In Figure 2, significant differences of VAS scores of male patients were found between the study group (n = 14) and the control group (n = 17) at the 2nd, 4th, and 6th hours (P < .05, P < .01, and P < .01, respectively).
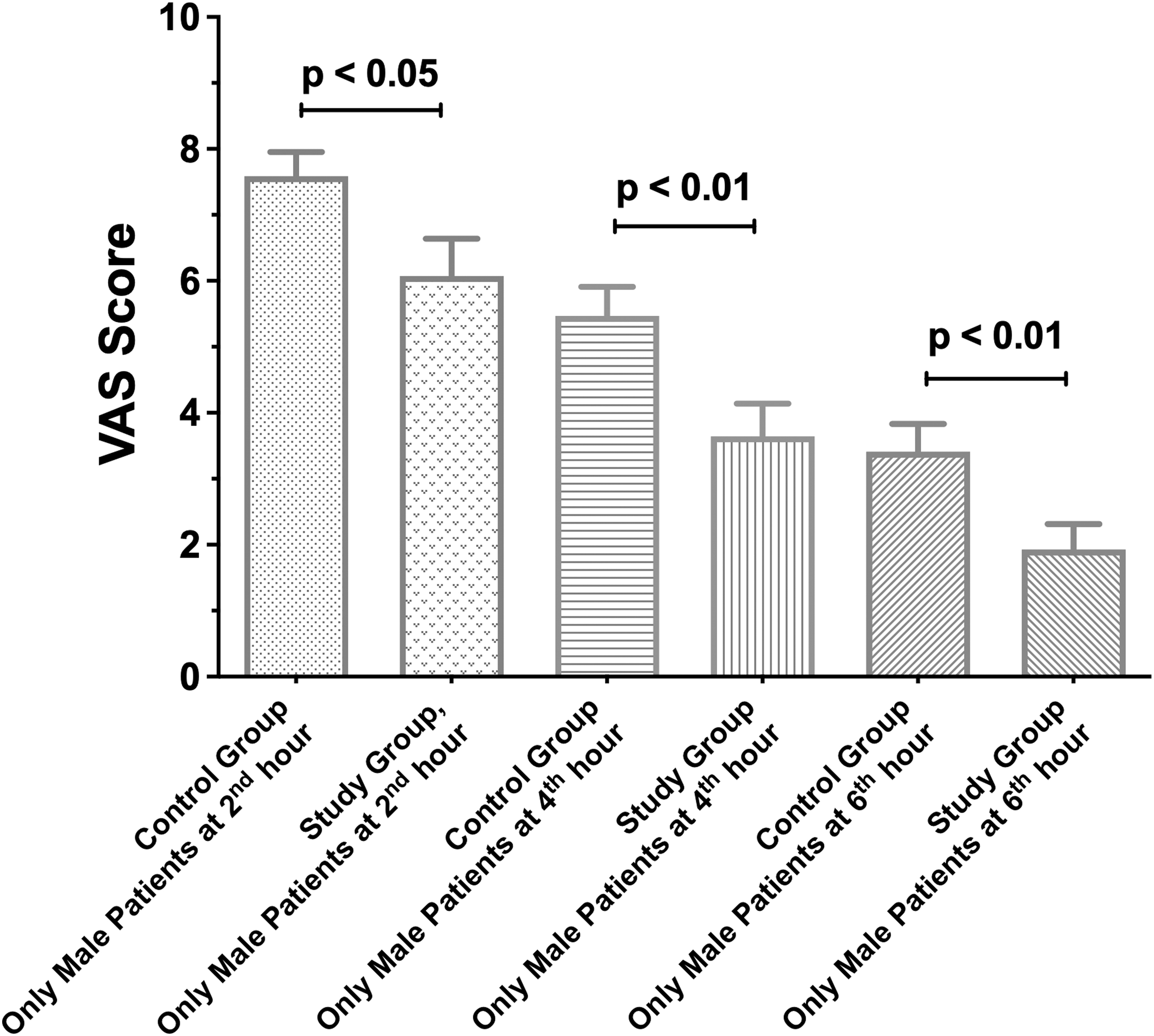
Comparison of VAS scores of study group and control group in only male patients. VAS, visual analog scale.
In Figure 3, no significant differences of VAS scores of female patients were found between the study group (n = 20) and the control group (n = 17) at the 2nd, 4th, and 6th hours.
