
Abstract
Background:
The aim of this study was to examine the feasibility and safety of the single-incision laparoscopic percutaneous extraperitoneal surgery for the treatment of incarcerated indirect inguinal hernia in children.
Methods:
Seventy-five patients who presented with incarcerated indirect inguinal hernia and underwent laparoscopic surgery from January 2019 to January 2022 in Children's Hospital, Zhejiang University School of Medicine were retrospectively analyzed. The data were collected including the clinical information of the patients, perioperative details, and postoperative outcomes.
Results:
The median age of these patients was 21 months with a median weight of 9 kg. Among these 75 patients, the herniated contents of 73 patients were pushed back successfully with external manual pressure under the monitoring of laparoscope, then we did the hernia sac high ligation by using fascial closure device. After successful reduction, three cases developed incarcerated intestine necrosis, we enlarged the umbilical incision, dragged out the necrotic intestine, and did parallel resection and anastomosis. Only in two patients, it was difficult to push back the herniated organ; therefore, these patients were converted to traditional open surgery. The average length of postoperative hospital stay for the patients who didn't get incarcerated organ necrosis was 2 days. All patients recovered very well; there was no recurrence of the hernia and any other postoperative complications.
Conclusions:
Single-incision percutaneous extraperitoneal laparoscopic surgery for the treatment of incarcerated indirect inguinal hernia in children appears to be safe and feasible. Our experience shows that it is recommended to perform laparoscopic surgery for incarcerated indirect inguinal hernia in children.
