
Abstract
Background:
Data on the outcomes of laparoscopic fundoplication (LF) in patients with ventriculoperitoneal (VP) shunts are limited.
Materials and Methods:
We retrospectively evaluated the demographic characteristics and outcomes of patients who underwent LF at our institutions between 2014 and 2022. Then, we systematically reviewed articles in MEDILINE/PubMed, Cochrane Library, and Web of Science.
Results:
There was no significant difference in terms of the outcomes between patients with VP shunt (n = 10) and those without (n = 96) at our institutions. None of the patients presented with shunt trouble after LF. The meta-analysis included four retrospective studies and our institutional data. In total, 605 patients (55 with VP shunt) underwent LF. Furthermore, 2 (3.6%) of 55 patients (1 with infection and 1 with occlusion) had shunt troubles. The conversion and complication rates, operative time, and length of hospital stay did not significantly differ between patients with VP shunt and those without.
Conclusions:
LF can be safely performed on children with VP shunts and is associated with a low risk of shunt troubles. The Clinical Trial Registration number is 2022-387.
Introduction
Laparoscopic fundoplication (LF) is one of the most common minimally invasive procedures for severe gastroesophageal reflux disease (GERD).1,2 A significant number of patients with GERD present with neurological impairment, and they may have previously required surgical treatment, including ventriculoperitoneal (VP) shunt implantation, which is the standard treatment option for patients with hydrocephalus. 3
The presence of VP shunt is associated with complications such as shunt infection and occlusion and increased operative complexity in patients who undergo LF. However, data on the outcomes of LF in patients with VP shunt are limited. Moreover, to the best of our knowledge, there is no published systematic review and meta-analysis on this subject. First, this study aimed to retrospectively analyze the surgical outcomes of patients with VP shunt who underwent LF. Second, a systematic review was conducted to evaluate all published studies on the outcome of patients with VP shunt who underwent LF. Finally, a meta-analysis on patient outcomes and surgical risks was performed.
Materials and Methods
Retrospective study
The medical records of patients who underwent LF at three institutions between January 2014 and October 2022 were retrospectively reviewed. The indications for LF included GERD symptoms and a low esophagus pH <4 for >4% within a 24-hour cycle. Patients who previously underwent gastrostomy were excluded.
We recorded data on the demographic and clinical characteristics of patients. These included sex, age, and body weight at the time of LF, previous history of abdominal surgery, and surgical parameters (operative time, volume of blood loss, and complication and recurrence rates). The surgical parameters of patients with VP shunt and those without were compared. The following indwelling VP shunt catheters were used: CODMAN HAKIM, CODMAN CERTAS, Pro GAV, and PUDENZ. All shunt systems were standardized with no-reflow valves, which can withstand up to 50 cm H2O. The VP shunt catheter was clamped intraoperatively based on the discretion of the neurosurgeon performing the surgery at the institution. Furthermore, the incidence rate of shunt trouble (infection and occlusion) after LF was investigated. Recurrence was determined according to upper gastrointestinal findings and history of rehospitalization due to GERD symptoms.
Laparoscopic fundoplication
We performed LF with a complete 360° wrap according to Nissen or a partial 270° wrap based on Toupet, which is a standardized procedure previously described by our institution. 4 In Toupet, the wrap was formed with six stitches.
The VP shunt catheter was placed in the right abdomen. Hence, the right-most port was shifted to either side to avoid the catheter. The pneumoperitoneum pressure ranged from 6 to 10 mmHg of carbon dioxide according to patient size. Gastrostomy was performed according to the patient's need after fundoplication.
Postoperative management
Postoperative management was similar among three institutions. All patients received prophylactic antibiotics. Enteral nutrition was started within 3 days after surgery, and the dose was gradually increased. If the nutritional dose was sufficient and the family had mastered the technique of nutritional administration, the patient was discharged.
Systematic review and meta-analysis
We reviewed articles in MEDILINE/PubMed, Cochrane Library, and Web of Science using different combinations of the following terms: “laparoscopy,” “fundoplication,” “Nissen,” and “ventriculoperitoneal shunt.”
Selection criteria
Original articles reporting the outcomes of patients with VP shunt who underwent LF were included in the analysis. Two reviewers independently scanned the titles and abstracts of articles. The exclusion criteria were as follows: (1) Articles not written in English, (2) nonoriginal articles (case reports or case series, meeting abstract, and reviews), (3) studies that did not focus on patients with VP shunt who underwent LF, and (4) studies without insufficient outcome data on patients with VP shunt who underwent LF. This systematic review was based on the PRISMA principles.
