
Abstract
Background:
Ventilating a pediatric patient during thoracoscopy is challenging. Few studies have highlighted the impact of capnothorax in children by measuring regional cerebral oxygen saturation (rcSO2) with near infrared spectroscopy. In this systematic review, we aimed to summarize the data from relevant studies and assess whether thoracoscopy in children is associated with intraoperative pathological cerebral desaturation.
Methods:
The authors systematically searched four databases for relevant studies on the measurement of rcSO2 during pediatric thoracoscopic procedures. The primary outcome was the proportion of patients with pathological desaturation, that is, >20% decline in the intraoperative rcSO2. Risk of bias among the included studies was estimated using the Newcastle–Ottawa scale.
Results:
The systematic search resulted in 776 articles, of which 7 studies were included in the analysis. In total, 88 patients (99 procedures) with an age ranging from 0 days to 8.1 years were included. Of these, 43 (49%) patients were neonates. The included cohort had esophageal atresia and tracheoesophageal fistula (n = 26), long-gap esophageal atresia (n = 5), congenital diaphragmatic hernia (n = 14), and congenital pulmonary airway malformations and other conditions needing lung resection (n = 43). Of the total 99 procedures, pathological desaturation was noticed in 13 (13.1%, 95% confidence interval 7.2–21.4) of them. Upon quality assessment, most of the studies were weaker in the selection and comparability domains.
Conclusion:
In this review, pathological cerebral desaturation was noticed in 13.1% of the pediatric thoracoscopic procedures. However, due to limited methodological quality of the included studies, further randomized multicentric studies comparing rcSO2 in open versus thoracoscopic surgeries are needed to derive definitive conclusions.
Introduction
The uptake of minimally invasive surgery in the pediatric age group has been gradual, due to challenges of miniaturization of surgical instruments, a steep learning curve, and the development of safe and reliable techniques of pediatric anesthesia. 1 Over the years, thoracoscopic surgeries in children including repair of esophageal atresia–tracheoesophageal fistula (EA–TEF), repair of congenital diaphragmatic hernia (CDH), and lobectomies for disorders such as congenital pulmonary airway malformations (CPAMs) have become common in specialized pediatric surgical centers. 2
A major challenge in pediatric minimally invasive procedures is achievement of adequate ventilation. Carbon dioxide (CO2) can be absorbed in the circulation during insufflation into the chest and creation of the capnothorax. It can cause significant metabolic and physiological perturbations including right-to-left shunting, decreased venous return and cardiac output, and systemic hypertension or hypotension. Furthermore, the associated lung collapse and, at times, the use of single lung ventilation can impair oxygenation and CO2 elimination. These factors, in consonance, culminate in an increased end-tidal CO2 during thoracoscopic procedures. 3
In neonates, the potential impact of CO2 pneumothorax and collapse or reduced ventilation of the ipsilateral lung in an immature (and often diseased) neonatal cardiopulmonary system is a major concern. Severe acidosis and hypercarbia can compromise the cerebral circulation.4,5 It is possible that cerebral hypo- and hyperperfusion due to rapid CO2 shifts during thoracoscopic surgery can cause adverse long-term neurodevelopmental outcomes.
A few studies have attempted to throw light on this aspect through the measurement of intraoperative regional cerebral oxygen saturation (rcSO2) using techniques such as near infrared spectroscopy (NIRS) and oxygen to see (O2C).5,6 NIRS is a noninvasive method of in vivo monitoring of rcSO2. The NIRS monitor gives a venous-weighted measurement of oxyhemoglobin. In addition, rcSO2 provides information about the oxygen demand, oxygen extraction, and oxygen reserve of the underlying tissue. 5
Previously published studies have demonstrated that thoracoscopy in neonates and children can lead to severe hypercapnia and acidosis intraoperatively. Even if rcSO2 remains within clinical acceptable limits during periods of acidosis, pathological desaturation of >20% can occur in a certain number of patients.6,7 This review aims to systematically evaluate such studies and assess the effect of thoracoscopic surgery on rcSO2 using NIRS in the pediatric population.