Introduction
Incarcerated indirect inguinal hernia is one of the most common emergencies in children, 1 if the hernia cannot be reduced manually, or has incarcerated for >12 hours, the groin exploration surgery will be performed. With the development of laparoscopic technology, the application of laparoscopic surgery in the treatment of incarcerated indirect inguinal hernia in children is becoming increasingly common nowadays 2 ; it has the advantages of small trauma and fast recovery for the patient. In this study, we performed a retrospective analysis to show our experiences in single-incision laparoscopic extraperitoneal procedure for the patients presenting with incarcerated indirect inguinal hernia.
Materials and Methods
Patients
A retrospective analysis was conducted on 75 patients with incarcerated indirect inguinal hernia who underwent laparoscopic high ligation of hernia sac at the Children's Hospital of Zhejiang University School of Medicine from January 2019 to January 2022. The study was approved by the institute of ethics committee (No. 2023-IRB-0135-P-01). The laparoscopic surgery indications for the patients were as follows: (1) incarcerated for >12 hours; (2) manual reduction failed; and (3) obvious local redness and swelling of groin.
Surgical procedures
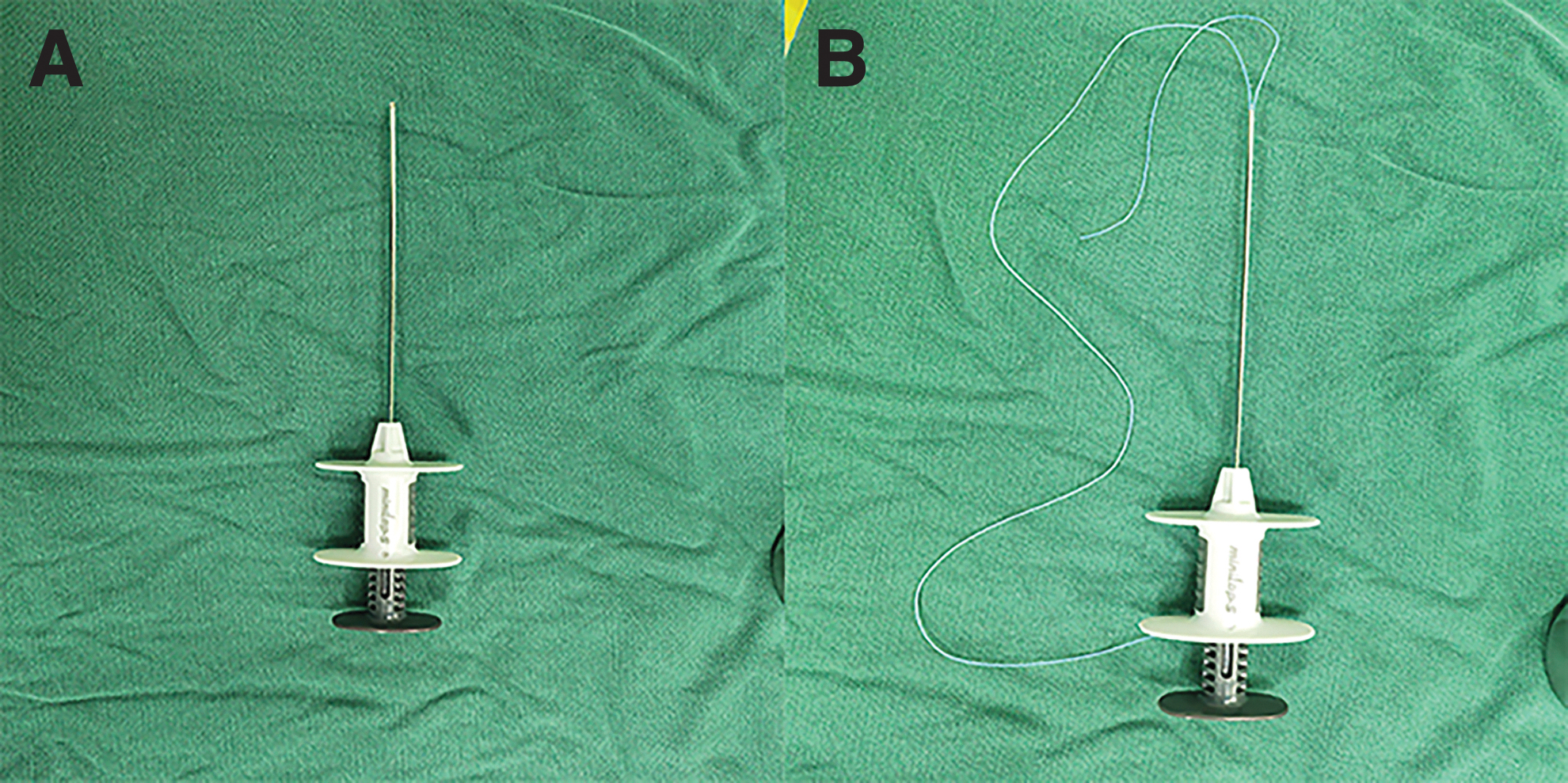
Placing the patient in a supine position, general anesthesia was performed with tracheal intubation, and a 5 mm Trocar was inserted through the umbilical incision that serves as a port for the 30° laparoscope. After that the operating table was adjusted to the low head and high feet posture, and the fascial closure device carrying 2/0 unabsorbable suture was used to ligate the inner ring (Fig. 1A, B).