Data extraction
Two reviewers separately collected the following data from the selected articles: the first author, year of publication, study design, sample size, operative time, length of hospital stay, complications, and shunt trouble after LF. Two reviewers reached a consensus at each stage of the data extraction process.
Statistical analysis
Continuous variables were presented as medians and interquartile ranges and categorical variables as frequencies and percentages. The Fisher's exact test and the Mann–Whitney U test were used to evaluate categorical and continuous variables, respectively. P < .05 was considered statistically significant.
Odds ratios (OR) were calculated using the Mantel–Haenszel method, and the 95% confidence interval (CI) was established. Statistical heterogeneity was quantified using I2. Strong heterogeneity was defined as an I2 score of >75%. Review Manager 5.4 was used to perform statistical analysis.
The ethics board of our institution approved this study (Approval No.: 2022055). Informed consent to participate in the study was obtained from the parents of all individual participants by disclosing the study information and giving those who did not wish to participate an opportunity to request it (opt out).
Results
Retrospective study
During the study period, 106 patients underwent LF (Nissen, n = 92 and Toupet, n = 14) at three institutions. Among them, 10 had a VP shunt during surgery. The median duration from VP shunt implantation to LF was 20 months (range: 2 months to 16 years). In 6 cases at 1 institution, the neurosurgeon temporarily clamped the VP shunt during LF. After a skin incision was made over the catheter on the right anterior thoracic region, the catheter was clamped with the atraumatic forceps. The clamp was released after the pneumoperitoneum. In 4 cases at 2 institutions, the shunt tube was not clamped. The median follow-up period was 5 years (range: 4 months to 17 years).
Table 1 shows the demographic and clinical characteristics of patients who underwent LF. The patients did not significantly differ in terms of age, body weight during surgery, and previous history of abdominal surgery. Patients with VP shunt had a significantly higher incidence of neurological impairment and scoliosis than those without.
Characteristics of Patients Who Underwent Laparoscopic Fundoplication With and Without Ventriculoperitoneal Shunts
Values are present as n (%) or median (interquartile range).
Bold value indicates significant difference.
LF, laparoscopic fundoplication; VP, ventriculoperitoneal.
Table 2 shows the surgical parameters of 106 patients. The operative time, volume of blood loss, and rate of conversion to open surgery did not differ between patients with VP shunt and those without. One patient without VP shunt required conversion to open surgery because of a large hiatal hernia. There was no significant difference in the postoperative course (length of hospital stay and complication and recurrence rates) between patients with VP shunt and those without. None of the patients presented with shunt trouble (infection or occlusion) after LF.
Comparison of Outcomes Between Patients With and Without Ventriculoperitoneal Shunts at Laparoscopic Fundoplication
Values are present as n (%) or median (interquartile range).
DGE, delayed gastric emptying; EN, enteral nutrition; LF, laparoscopic fundoplication; VP, ventriculoperitoneal.
Systematic review and meta-analysis
In total, 246 articles were identified through a comprehensive review. There were 105 duplicates, and 137 records were removed based on the exclusion criteria. Four retrospective observational studies met the inclusion criteria.3,5–7 Finally, these four studies and our institutional data were evaluated using a meta-analysis. Figure 1 shows the flow diagram, and Table 3 depicts the included studies. Our study included 605 patients, and 55 of whom with VP shunt underwent LF. In total, 2 (3.6%) of 55 patients (1 with infection and 1 with occlusion) had shunt troubles.

PRISMA flowchart.
Characteristics of Studies Included in Meta-Analysis
The patient with ventriculoperitoneal shunt who underwent laparoscopic fundoplication.
Con, control; LOS, length of hospital stay; OCT, operation time; ROS, retrospective observational study; SD, standard deviation; VP, ventriculoperitoneal.
Three studies reported the rate of conversion to open surgery (Table 3). In total, 2 (7.4%) of 27 patients with VP shunt and 7 (1.6%) of 445 patients without VP shunt underwent LF that required conversion to open surgery. There was no significant difference between the two groups (pooled OR = 4.11, 95% CI: 0.81–20.95, P = .89, I2 = 0%; Fig. 2a).