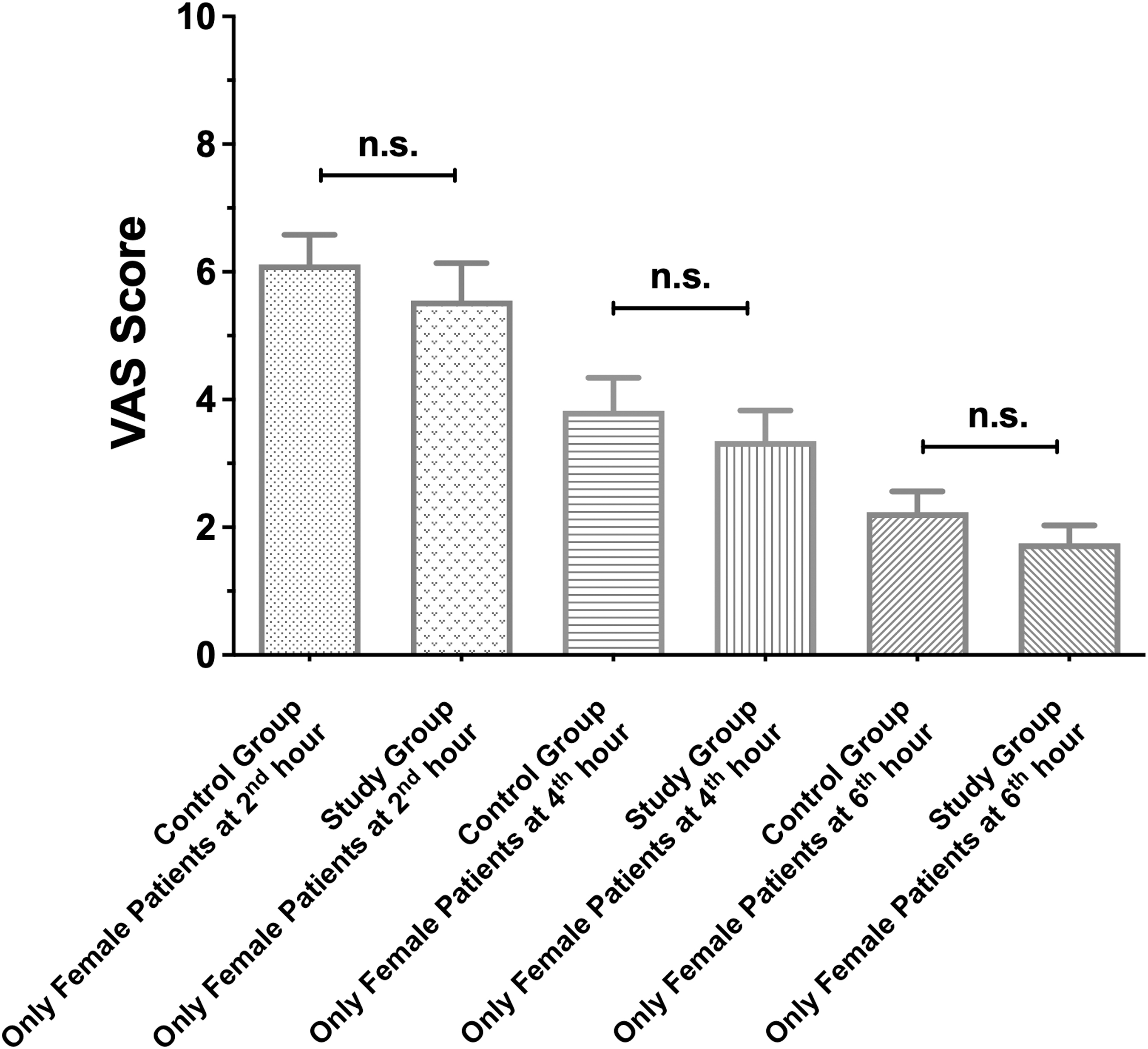
Comparison of VAS scores of study group and control group in only female patients. VAS, visual analog scale.
In Figure 4, VAS scores of the patients were evaluated, significant differences of VAS were found between female patients in control group (n = 17) and male patients in control group (n = 17) at the 2nd, 4th, and 6th hours (P < .05, P < .05, and P < .05, respectively).