Materials and Methods
Search strategy
A preliminary search was independently performed by 2 authors (G.P. and A.S.) in the PubMed database to identify prior systematic reviews and meta-analyses on the topic. Subsequently, both the authors conducted a systematic search in PubMed, Web of Science, Scopus, and EMBASE databases during February 2023. The search terms used were “Thoracoscopy OR Video assisted Thoracoscopic Surgery OR VATS OR Minimal Access Surgery OR Minimally Invasive Surgery” AND “cerebral oxygenation OR cerebral hypoxia OR cerebral hypercarbia OR cerebral saturation” AND “Near Infra-red Spectroscopy OR NIRS.” Duplicates were removed and references were screened for inclusion in the review. A detailed electronic search strategy is described in Supplementary Table.
Eligibility
All studies with patients <18 years of age who underwent thoracoscopic surgery and where intraoperative rcSO2 was measured using NIRS were included in this review. Both prospective and retrospective study designs were included. Case reports, opinion articles, letters to the editor, and correspondences were excluded. Also, studies including animal subjects and those in languages other than English were excluded. If a study provided sufficient information regarding the proportion of patients with a decrease in intraoperative rcSO2, it was included in the quantitative synthesis.
Data extraction
Two authors (G.P. and A.S.) independently screened the references and retrieved full texts of the selected articles. Any discrepancies were resolved through mutual consensus and referring back to the source. Information was extracted regarding the number of included patients, age at surgery, type of surgical procedure performed, intraoperative partial pressure of CO2 (pCO2) measured through arterial blood gas sampling, and rcSO2 levels. The primary outcome was the proportion of patients with >20% decline in the intraoperative rcSO2. A 20% decline was chosen as “pathological,” based on the guidance from relevant studies.6,7 Individual authors were contacted for relevant details, in case of incomplete information.