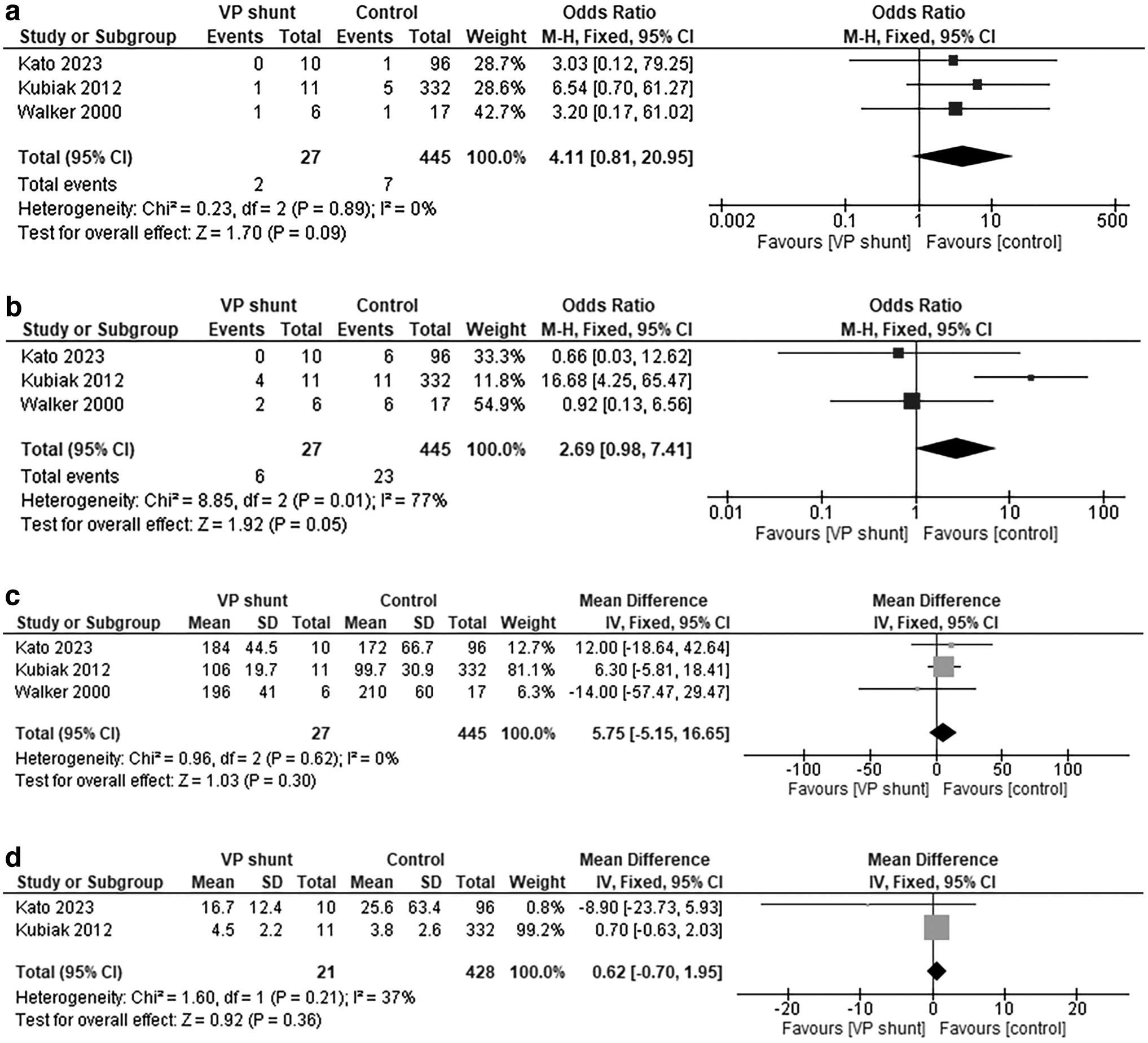
Three studies reported the rate of surgical complications (Table 3). In total, 6 (22%) of 22 patients with VP shunt and 23 (5.2%) of 445 patients without VP shunt underwent LF that required conversion to open surgery. There was no significant difference between the two groups (pooled OR = 2.69, 95% CI: 0.98–7.41, P = .05, I2 = 77%; Fig. 2b).
Three studies reported the operative time of LF (Table 3). Results showed no significant difference in terms of operative time between the two groups (pooled OR = 5.75, 95% CI: −5.15 to 16.65, P = .30, I2 = 0%; Fig. 2c).
Two studies reported the length of hospital stay (Table 3). Results showed no significant difference in terms of length of hospital stay between the two groups (pooled OR = 0.62, 95% CI: −0.70 to 1.95, P = .36, I2 = 37%; Fig. 2d).
Overall, there was no significant difference in terms of conversion and complication rates, operative time, and length of hospital stay between patients with VP shunt and those without.