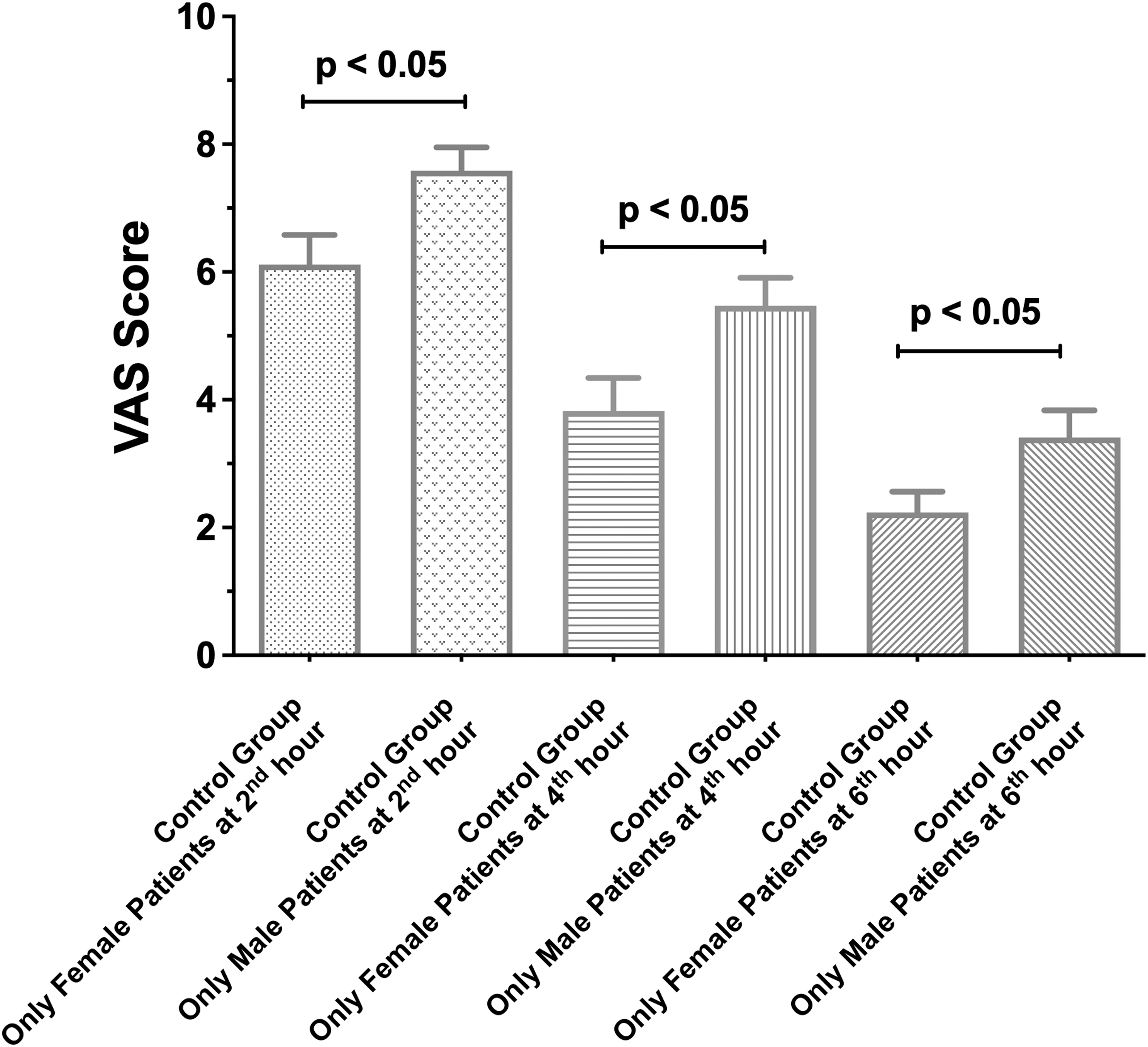
Comparison of VAS scores of male patients in control group and female patients in control group. VAS, visual analog scale.
In Figure 5, VAS scores of the patients were evaluated, no significant differences of VAS were found between female patients in study group (n = 14) and male patients in study group (n = 20) at the 2nd, 4th, and 6th hours.