Statistical analysis and assessment of bias
Categorical variables are depicted as proportions and continuous variables are depicted as median with range. The included studies were graded for risk of bias using the Newcastle–Ottawa scale. 8 Two authors (S.A. and D.K.) independently assessed the methodological quality. Any dispute was resolved through consensus or by discussion with a third author (P.K.).
Results
A total of 776 articles were screened (Fig. 1). After excluding 767 studies based on predefined exclusion criteria, 9 studies were found eligible for the full-text review.1,5–7,9–13 One study was excluded after full-text review screening as it primarily focused on hypercapnia and acidosis during thoracoscopic surgery and did not report data on rcSO2.1,6 Another study was excluded because it utilized O2C for measuring rcSO2 rather than NIRS. Finally, seven studies were included in the quantitative analysis.5,7,9–13
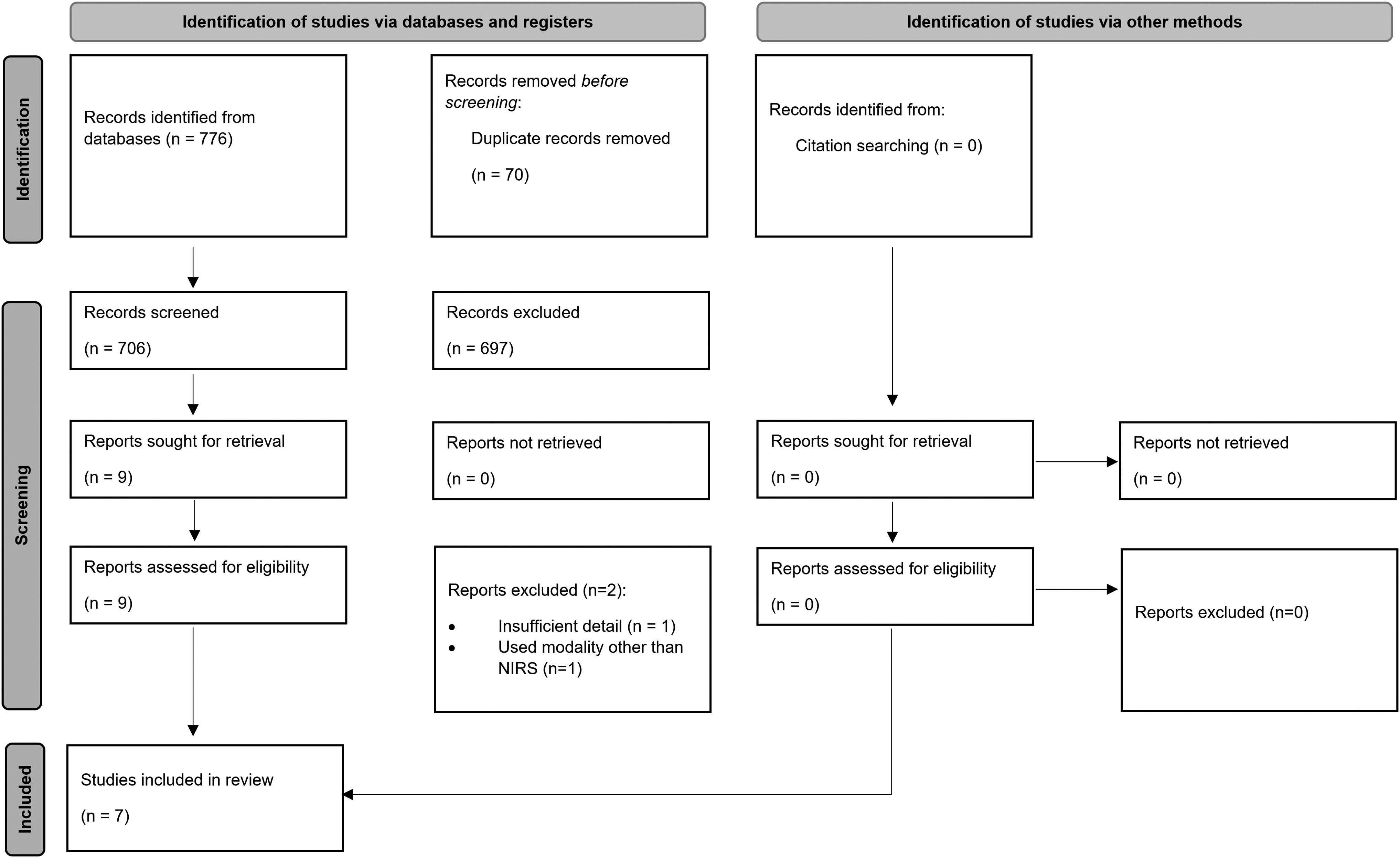
Selection of the relevant studies using the PRISMA flow diagram. NIRS, near infrared spectroscopy; PRISMA, Preferred Reporting Items for Systematic Review and Meta-Analysis.
The characteristics of the included studies are depicted in Table 1. All the full-text articles included in the analysis were contributed by authors from high-income countries. A total of 88 patients were included in 7 studies. Ninety-nine surgical procedures were performed on 88 patients. All the studies were conducted as a prospective cohort design. The earliest study could be traced back to 2011. The age at presentation ranged from 0 days to 8.1 years, with 48% of the patients being neonates (n = 43).
Characteristics of the Included Studies
CDH, congenital diaphragmatic hernia; EA–TEF, esophageal atresia–tracheoesophageal fistula.
The indication for surgery (Table 2) was predominantly EA–TEF (26 patients, 29.5%). Other conditions included long gap esophageal atresia (5 patients, 5.6%), CDH (14 patients, 15.9%), and CPAM and lung resections for other conditions (43 patients, 49%). The mean (range) duration of the surgeries mentioned in the included studies was 189.05 (55–521) minutes.