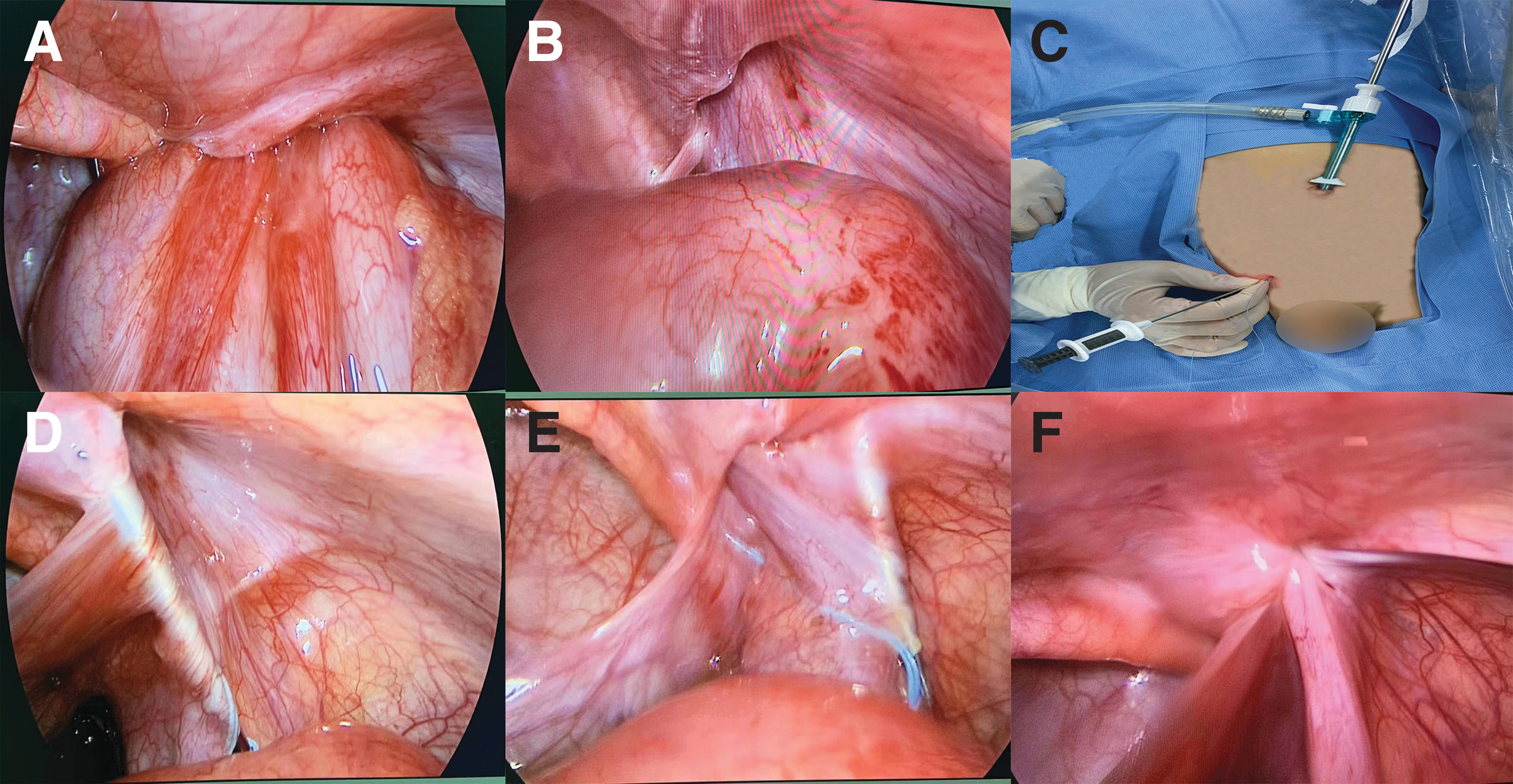
Manual reduction of the incarcerated hernia contents under laparoscopic monitoring was performed (Fig. 2A). After successful reduction (Fig. 2B), the projection point on the body surface of the midpoint of the inner ring as the operation point (Fig. 2C) is taken, inserting the fascial closure device until the preperitoneal space, wrapping deep ring around half a circle, piercing the peritoneum, and leaving the end of the suture within the peritoneum cavity (Fig. 2D). Then the fascial closure device was slowly withdrawn until its tip reached the preperitoneal space of the deep ring and again encircled another half circle of the deep ring in the preperitoneal space until the previous breach point was reached (Fig. 2E) (for the male patients, when encircling the deep ring, we needed to separate the testicular vessels and vas). If the inner ring was particularly large and was difficult to be encircled, an additional fascial closure device can be used to assist the operation. Then the suture end was retrieved out of the body, making a knot to ligate the deep ring (Fig. 2F).
Then we could assess the vitality of the reduced content and the situation of the contralateral deep ring. If the contralateral deep ring was also unclosed, we would use the same method to close it. For the reduced content, if it were necrotic, we would expand the navel incision and drag it out of the abdominal cavity and treat with resection and anastomosis.