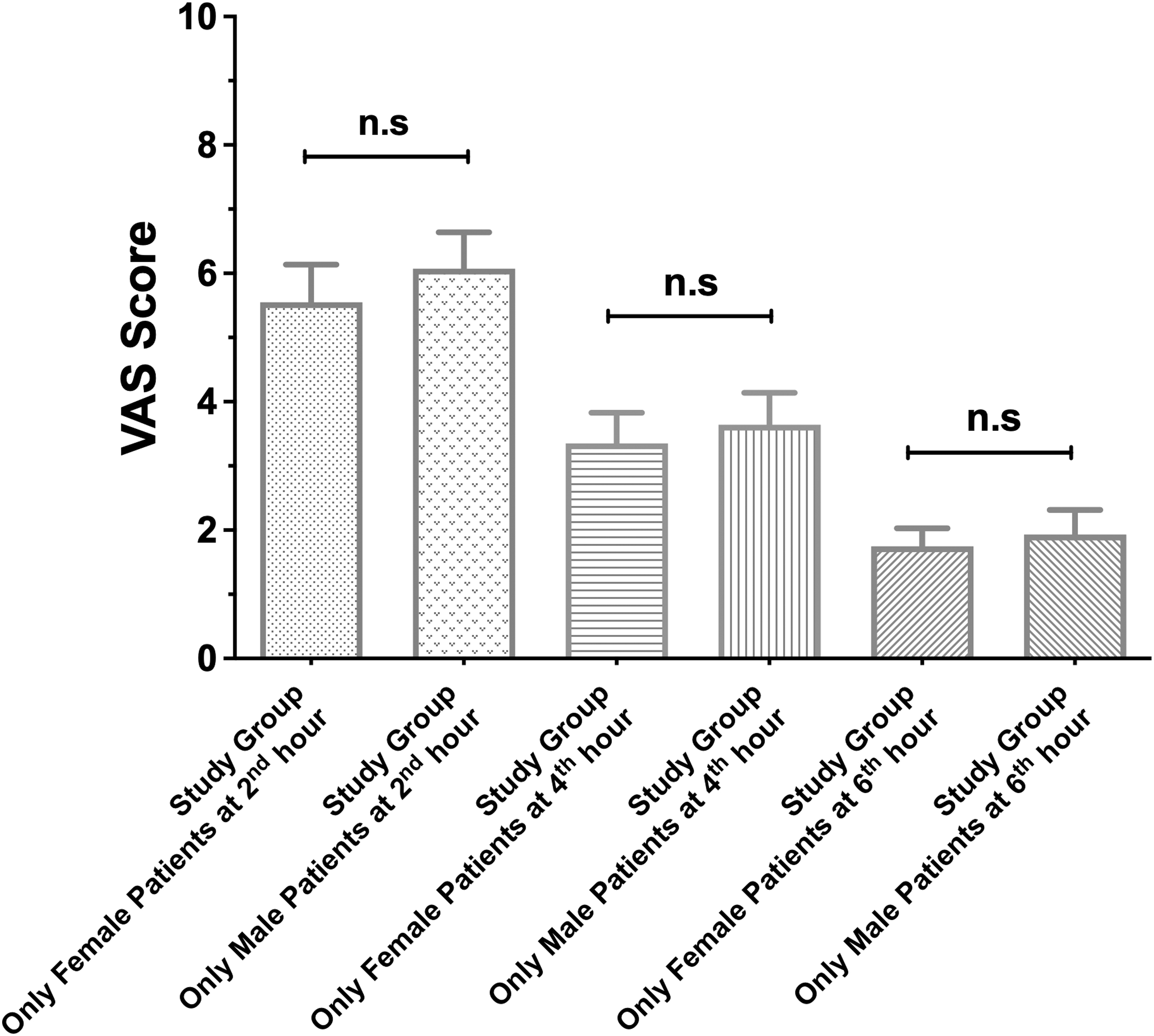
Comparison of VAS scores of male patients in control group and female patients in study group. VAS, visual analog scale.
Overall, in Figure 2–5, male patients in the study group had significantly lower VAS scores compared with the male patients in the control group at the 2nd, 4th, and 6th hours. Interestingly, there were no significant differences in VAS score of female patients between the study group and control group. These findings suggest that bupivacaine may be more effective in managing postoperative pain in male patients undergoing bariatric and metabolic surgery.
None of the patients experienced postoperative complications, and all the patients were discharged on postoperative day 3. None of the patients complained of pain at their follow-up visit on postoperative day 7.