Procedures Undertaken in the Patients
Data for intraoperative values of rcSO2 were available for 42 patients who underwent 53 procedures.5,10–12 The rcSO2 values ranged from 55% to 90% in these patients. In addition, three studies provided the data for the proportion of patients with pathological cerebral desaturation.7,9,13 Of the total 99 procedures performed in 88 patients, 13 (13.1%, 95% confidence interval 7.2–21.4) had a pathological cerebral desaturation during thoracoscopy.
The values of intraoperative pCO2 were available for 78 of 88 patients. The mean (range) pCO2 of these patients was 72.6 (36.5–195) mm Hg. Two studies by Bishay et al. 5 and Costerus et al. 12 reported significant hypercarbia with average pCO2 values of 93 and 135 mm Hg, respectively.
Upon utilizing the Newcastle–Ottawa scale (Table 3), only two studies demonstrated compliance to all items within the selection domain.7,9 Although the included studies were weaker in the comparability domain, outcome category was adequately presented in all of them.
Methodological Quality Assessment Utilizing the Newcastle–Ottawa Scale
In each study, * denotes adequate description of the particular numbered item within that specific domain. A maximum of one * /item can be awarded for the selection and outcome domains. For the comparability domain, a maximum of two * can be awarded.
Discussion
Minimally invasive surgeries are being increasingly performed in the pediatric age group. Although early studies concentrated on technical aspects (working space, instruments, and complications), recent reports have started focusing on the functional and physiological parameters, particularly the cerebral pathophysiology.4,5
Thoracoscopic approach for anomalies such as EA–TEF, CDH, diaphragmatic eventration, and CPAM offers numerous benefits including decreased postoperative pain, decreased respiratory impairment, shorter hospital stay, and better overall cosmesis with a minimal risk of long-term orthopedic deformities such as scoliosis.2,14 However, concerns have been raised regarding its safety, pertaining to the impact of applied pressurized pneumothorax on hemodynamics and organ perfusion in children. 15 This has particularly been emphasized in neonates, owing to their immature and pathological cardiopulmonary system. 10
Pneumothorax is created during thoracoscopy to increase the working space in the chest by collapsing or reducing the ventilation of the ipsilateral lung. CO2 is used for this purpose since it is noncombustible, inexpensive, and least likely to cause air embolism. However, intrathoracic CO2 insufflation collapses the lung that adversely affects the gas exchange leading to hypoxia and hypercarbia. These factors along with the acidosis cause vasodilatation of the cerebral vessels. When lower arterial oxygen saturation causes a decrease in the cerebral blood supply, the hypercarbia-induced vasodilatation can compensate for the reduced cerebral oxygen supply.16–18
Thus, thoracoscopy in the pediatric age group (particularly neonates) is often complicated by a combination of CO2 absorption and ventilation–perfusion (V/Q) mismatch.5,19 The hypercapnia and acidosis associated with it can affect cerebral circulation. Classical parameters such as heart rate, blood pressure, arterial oxygen saturation, and end-tidal CO2 reflect the general condition of the patient during surgery. In a study by Neunhoeffer et al., 6 peripheral arterial oxygen saturation remained within normal limits during periods of decreased cerebral oxygen saturation measured by laser Doppler flowmetry.
Outliers in cerebral oxygen oxygenation may pose a risk for brain injury in the developing neonatal brain. The same has been demonstrated in cardiac patients undergoing major neonatal surgery, in whom a high percentage of de novo brain injury has been detected postoperatively on magnetic resonance imaging.5,20 This underscores the importance of measuring rcSO2 intraoperatively by methods such as NIRS.