Discussion
First, the medium-term outcomes of 10 patients with VP shunt and 96 patients without VP shunt who underwent LF were compared. There was no significant difference in terms of the surgical parameters and postoperative course. Moreover, there was no shunt trouble associated with LF. Based on the systematic review and meta-analysis, the conversion and complication rates, operative time, and length of hospital stay did not significantly differ between patients with VP shunt and those without.
Less invasive techniques are required for abdominal surgery in pediatric patients. The benefits of laparoscopy include less postoperative pain, shorter length of hospital stay, and better cosmesis.8,9 These benefits are especially important if patients with VP shunt can safely undergo LF, who have a variety of comorbidities. Laparoscopic surgery is not associated with an increased incidence of postoperative complications in patients with VP shunt. 10
Several retrospective studies reported that LF was feasible in children with a previous history of VP shunt placement.3,5–7 In these studies, complication and shunt trouble were assessed at a median of 18 months at the longest. However, the median follow-up period in this study was 5 years, which was longer than that in previous studies. Hence, LF can be safely performed on children with VP shunt, and there is no risk of medium-term shunt trouble.
Previous studies showed that patients with VP shunts presented with LF complications.5,7 These included cellulitis at the gastrostomy site, pelvic hematoma, adhesion resulting in bleeding from the omentum, and colon perforation during gastrostomy insertion. There was no significant difference between patients with VP shunt and those without in terms of LF complications.5,7 Although the complications were not attributed to the presence of VP shunt, the abovementioned complications should be considered in LF.
At our institutions, some patients with a history of other types of laparotomy gastrointestinal tract surgeries had moderate to severe postoperative adhesions. However, patients with VP shunt had minimal or no adhesion. In this study, one port is shifted to prevent shunt tube damage to either side in LF, and this is the only difference between LF and the common fundoplication procedure. None of the patients with VP shunt experienced conversion to open surgery and presented with complications.
There was no significant difference in terms of operative time, volume of blood loss, and recurrence rate. Laparoscopic techniques are associated with a better field of view and access to the esophagogastric junction in patients with scoliosis who have VP shunt. Moreover, our meta-analysis showed no significant difference in the conversion and complication rates, operative time, and length of hospital stay between patients with VP shunt and those without. Hence, LF can be feasible with minimally invasive surgery in patients with VP shunt.
However, pneumoperitoneum may cause shunt trouble (occlusion or infection). Most VP shunt catheters are routinely equipped with no re-flow valves. An in vitro study found that no disruption of the VP shunt with a check valve at a pressure of <350 mmHg. 11 Another study revealed that laparoscopic surgery with pneumoperitoneum pressure ranging from 3 to 25 mmHg could not cause retrograde reflux. 12 Theoretically, intraoperative catheter manipulation, including the clamp, is not necessary. However, there were a few reports about laparoscopic-induced pneumocephalus, shunt infection, and occlusion.3,13,14
The check valve could have been initially defective. However, it is challenging to identify before surgery. It can be clamped according to the neurosurgeon's preference. At our institution, 6 patients had intraoperative VP shunt clamping to prevent serious complications caused by the pneumoperitoneum. Furthermore, none of the patients presented with postoperative catheter injury. Therefore, shunt tube clamping can be acceptable in rare cases of shunt troubles.
Our study had several limitations. First, all eligible studies on patients who underwent LF were retrospective and nonrandomized in nature. A prospective study may provide additional insights into the safety and efficacy of LF in patients with VP shunt. Second, the sample size was small. Nevertheless, large, high-quality randomized controlled trials should be conducted in the future.
Conclusions
Although the sample size was small, the presence of VP shunts did not significantly affect operative time and complication and recurrence rates. There was no case of shunt occlusion or infection caused by LF. Theoretically, it is not necessary to clamp the shunt, but some neurologists believe that shunt clamping is less likely to cause serious complications caused by the pneumoperitoneum. Therefore, we can respect the judgment of the physician managing VP shunt to clamp the shunt or not. Moreover, the conversion and complication rates, operative time, and length of hospital stay did not significantly differ between patients with VP shunt and those without based on a meta-analysis. Therefore, LF can be safely performed on children with VP shunts and is associated with a low risk of shunt troubles.
Footnotes
Authors' Contributions
D.K. planned and conducted the study, collected and interpreted the data, and wrote the article. D.K. and T.T. extracted and analyzed the data. H.U. interpreted and critically reviewed the article. All authors approved the final draft of this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.