Discussion
When there is tissue damage or an irritating effect in a part of the body, it is transmitted to the central nervous system to the brain with specialized nerve fibers that are called nociceptors. The brain analyzes these signals and perceives the pain. The pain is a perception in nociception. Perception of pain is not just a result of physical sensations and can be influenced by psychological factors, gender, and sociocultural conditions. 8
Abdominal pain is commonly encountered after laparoscopic surgery. It is hypothesized that the pain originates from residual intraperitoneal carbon dioxide irritating the visceral peritoneum and diaphragm and increasing the intraabdominal pressure. 11 Alleviating postoperative pain following bariatric and metabolic surgery reduces the risk of complications, shortens the length of hospital stay, early postoperative mobilization, and provides a quick return to their daily lives. 11 Although there is no consensus on the optimal strategy for postoperative pain management, various techniques have been recommended, including intraperitoneal local anesthesia, oral or parenteral narcotic administration, TAP block, and local anesthesia at the trocar site.12–14
Several studies have investigated the effect of intraperitoneal local anesthetics on postoperative pain.12–14 In a study by Omar and Abualsel involving 100 patients (n = 33 male patients, and n = 77 female patients) who underwent laparoscopic sleeve gastrectomy, intraperitoneal bupivacaine administration provided adequate analgesia in the first 6 hours after surgery. 11 In another randomized controlled study examining the efficacy of intraperitoneal administration of bupivacaine after bariatric surgery, significant differences of the VAS scores of the patient (n = 20 male patients, and n = 86 female patients) were found between the control group at 2nd, 4th, and 6th hours. 15 Kahokehr et al. conducted a meta-analysis of intraperitoneal local anesthetic infusion in patients undergoing laparoscopic gastric surgery, reporting effectively reduced postoperative abdominal pain, shoulder pain, and narcotic use. 16
Furthermore, in a prospective, randomized-controlled clinical study of patients (n = 35 male patients, and n = 75 female patients) who underwent bariatric surgery conducted by Ruiz-Tovar et al., continuous intraperitoneal local anesthetic infusion through a catheter significantly reduced postoperative abdominal and shoulder pain, shortened the length of hospital stay, reduced narcotic use, and promoted early mobilization and oral intake of fluids. 17 Consistent with these studies, our study showed that significant differences of VAS scores were found between the study group (n = 34) and the control group (n = 34) at the 2nd, 4th, and 6th hours in patients (P < .05, P < .05, P < .01, respectively) (Fig. 1).
According to the studies of PB Ali and BR Pamuk, local anesthetic was administered to the pelvic cavity after total abdominal hysterectomy in 60 female patients, however, there were no significant differences found between local anesthetic group and control group. 18 Bupivacaine administration does not significantly lower VAS scores of female patients (n = 15) after laparoscopic surgery compared with the control group (n = 16). 19 Intra-abdominal local anesthetics in many gynecological surgeries do not provide effective analgesic postoperatively.19–23 In consistence with these studies, our study shows that no significant differences of VAS scores of female patients were found between the study group (n = 20) and the control group (n = 17) at the 2nd, 4th, and 6th hours (Fig. 3).
Conclusion
Overall, our study showed that male patients in the study group had significantly lower VAS scores compared with the male patients in the control group at the 2nd, 4th, and 6th hours. Interestingly, there were no significant differences in VAS score of female patients between the study group and control group. These findings suggest that bupivacaine is more effective in managing postoperative pain in male patients undergoing bariatric and metabolic surgery. Our results indicate that there is a gender-related difference in the response to intraperitoneal local anesthetic administration. There may be various reasons to explain gender-related differences in the response to intraperitoneal local anesthetic administration, such as, (1) gender differences in neurohormonal nociception, (2) psychological factors, (3) social/cultural factors, (4) geographical conditions etc. To understand the background of our findings, further studies should be conducted in various perspectives of gender differences such as in neurohormonal nociception, psychological factors, social/cultural factors, and geographical conditions.
Footnotes
Acknowledgments
The authors thank the Istanbul Aydin University Anesthesia and Reanimation Department and surgical personnel for providing assistance in this clinical study.
Authors' Contributions
S.B., and H.A. were involved in conceptualization, design study, and writing in the first draft of the article. S.B., and B.K. were involved in data acquisition. Y.E.A. and M.O. were involved in data analysis, interpretation, and writing the final draft of the article. All authors reviewed and approved the final article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.