Statistical analysis
Statistical analysis was done using SPSS 24.0. Frequency of continuous variables was reported as median and range. Mann–Whitney U test was utilized for continuous variables, and Pearson's chi-square and Fisher's exact tests were used for categorical variables. P values < .05 were considered statistically significant.
Results
A total of 75 patients (37 females and 38 males) were enrolled in the present study (Table 1). The median age of these patients was 21 months (range: 1–114 M) with a median weight of 9 kg.
Clinical Parameters of the Incarcerated Indirect Inguinal Hernia Patients
Among these patients, the incarcerated hernia contents of 73 patients were successfully pushed back with external manual pressure under the monitoring of laparoscope; then we did the laparoscopic percutaneous extraperitoneal hernia sac high ligation by using the fascial closure device for these patients. After successful reduction, the incarcerated intestine was necrotic in three cases, after which we performed intestinal resection and anastomosis through the enlarged umbilical incision. For two patients, pushing back the incarcerated hernia contents was difficult because of the serious swelling of the deep ring and incarcerated intestine; we then decided to do the open surgery for these patients. The median surgical time for laparoscopic percutaneous extraperitoneal hernia sac high ligation was 15 minutes. For intestinal resection and anastomosis, the median surgical time was 70 minutes, and the average length of postoperative hospital stay for the patients who didn't get incarcerated organ necrosis was 2 days. All of the patients recovered well without any complications.
Discussion
For incarcerated indirect inguinal hernia in children, it is difficult for parents to provide accurate incarcerated time. Sometimes the incarcerated part of the patient is obviously red and swollen; therefore, there is a high risk of manual reduction because we are not sure whether the incarcerated contents are necrotic. Therefore, in such cases laparoscopic surgery has obvious advantages. 3 We can perform manipulative reduction under laparoscopic monitoring, ligate the deep ring, and evaluate the viability of incarcerated contents, thereby avoiding the trauma caused to the patient by traditional open surgery. In addition, for the patients with failed manual reduction, after general anesthesia, their abdominal muscles are relaxed. The success probability of manual reduction will be much higher. If the incarcerated content is necrotic, we can perform further surgery by slightly expanding the umbilical incision.
Owing to the advantages of the laparoscopic surgery, there have been multiple studies on laparoscopic surgery for the treatment of incarcerated inguinal hernia.4–6 But these surgeries are all performed using multiple trocar holes. In this case, we attempted to use a fascial closure device (hernia needle) to complete the surgery and only required one trocar hole. First, in our experience, it is not advisable to use grasping forceps to pull the incarcerated hernia content back to the abdominal cavity to complete the reduction, as this can crush the incarcerated tissues. Second, if the inner ring is very large and is difficult to be encircled, we can insert another hernia needle to assist in the operation. Without the need for additional trocar holes, the position of the hernia needle can be selected at any point of the lower abdomen according to the surgeon's habits, and the wound is almost invisible after healing.
The occurrence of postoperative complications of traditional open surgery for incarcerated indirect inguinal hernia, such as edema of scrotum, hematoma, indirect hernia recurrence, is high. 7 Laparoscopic surgery has several advantages and include small operation incision, fast procedure, and efficient, quick recovery after surgey. 8 So the occurrence of postoperative complications is relatively low. In this study, all of the patients recovered very well after surgery, and there was no recurrence of the hernia and any other postoperative complications.
However, the limitations of this study are its retrospective nature and small sample quantity; so a larger multicenter prospective clinical trial and long-term follow-up is deemed necessary to validate the advantages of this technique.
Conclusion
Single-incision laparoscopic percutaneous extraperitoneal surgery for the treatment of incarcerated indirect inguinal hernia in children appears to be safe and feasible. Our experience shows that it is recommended to perform such surgery in children.
Footnotes
Authors' Contributions
M.H.: Data curation, Writing—Original draft preparation. J.X.: Conceptualization, Methodology, Formal analysis, Visualization. J.C.: Investigation, Software, Validation. X.Y.: Writing—Reviewing and Editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.