NIRS is a noninvasive method of measuring and monitoring changes in the regional hemoglobin oxygen saturation in the blood. Since hemoglobin in the sensor's field is made up of ∼75% venous blood, 20% arterial blood, and 5% capillary blood, the readings mainly reflect oxygen saturation. 5 NIRS is widely used in pediatric cardiac surgery and adult aortic surgery to assess perioperative cerebral oxygen saturation. 21 The studies identified by our systematic search show that its use can be extended to pediatric thoracoscopic surgery as well.
The normal range of arterial pH is generally taken as 7.35–7.45, and arterial pCO2 as 35–45 mm of Hg. In children with CDH, arterial pH >7.20 and arterial pCO2 between 50 and 70 mm of Hg (6.9–9.3 kPa, permissive hypercapnia) are acceptable. 22 In this review, the mean (range) pCO2 of 78 of 88 patients was 72.6 (36.5–195) mm of Hg. Two studies demonstrated significant hypercarbia during thoracoscopy.5,12 Moreover, the compilation of results showed that 13.1% of the 99 procedures (in 88 patients) demonstrated a pathological fall in rcSO2. Analyzing the results of the individual studies, it was found that in most of these cases, intraoperative cerebral oxygenation remained within the safety range (55%–85%).
The studies included in this review highlight the importance of close monitoring and collaboration between neonatologists, anesthesiologists, and pediatric surgeons to achieve stable physiological condition with sustained brain oxygenation levels. Fluid expansion and inotropic support instituted by the anesthetist prevent blood pressure from declining below the physiological limits during thoracoscopy. In the study by Tytgat et al., 18 to allow adequate ventilation, CO2 insufflation was stopped for brief intervals of time intraoperatively.
This was done to avoid any hemodynamic instability during the procedure. A recent experimental study in piglets showed that 10 mm Hg of pneumothorax pressures cause severe hemodynamic instability and decreased cerebral perfusion, whereas these parameters remained stable with pneumothorax pressures of 5 mm of Hg. 23 Thus, it is essential to have an experienced operating team, particularly the anesthesiologist, during pediatric thoracoscopy. The anesthesiologist must have specific experience in managing fluctuations in rcSO2 during the procedure.
The findings of this review must be interpreted within the context of a few limitations. First, only seven studies were eligible for inclusion in this systematic review. Additional studies with a larger sample size are required to confirm the results reported so far. Second, the included studies had variable reporting of the data on rcSO2. Four of them depicted the actual values of intraoperative rcSO2 whereas three studies only provided the data on the proportion of patients with pathological cerebral desaturation.
Third, this review is limited by its ability to determine whether the observed effects have any correlation with the neurodevelopmental outcomes. Future studies focusing on the long-term follow-up need to be conducted. Fourth, there is a paucity of literature on the comparison of rcSO2 values among newborns who have undergone thoracoscopy versus open thoracotomy. Although this would be technically difficult because choosing the open approach only for scientific comparison does not comply with the ethical standards, however, future randomized controlled trials on this subject would provide an ideal comparison between the two surgical approaches in terms of intraoperative rcSO2.
Finally, unit specific variations in anesthesia regimens (such as hemodynamic optimization and respiration) can also confound the reported results. A detailed information on these factors is needed before any definite conclusions are drawn in this regard.
Conclusion
When performed by an experienced operating team, thoracoscopic surgeries are considered safe in children. Application of NIRS to monitor cerebral oxygenation can provide valuable information on the physiological effects of pediatric thoracoscopy. We found that 13.1% of the patients showed pathological cerebral desaturation during thoracoscopy. Owing to limited methodological quality of the included studies, further randomized multicentric studies are needed to derive definitive conclusions.
Footnotes
Authors' Contributions
S.A. and D.K. contributed to study conception and design. Data acquisition was done by G.P., A.S., and P.K. Analysis and interpretation of data were done by G.P., A.S., S.A., D.K., and P.K. Drafting of the article was performed by G.P., A.S., and D.K. Article was revised by S.A. and P.K. The final draft of the article was read and approved by all the authors. S.A. acts as the guarantor of this article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.